Make the detailed research on the topic of Post menopausal syndrome
Reading File
Finding Sources
Searching PubMed
"postmenopausal syndrome" OR "menopause" AND "management"
Searching the Web
postmenopausal syndrome symptoms pathophysiology management 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
fezolinetant elinzanetant vasomotor symptoms menopause
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full detailed research report:
Post-Menopausal Syndrome: Detailed Research Overview
1. Definition and Classification
Menopause is defined as the permanent cessation of menses, representing the culmination of reproductive aging. It is confirmed retrospectively after 12 consecutive months of amenorrhea in the absence of other pathologic causes. The median age at natural menopause is 51-52.5 years.
Post-menopausal syndrome refers to the constellation of four core symptom clusters that arise from the loss of ovarian estrogen and progesterone:
- Vasomotor symptoms (hot flashes/flushes)
- Genitourinary syndrome of menopause (GSM)
- Sleep disturbances
- Mood changes
Health risks that accumulate over time include osteoporosis, cardiovascular disease, cognitive decline, and increased cancer risk.
- Goldman-Cecil Medicine, p. 2597
- Guyton & Hall Medical Physiology, p. 1028
2. Staging of Reproductive Aging (STRAW Paradigm)
| Stage | Reproductive (-5 to -3) | Menopausal Transition (-2 to -1) | Postmenopause (+1 to +2) |
|---|---|---|---|
| Age (approx.) | 13-47 | 47-52 | 50+ |
| Menses | Mostly regular | Minor irregularity → ≥60-364 days amenorrhea | Permanent amenorrhea |
| FSH | Low | Sporadically elevated | Consistently elevated (≥25 IU/L) |
| AMH | High | Normal to low | Undetectable |
- Stage 0 = Final Menstrual Period (FMP)
- Goldman-Cecil Medicine, p. 2598
3. Epidemiology
Menopause is a universal biological event in women. Approximately 1.3 million women enter menopause each year in the United States. The lived experience varies markedly among individuals and across racial/ethnic groups. African American and Hispanic women tend to enter menopause ~2 years earlier than Caucasian women; Asian women tend to enter ~1-2 years later.
Factors influencing age at menopause:
| Factor | Direction | Degree |
|---|---|---|
| Smoking | Earlier | 1-2 years |
| Low socioeconomic status | Earlier | 1-2 years |
| Endocrine-disrupting chemicals | Earlier | 1.8-3.8 years |
| High altitude | Earlier | 1-1.5 years |
| Oral contraceptive use | Later | ~6 months |
| Higher parity | Later | Variable |
| Fragile X premutation | Earlier | Variable |
| Mosaic Turner syndrome | Earlier | Variable |
- Goldman-Cecil Medicine, p. 2595
4. Pathophysiology
4a. Ovarian Follicular Depletion
