Vitiligo
Reading File
Finding Sources
Searching PubMed
vitiligo
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, multi-textbook content to deliver a thorough answer. Let me compile everything.
Vitiligo
Definition
Vitiligo is an acquired autoimmune disease of the skin characterized by well-defined, milky-white macules and patches resulting from T-cell-mediated destruction of epidermal melanocytes. Leukotrichia (white hairs) within lesions reflects concurrent loss of follicular melanocytes.
- Fitzpatrick's Dermatology, Ch. 76
- Dermatology 2-Volume Set 5e, Ch. 66
Epidemiology
- Prevalence: ~0.5-1% worldwide; up to >8% in parts of India
- Peak onset: ages 10-30 years; ~50% of cases begin before age 20
- No definitive sex predilection, though females seek care more often
- Can occur in bone marrow transplant recipients from donors with vitiligo (supports immune transfer)
- Monozygotic twin concordance only ~23%, supporting an important environmental/non-genetic component
Pathogenesis
The convergence theory unifies multiple pathogenic mechanisms:
1. Intrinsic melanocyte defects
Melanocytes in vitiligo patients have intrinsic abnormalities - they are more susceptible to oxidative stress, have dilated rough endoplasmic reticulum (unfolded protein response), and produce excess reactive oxygen species (ROS).
2. Cellular stress and danger signals
Stressed melanocytes release DAMPs - HSP-70 (heat shock protein 70) and HMGB1. These activate plasmacytoid dendritic cells and innate lymphoid cells to secrete IFN-α and IFN-γ.
3. Immune activation cascade
- Activated keratinocytes produce CXCL9 and CXCL10
- These recruit CD4+ helper and CD8+ cytotoxic T cells (which express CXCR3) to the skin
- CD8+ T cells produce IFN-γ and TNF, directly destroying melanocytes
- CD8+ T cells are both necessary and sufficient for melanocyte destruction