The primary driver is progressive depletion of primordial follicles. A woman is born with ~1-2 million oocytes; by menarche ~400,000 remain; only ~400 ovulate over the reproductive lifespan. By age ~45, the number of primordial follicles approaches zero. This decline is accelerated during the perimenopause.
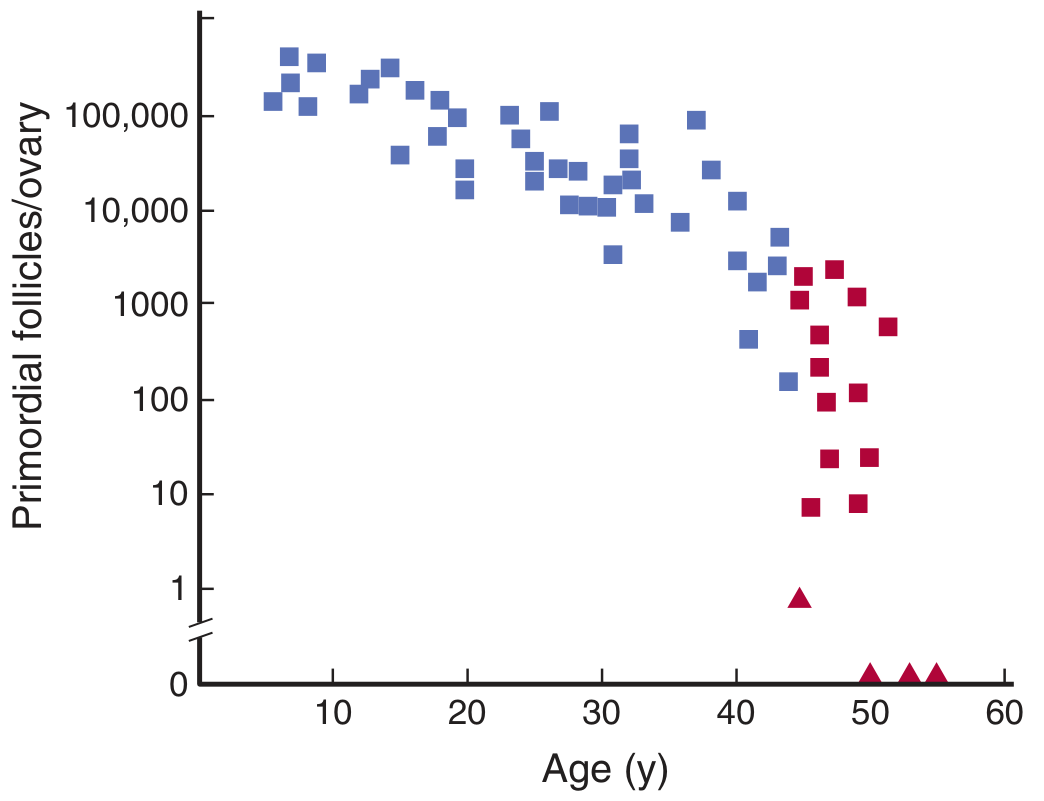
Figure: Number of primordial follicles per ovary at various ages (Ganong's Review of Medical Physiology, 26th ed., p. 686)
4b. Hormonal Changes
As follicles are depleted:
-
Estradiol (E2) falls markedly - from ~100-400 pg/mL in reproductive years to <20 pg/mL postmenopausally
-
Progesterone falls to near zero (anovulatory cycles → no corpus luteum)
-
Inhibin A and B decrease - releasing negative feedback on the pituitary
-
FSH rises markedly (often >25-40 IU/L) - the most reliable hormonal marker
-
LH rises moderately
-
Peripheral aromatization of androstenedione (from adrenals) to estrone becomes the primary estrogen source in postmenopause - explains why obese women have milder symptoms (more adipose aromatase activity)
-
Ganong's Review, p. 686-690
-
Guyton & Hall, p. 1028
4c. Mechanism of Hot Flashes
Hot flashes coincide with episodic LH surges but LH itself is not causal (symptoms continue after hypophysectomy). The current hypothesis centers on estrogen-sensitive hypothalamic neurons:
- Estrogen normally modulates the thermoregulatory "set point" in the preoptic/anterior hypothalamus
- Estrogen withdrawal narrows the thermoneutral zone - small temperature rises trigger heat-dissipation responses (peripheral vasodilation, sweating)
- KNDy neurons (kisspeptin/neurokinin B/dynorphin) in the arcuate nucleus are estrogen-sensitive and drive episodic GnRH/LH secretion - neurokinin B (acting on NK3 receptors) is now understood to be a key trigger of hot flashes
This explains why NK3 receptor antagonists (fezolinetant, elinzanetant) effectively suppress hot flashes without estrogen.
- Ganong's Review, p. 699
- Goldman-Cecil Medicine, p. 4228
5. Clinical Features
5a. Vasomotor Symptoms
- Hot flashes (flushes): Sudden sensation of intense warmth, typically starting in the chest/face and spreading; lasting 2-4 minutes, often with sweating, palpitations, chills, and anxiety
- Frequency: 1 to many times/day; often worse at night ("night sweats")
- Prevalence: ~75% of menopausal women
- Average duration: 5.2 years (range up to 20+ years)
- Night sweats disrupt sleep, contributing to secondary insomnia, fatigue, and cognitive complaints
5b. Genitourinary Syndrome of Menopause (GSM)
Formerly called "atrophic vaginitis" - now recognized as a broader entity affecting the genital, urinary, and sexual systems. GSM worsens over time and does not resolve spontaneously.