4. Resident memory T cells
Express CD69, CD103, CD49a and persist in previously affected skin, explaining why vitiligo recurs in the same areas after treatment.
5. Genetic factors
Multiple susceptibility loci identified. Key candidate genes are involved in melanogenesis, immune regulation, and apoptosis. ~7% of first-degree relatives of vitiligo patients are also affected. Many susceptibility genes are shared with other autoimmune diseases.
6. Chemical/environmental triggers
Phenolic compounds (e.g., industrial chemicals) act as tyrosine analogs and initiate the cellular stress response in melanocytes, exacerbating or inducing vitiligo.
Clinical Features
Lesion Characteristics
- Well-defined, milk-white macules/patches with smooth, convex margins
- Surrounding skin may appear normal or hyperpigmented (normal or hyperpigmented border)
- Trichrome vitiligo: intermediate tan zones between normal skin and fully depigmented areas (especially in early disease)
- Leukotrichia: white hairs within depigmented patches
- Rarely: inflammatory erythematous border (can mimic tinea corporis)
Clinical Types / Distribution
| Type | Description |
|---|---|
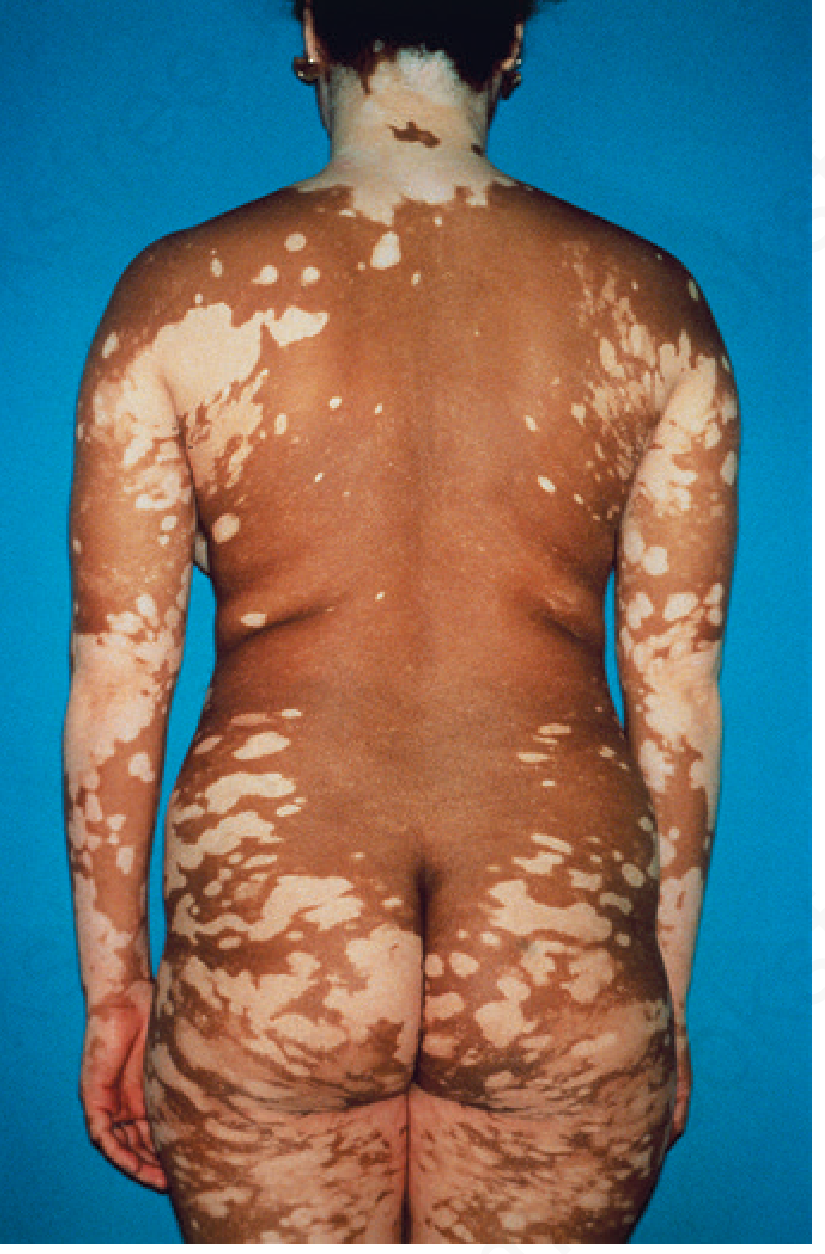
| Generalized (most common) | Symmetric involvement; face, chest, hands, axillae, groin |
| Acrofacial | Distal fingers and facial orifices (lips, tips) |
| Segmental | Unilateral, Blaschkoid pattern; spreads for 1-2 years then stabilizes |
| Focal | Single or few macules in one area, often trigeminal (especially in children) |
| Mucosal | Oral/genital mucosa only |
| Universal | Nearly entire body surface depigmented |
Predilection Sites
Face (especially around orifices - eyes, nose, mouth, ears), dorsal hands, upper chest, axillae, groin, elbows, knees, nipples, umbilicus, genitals, anus. Koebner phenomenon is common - lesions appear at sites of trauma.
Fig. - Segmental vitiligo (face/neck):
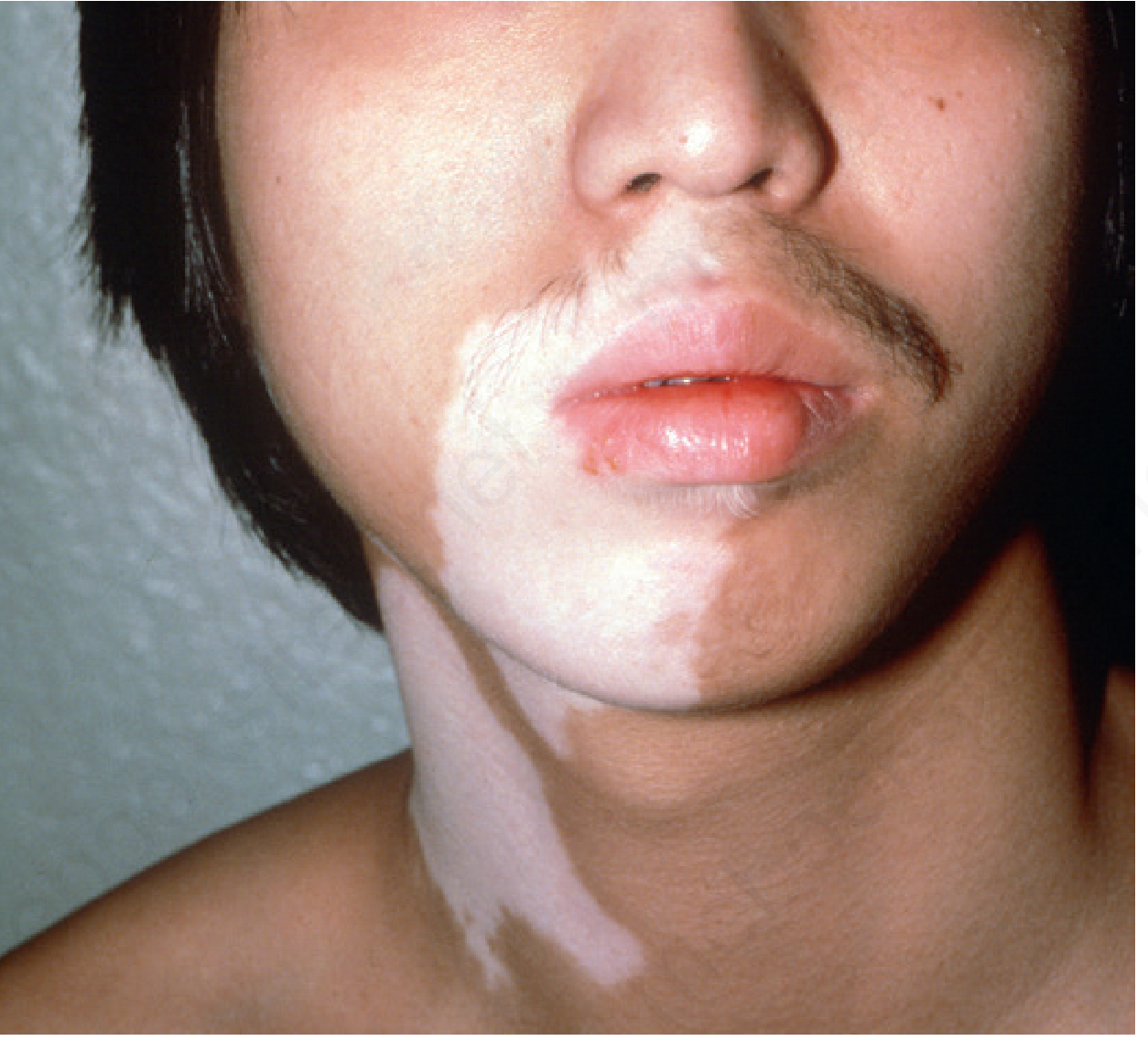
Fig. - Generalized vitiligo (back):
Signs of Active Disease
- Confetti-like lesions
- Hypomelanotic lesions with poorly defined borders
- Trichrome pattern
- Inflammatory (erythematous) border
- Koebnerization
Associated Conditions
Vitiligo correlates with increased risk of other autoimmune diseases, especially:
- Autoimmune thyroid disease (~15% of adults, ~5-15% of children with vitiligo)
- Alopecia areata
- Pernicious anemia
- Type 1 diabetes mellitus
- Addison's disease
- Rheumatoid arthritis, lupus
- Up to 20% of patients have at least one comorbid autoimmune disorder
Notable associated syndromes:
- Vogt-Koyanagi-Harada (VKH) syndrome: uveitis + aseptic meningitis + otic involvement + vitiligo/poliosis
- Alezzandrini syndrome: unilateral facial depigmentation + ipsilateral ocular changes
- Halo nevi: depigmented halo around melanocytic nevi - associated with vitiligo
Paradoxically, vitiligo is associated with a decreased risk of melanoma and other skin cancers.