Genital symptoms:
- Vaginal dryness, itching, burning, irritation
- Reduced vaginal secretions and lubrication
- Vaginal wall thinning, pallor, loss of rugae
Urinary symptoms:
- Dysuria, urinary urgency/frequency, nocturia
- Recurrent urinary tract infections (UTIs)
- Stress and/or urge incontinence (urethral epithelial thinning + weakened pelvic floor)
Sexual symptoms:
- Dyspareunia (painful intercourse)
- Reduced arousal and delayed/absent orgasm
- Postcoital bleeding
- Decreased libido (hypoactive sexual desire disorder - HSDD)
5c. Sleep Disturbances
- Difficulty falling/staying asleep
- Increased sleep apnea (rate rises from 6.5% at 30-39 years to ~16% at 50-60 years; possibly related to progesterone loss - progesterone is a respiratory stimulant)
- Decline in melatonin and growth hormone further disrupts sleep architecture
5d. Mood and Psychological Symptoms
- Irritability, anxiety, mood swings, depression
- Women with prior PMS or postpartum depression are particularly vulnerable
- Notably, mood effects can be independent of sleep disruption from hot flashes
- Cognitive behavioral therapy (CBT) has evidence for both mood and vasomotor symptoms
5e. Metabolic and Body Composition Changes
- Redistribution of fat from gynoid (hips/thighs) to android (abdominal/visceral) pattern
- Increased insulin resistance
- Adverse changes in lipid profile: LDL increases, HDL decreases
- Accelerated rate of weight gain
5f. Skeletal Effects
- Estrogen normally suppresses osteoclast activity (RANK-L pathway) - its loss accelerates bone resorption
- Bone mineral density (BMD) decreases at 2-3% per year in the first 5-10 years postmenopausally
- Risk of osteoporosis and fragility fractures (hip, vertebral, distal radius)
- Risk highest in thin, smoking, Caucasian/Asian, physically inactive women with low calcium intake
5g. Cardiovascular Risk
- Estrogen normally promotes HDL, reduces LDL, maintains endothelial function and vasodilation, reduces platelet aggregation
- Postmenopausally: risk of coronary artery disease, hypertension, and stroke rises sharply
- After age 55, CVD risk in women approaches that of men
6. Diagnosis
Clinical diagnosis:
- Amenorrhea for ≥12 months in a woman ≥45 years old - diagnosis is retrospective
- History of typical symptoms (hot flashes, night sweats, vaginal dryness)
Laboratory confirmation (when clinically uncertain):
- FSH ≥25 IU/L - most useful single test; consistently elevated in postmenopause
- Estradiol <20 pg/mL
- AMH (Anti-Müllerian Hormone): most reliable marker of ovarian reserve; undetectable in postmenopause; does not fluctuate with the menstrual cycle
- Inhibin B: low/undetectable
- LH: elevated (moderate)
Note: FSH and inhibin B fluctuate in perimenopause and are less reliable at that stage; AMH is preferred for estimating proximity to FMP.
- Goldman-Cecil Medicine, p. 4199-4201
- Tietz Textbook of Laboratory Medicine
7. Long-term Consequences
| System | Consequence |
|---|---|
| Skeletal | Osteoporosis, fragility fractures |
| Cardiovascular | CAD, hypertension, dyslipidemia |
| Neurological | Increased risk of Alzheimer's dementia (estrogen has neuroprotective effects) |
| Urogenital | Persistent GSM, recurrent UTIs, pelvic organ prolapse |
| Metabolic | Type 2 diabetes risk, metabolic syndrome |
| Psychological | Depression, anxiety, cognitive decline |
8. Management
8a. General Principles
Current guidelines (ACOG, NAMS, NICE 2024) state that symptomatic treatment as needed is appropriate for this normal life transition. Shared decision-making is emphasized - risks and benefits must be individualized.
8b. Hormone Therapy (HT) - the Most Effective Treatment
Indications: Moderate-to-severe vasomotor symptoms, GSM, prevention of bone loss in women with symptoms. HT also improves mood, sleep, and sexual function.