Diagnosis
Diagnosis is primarily clinical. Key tools:
- Wood's lamp (UV-A light): Enhances contrast of depigmented lesions; particularly useful in fair-skinned patients - lesions fluoresce bright white
- Skin biopsy: Absence of melanocytes on DOPA stain; sparse lymphocytic infiltrate at active edges
- Lab workup for associated autoimmune diseases: TSH, anti-TPO antibodies, FBS, CBC, ANA
Disease Assessment Tools
- Vitiligo Area Scoring Index (VASI)
- Vitiligo European Task Force (VETF) score
- Vitiligo Extent Score (VES)
Treatment
Repigmentation is possible only in areas with pigmented hair follicles (reservoir of melanocyte precursors). Lesions with leukotrichia respond poorly.
1. Topical Therapies
| Agent | Notes |
|---|---|
| Topical corticosteroids | First-line for localized disease; moderate-to-potent class; risk of atrophy with prolonged use |
| Topical calcineurin inhibitors (tacrolimus 0.1%, pimecrolimus 1%) | Preferred for face and flexures; avoids atrophy; also used as maintenance (twice-weekly application) |
| Topical JAK inhibitors (ruxolitinib 1.5%) | Newer; FDA-approved for non-segmental vitiligo; targets JAK1/JAK2-IFN-γ pathway |
2. Phototherapy
- Narrowband UVB (NB-UVB): Most widely used phototherapy; 311-313 nm; effective for generalized disease; can combine with topical agents
- PUVA (psoralen + UVA): Oral or topical psoralen + UVA exposure; effective but more side effects (nausea, phototoxicity, cataract risk with oral PUVA); used less now with NB-UVB available
- Excimer laser (308 nm): Targeted NB-UVB; best for localized, resistant lesions
3. Systemic Therapies
- Oral corticosteroids (mini-pulse): Weekly low-dose dexamethasone or betamethasone; used to halt rapid progression
- Oral JAK inhibitors (ruxolitinib, baricitinib): Emerging; target CXCL9/10-CXCR3 and IFN-γ signaling; promising results in trials
- Oral PUVA (less commonly used now)
4. Surgical Options (for stable, localized vitiligo)
- Suction blister epidermal grafting - most widely used
- Split-thickness skin grafting
- Melanocyte-keratinocyte transplant procedure (MKTP)
- Punch grafting
Surgical options require disease stability (no new lesions, no Koebner phenomenon) for at least 1-2 years.
5. Depigmentation
For extensive treatment-resistant vitiligo with minimal residual normal skin:
- Monobenzyl ether of hydroquinone (MBEH) 20% applied 1-2x/day for 9-12 months
- Requires lifelong strict photoprotection afterward
- Can cause contact dermatitis; may depigment distant sites
6. Cosmetic
- Camouflage cosmetics (cover-up makeup, self-tanning products)
- Micropigmentation (tattooing): Especially useful for lips, nipples, distal fingers - areas with poor repigmentation response
Prognosis & Course
- Course is unpredictable - may spread slowly, stabilize, or rarely progress rapidly
- Segmental vitiligo: reaches full extent within 1-2 years then usually stabilizes
- Generalized vitiligo: typically slow, chronic progression
- Spontaneous partial repigmentation can occur (especially with sun exposure); complete spontaneous repigmentation is rare
- After successful treatment, relapse rate ~40%
Mental Health Impact
Vitiligo carries significant psychosocial burden - social stigma, reduced self-esteem, anxiety, and depression are well-documented, particularly in darker-skinned individuals where contrast is more pronounced and in cultures with historical associations between depigmentation and leprosy. Psychological support is an integral part of management.
Sources: Fitzpatrick's Dermatology (9780071837781), Dermatology 2-Volume Set 5e (9780702082252), Andrews' Diseases of the Skin (9780323547536)
Recent evidence note (PMID 40192197): A 2025 systematic review on off-label topical ruxolitinib in dermatology confirms its growing use in vitiligo, supporting the JAK inhibitor class as an important emerging treatment option.