Types:
- Estrogen alone - for women post-hysterectomy
- Estrogen + progestogen - for women with an intact uterus (progestogen protects the endometrium from estrogen-induced hyperplasia/cancer)
- Routes: Oral, transdermal (patch, gel), vaginal (cream, ring, tablet/suppository)
- Transdermal/vaginal estrogen avoids first-pass hepatic metabolism - lower VTE and triglyceride risk vs. oral
Dosages (Katzung):
- Conjugated estrogen: 0.3-1.25 mg/day orally
- Ethinyl estradiol: 0.01-0.02 mg/day
- Start at the lowest effective dose
Benefits (from WHI data):
- 50-90% reduction in vasomotor symptoms
- Significant improvement in GSM (virtually all cases)
- 33% reduction in hip fracture risk (both E alone and E+P)
- Improvement in sleep quality, mood, and quality of life
Risks (from WHI - women 50-79 years):
| Outcome | Estrogen + Progestin | Estrogen Alone |
|---|---|---|
| Breast cancer | +24% increased risk (after ≥5 years) | No increased risk (possibly reduced) |
| VTE / PE | +78-87% increased risk | +73-76% increased risk |
| DVT | +87% increased risk | +76% increased risk |
| Endometrial cancer | Neutral (progestin protective) | +4.6 excess cases/10,000/year |
| Colorectal cancer | Small protective effect | Small protective effect |
| Hip fracture | 33% decreased risk | 33% decreased risk |
| Coronary heart disease | Neutral/slightly increased | Neutral |
The "Timing Hypothesis" (most important current concept):
- Risk-benefit balance is more favorable when HT is started within 10 years of menopause or before age 60 ("window of opportunity")
- When started later (>10 years post-FMP), cardiovascular and neurological risks increase
- Goldman-Cecil Medicine, p. 4244-4251
- Harrison's Principles, p. 3187
- Guyton & Hall, p. 1028
Contraindications to systemic HT:
- Personal history of breast cancer, endometrial cancer
- Active or recent VTE, PE
- Active CVD or recent MI/stroke
- Liver disease
- Unexplained vaginal bleeding
Local/vaginal estrogen: Very low systemic absorption; safe even in women who cannot use systemic HT; effective for GSM. (2024 systematic review, PMID 39250810 confirmed efficacy.)
8c. Non-Hormonal Pharmacological Treatments
| Drug | Dose | Efficacy for Hot Flashes | Notes |
|---|---|---|---|
| Fezolinetant (NK3 antagonist) | 45 mg/day | ~50-60% reduction | FDA-approved 2023; risk: hepatotoxicity; first-in-class non-hormonal |
| Elinzanetant (NK3 antagonist) | Investigational | Similar to fezolinetant | Phase 3 trials 2024; also improves sleep |
| Paroxetine mesylate | 7.5 mg/day | ~50% reduction | Only FDA-approved SSRI for hot flashes |
| Venlafaxine (SNRI) | 37.5-75 mg/day | ~50% reduction | Good evidence |
| Desvenlafaxine | 100 mg/day | Moderate | - |
| Fluoxetine | 10-30 mg/day | Modest | Lower efficacy |
| Citalopram/Escitalopram | 10-30 mg/day | Moderate | - |
| Gabapentin | 300 mg nightly (up to 900 mg/day) | Moderate | Also helps sleep |
| Oxybutynin | 2.5-5 mg twice daily | Moderate | Anticholinergic |
| Clonidine | 0.1-1 mg/day oral | Modest | Inconsistent evidence |
Fezolinetant and elinzanetant (NK3/NK1 receptor antagonists) represent the most significant recent pharmacological advance - acting on the KNDy neuronal pathway. Multiple 2025 systematic reviews confirm their efficacy (PMIDs: 39987726, 39746208, 40592206).
- Harrison's Principles, p. 3187
- Goldman-Cecil Medicine, p. 4228
8d. Treatment of Osteoporosis
- Calcium supplementation to total 1500 mg/day + Vitamin D (600-2000 IU/day)
- Bisphosphonates (alendronate, risedronate, zoledronate): first-line for osteoporosis
- HT if also symptomatic
- Raloxifene (SERM): bone-protective + reduces breast cancer risk; can worsen vasomotor symptoms; increases VTE risk
- Denosumab: RANK-L inhibitor for severe osteoporosis
- Teriparatide / Abaloparatide: anabolic agents for severe cases
8e. Complementary and Integrative Health (CIH)
- Black cohosh (Cimicifuga racemosa): SERM-like + serotonin receptor modulation; does not contain phytoestrogens; dose 40 mg twice daily (Remifemin); evidence inconsistent (Cochrane 2012); possible rare hepatotoxicity; may help depression/anxiety
- Soy isoflavones / phytoestrogens: mild benefit for vasomotor symptoms; similar to placebo in some trials
- Vitamin E: no significant benefit over placebo
- Omega-3 fatty acids: inconsistent evidence
- Cognitive behavioral therapy (CBT): ~50% efficacy for hot flashes, endorsed in guidelines