Auscultation in front and back amd which condn also the sounds
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive, well-structured content from Murray & Nadel and Textbook of Family Medicine. Let me compile the full answer now.
Lung Auscultation: Front, Back & Clinical Correlations
Technique Basics
- Use the diaphragm of the stethoscope for higher-pitched sounds (breath sounds, wheezes, crackles)
- Use the bell for lower-pitched sounds (low-pitched rhonchi, cardiac sounds)
- Apply directly to skin, not through clothing - full skin contact is required
- Patient breathes through an open mouth with slow, deep breaths
- Room must be quiet
Auscultation Areas: Anterior (Front)
Auscultate over the upper and mid-lung fields anteriorly:
| Area | Lung Region Heard | Notes |
|---|---|---|
| Supraclavicular fossa (above clavicle) | Lung apex | Both sides |
| Infraclavicular area (below clavicle, 1st-2nd ICS) | Upper lobe | Both sides |
| 2nd-4th ICS, mid-clavicular line | Upper + mid lobe (R), Upper lobe (L) | |
| 4th-5th ICS, anterior axillary line | Right middle lobe (R) / Lingula (L) | ONLY heard anteriorly |
Key point: The right middle lobe and the lingula of the left lung can ONLY be auscultated anteriorly - they cannot be heard from the back.
Auscultation Areas: Posterior (Back)
The back provides access to the largest surface area of lung tissue (mostly lower lobes):
| Area | Lung Region Heard | Notes |
|---|---|---|
| Suprascapular area (above spine of scapula) | Upper lobe apex | |
| Interscapular area (T3-T7, between scapulae) | Upper and middle lobes | Best heard with arms crossed to move scapulae apart |
| Infrascapular area (below T7) | Lower lobes | Bilateral - most important zone posteriorly |
| Costovertebral angle / lung bases | Lower lobe bases | Often the earliest site for basal crackles (e.g., heart failure) |
Compare left vs right at each level before moving down. Listen to at least 3 levels posteriorly (upper, mid, lower).
Systematic Sequence (Standard Approach)
Posterior (patient sitting or leaning forward):
- Upper zones (between neck and spine of scapula)
- Mid zones (interscapular)
- Lower zones (below scapulae, down to bases)
Anterior (patient supine or sitting facing you):
- Apices (supraclavicular)
- Upper zones (infraclavicular)
- Mid zones (right middle lobe / lingula)
Lateral (axillary lines - often forgotten):
- Mid-axillary line at 4th-6th ICS
- Important for detecting early pleural effusion and lower lobe pathology
Types of Breath Sounds
Normal Sounds
| Sound | Characteristics | Normal Location |
|---|---|---|
| Vesicular (normal breath sounds) | Soft, low-pitched; inspiration louder and longer than expiration (3:1 ratio); no gap between I and E | Peripheral lung fields (all zones except trachea) |
| Bronchial (tracheal) | Loud, high-pitched, hollow; expiration = inspiration or louder; gap between I and E | Over trachea/manubrium only (normal there) |
| Bronchovesicular | Intermediate intensity and pitch; I:E roughly equal | 1st and 2nd ICS anteriorly; between scapulae posteriorly |
Adventitious (Abnormal) Sounds - ATS Classification
| Sound | Characteristics | Mechanism | Clinical Condition |
|---|---|---|---|
| Fine crackles | Soft, high-pitched, short, discontinuous; mid-to-late inspiratory; like rubbing hair near the ear | Sudden opening of collapsed distal airways | Pulmonary fibrosis, early pulmonary edema, early pneumonia |
| Coarse crackles | Loud, low-pitched, longer, early inspiratory or expiratory; may clear with cough | Opening of secretion-laden distal airways | Bronchiectasis, COPD, pneumonia with secretions |
| Wheezes | Continuous (>250 ms), high-pitched (≥400 Hz), musical/hissing | Airway narrowing - oscillation of airway walls | Asthma, COPD (diffuse); endobronchial lesion (focal) |