- Acupuncture: some evidence, not consistent
- Exercise, yoga: not proven effective for vasomotor symptoms; beneficial for general well-being, bone density, cardiovascular health
- Berek & Novak's Gynecology, p. 1165-1166
8f. Lifestyle Interventions
- Hot flash triggers to avoid: caffeine, alcohol, spicy foods, warm environments
- Layering clothing, cool room temperature
- Weight loss: observational evidence for benefit (adipose tissue as estrogen source)
- Regular weight-bearing exercise: slows bone loss, reduces cardiovascular risk
- Mediterranean diet: associated with favorable reproductive aging outcomes (PMID 37506751)
- Smoking cessation: slows post-menopausal bone loss
8g. Management of GSM Specifically
- Local vaginal estrogen (cream, ring, tablet): most effective; minimal systemic absorption; safe long-term
- Vaginal moisturizers (non-hormonal): for daily maintenance; shown effective in 2024 systematic review (PMID 39250810)
- Lubricants: for intercourse
- Ospemifene (oral SERM): for dyspareunia in women who cannot use vaginal estrogen
- Prasterone (intravaginal DHEA): FDA-approved; converted locally to estrogen and testosterone
8h. Sexual Dysfunction / HSDD
- Testosterone therapy: small but significant improvement in sexual desire; off-label use in postmenopausal women; 2023 meta-analysis supports short-term use (PMID 37314872)
- Flibanserin: approved for premenopausal HSDD only
- Psychosexual counseling and couples therapy
9. Special Situations
Premature Ovarian Insufficiency (POI)
- Menopause before age 40 (affects ~1% of women)
- Higher cardiovascular, cognitive, and skeletal risk than natural menopause
- HT is strongly recommended until the natural age of menopause (~51 years) regardless of contraindications that apply to older women
Surgical Menopause
- Bilateral oophorectomy causes sudden, severe postmenopausal symptoms (more abrupt than natural)
- Often more severe vasomotor symptoms
- HT strongly recommended if no contraindication
Menopause and Psychiatric Medications
- SSRIs used for hot flashes may interact with tamoxifen (paroxetine/fluoxetine inhibit CYP2D6 → reduce tamoxifen efficacy)
- Venlafaxine preferred in breast cancer survivors
- Maudsley Prescribing Guidelines, 15th ed.
10. Recent Evidence Updates (2023-2025)
| Study / Source | Finding |
|---|---|
| PMID 38016166 (Network meta-analysis, 2024) | Fezolinetant comparable to low-dose HT for vasomotor symptom frequency reduction |
| PMID 39987726 (Meta-analysis, 2025) | Both fezolinetant and elinzanetant significantly reduce hot flash frequency/severity vs. placebo |
| PMID 39250810 (Systematic review, Ann Intern Med, 2024) | Local hormonal treatments and vaginal moisturizers both effective for GSM; local estrogen superior |
| PMID 37314872 (Meta-analysis, Menopause, 2023) | Testosterone improves sexual function/desire in postmenopausal women |
| PMID 38669625 (Meta-analysis, 2024) | Mind-body exercise (yoga, Tai chi, qigong) improves physical and psychological menopausal symptoms |
| Korean Society of Menopause Guidelines 2025 | Lifestyle + CBT first-line; HT timing window concept reinforced; proactive GSM screening recommended |
| NICE Guidelines Nov 2024 | Updated to recommend HT as first-line for symptomatic women without contraindications, with individualized risk assessment |
11. Summary Algorithm for Clinical Management
Postmenopausal woman with symptoms
|
Symptom assessment
/ | \
Mild Moderate Severe
| | |
Lifestyle + Nonhormonal + Consider HT
Changes (CBT, SNRIs, (if no contraindications)
fezolinetant) Transdermal preferred
GSM present? → Local vaginal estrogen / moisturizers (all severity levels)
Osteoporosis risk? → BMD (DEXA), calcium/Vit D, bisphosphonates if indicated
Sources
- Goldman-Cecil Medicine International Edition (2024), Chapter 222 - Nanette Santoro & Genevieve Neal-Perry
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 107
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter: Postmenopausal Hormonal Therapy
- Guyton & Hall Textbook of Medical Physiology, Chapter 82
- Ganong's Review of Medical Physiology, 26th Edition, Chapter 22
- Berek & Novak's Gynecology - Chapter: Menopause
- Textbook of Family Medicine, 9th Edition
- Recent PubMed Systematic Reviews (2023-2025): PMIDs 37506751, 38016166, 38669625, 39250810, 37314872, 39987726, 40592206
This is a shared conversation. Sign in to Orris to start your own chat.