| Rhonchi | Continuous (>250 ms), low-pitched (<200 Hz), snoring quality; may clear with cough | Secretions in large airways | COPD with secretions, chronic bronchitis |
| Stridor | Loud, high-pitched, mainly inspiratory; heard best over neck | Extrathoracic/upper airway obstruction | Croup, epiglottitis, anaphylaxis, foreign body - URGENT |
| Bronchial sounds in periphery | Abnormal when heard outside trachea/manubrium | Airless air spaces around a patent airway | Consolidation (pneumonia), atelectasis |
| Pleural friction rub | Creaking/grating, like leather rubbing; both inspiratory and expiratory; disappears when breath held | Inflamed pleural surfaces rubbing | Pleuritis, pulmonary infarction (PE), pleuropneumonia |
Vocal Resonance Tests
Done during auscultation to differentiate consolidation vs. effusion:
| Test | Method | Normal | Consolidation | Pleural Effusion |
|---|---|---|---|---|
| Bronchophony | Patient says "99" | Muffled | Loud and clear | Absent/muffled |
| Egophony | Patient says "E" | Sounds like "E" | Sounds like "A" (E-to-A change) | Absent (except at effusion upper border) |
| Whispered pectoriloquy | Patient whispers "1-2-3" | Faint/inaudible | Clearly heard | Absent |
Clinical Correlations: Auscultation Findings by Disease
| Disorder | Breath Sounds | Added Sounds | Other |
|---|---|---|---|
| Pneumonia (consolidation) | Bronchial breath sounds (periphery) | Crackles (fine/coarse) | Bronchophony, egophony, whispered pectoriloquy all increased; dullness on percussion |
| Pleural effusion (large) | Absent/decreased | None (or rub above effusion line) | Dullness; stony dullness; trachea shifted AWAY; decreased fremitus; egophony at upper border only |
| Pneumothorax | Absent on affected side | None | Hyperresonance; trachea shifted AWAY (tension PTX); absent fremitus |
| Bronchial asthma (acute) | Vesicular with prolonged expiration | Expiratory wheezes (may be pan-inspiratory/expiratory) | Hyperresonant; decreased expansion; decreased fremitus |
| COPD | Decreased/quiet breath sounds | Wheezes, rhonchi | Hyperinflation; pursed-lip breathing; barrel chest |
| Atelectasis | Absent/decreased | None | Dullness; trachea shifted TOWARD affected side; decreased fremitus |
| Pulmonary fibrosis (ILD) | Normal or reduced | Fine "Velcro" crackles (bilateral, basal, end-inspiratory) | Clubbing; restrictive spirometry |
| Pulmonary edema (CHF) | Decreased at bases | Bilateral basal fine crackles (initially), progressing upward | S3 gallop; JVD; orthopnea |
| Bronchiectasis | Coarse or bronchial | Coarse crackles, wheezes | Persistent; sputum production |
| Pulmonary embolism | Usually normal | Pleural rub (if infarction) | Tachycardia; may have minimal auscultatory findings |
| Foreign body (large airway) | Decreased unilaterally | Focal wheeze (unilateral, monophonic) | Stridor if upper airway |
| Lung collapse (lobar) | Absent over that lobe | None | Trachea shifted toward collapse |
Quick Memory Summary
- Bronchial sounds in periphery = consolidation or atelectasis (airless lung around open bronchus)
- Fine crackles at bases = pulmonary edema or fibrosis
- Coarse crackles clearing with cough = secretions (bronchiectasis, COPD)
- Diffuse expiratory wheeze = asthma or COPD
- Monophonic/unilateral wheeze = endobronchial obstruction
- Absent breath sounds + hyperresonance = pneumothorax
- Absent breath sounds + dull percussion = effusion or total atelectasis
- Pleural rub = pleuritis/infarct
- Stridor = upper airway emergency
Sources: Murray & Nadel's Textbook of Respiratory Medicine (9780323655873); Textbook of Family Medicine 9e (9780323239905); Goldman-Cecil Medicine (9780323930345)
This is a shared conversation. Sign in to Orris to start your own chat.