Write down the diagnostic plan for a patient with history of gastric,h pylori negative, reflux taking voraprazan but still symptomatic and Les pressure low, no dental caries, halitosis, weight normal BMI,no respiratory symptoms and no pain in chest,no HTN and diabetes, mother has diabetes and HTN...no tb or other conditions
Reading File
Finding Sources
Finding Sources
Searching PubMed
vonoprazan refractory GERD diagnosis
Searching the Web
refractory GERD low LES pressure vonoprazan still symptomatic diagnostic workup 2024 2025
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
refractory GERD diagnostic workup esophageal impedance pH manometry
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I now have sufficient information from the library and current literature to write the full diagnostic plan. Let me compile the comprehensive answer.
Diagnostic Plan: Refractory GERD on Vonoprazan with Low LES Pressure
Clinical Summary
Patient profile: Known gastric/esophageal reflux disease, H. pylori negative, on vonoprazan (potassium-competitive acid blocker / P-CAB), still symptomatic. Low LES (lower esophageal sphincter) pressure confirmed. Normal BMI, no dental caries, halitosis present, no chest pain, no respiratory symptoms, no HTN or diabetes. Family history: mother with diabetes and HTN.
This is a case of refractory GERD on optimized acid suppression - the most important diagnostic challenge is distinguishing between:
- True acid breakthrough / persistent pathological reflux despite vonoprazan
- Weakly acidic or non-acid (alkaline/bile) reflux
- Esophageal hypersensitivity
- Functional heartburn (no true reflux)
- A structural/motility problem driving the low LES pressure
- An alternate or co-existing diagnosis
Step 1 - Confirm Compliance and Optimise Before Further Testing
- Verify vonoprazan dose: 20 mg once daily for active symptoms (healing dose), taken correctly
- Rule out medications that further reduce LES pressure: calcium channel blockers, nitrates, theophylline, benzodiazepines, NSAIDs, anticholinergics - ask explicitly
- Review dietary triggers: fatty foods, chocolate, citrus, carbonated drinks, coffee, alcohol, late meals, lying down after eating
- Review lifestyle: smoking (nicotine lowers LES pressure), body position in bed (head of bed elevation?)
- Rule out recent weight gain even within normal BMI range (abdominal adiposity can occur at normal BMI)
Step 2 - Upper Endoscopy (EGD) with Biopsies (First Priority if Not Recently Done)
Indications in this patient:
- Persistent symptoms despite potent acid suppression
- Halitosis (raises concern for mucosal disease, bile reflux, gastroparesis)
- Evaluate for complications and alternate diagnoses
What to look for and biopsy:
| Finding | Significance |
|---|---|
| Erosive esophagitis (grade A-D, LA classification) | Confirms acid/reflux injury persisting despite P-CAB |
| Barrett's esophagus (salmon-colored mucosa) | Long-term GERD complication; mandates surveillance |
| Hiatal hernia | Low LES pressure + hiatal hernia = mechanical failure; drives regurgitation independent of acid |
| Eosinophilic esophagitis (EoE) | Rings/furrows/exudates; biopsies show >15 eosinophils/HPF; can mimic GERD and is refractory to acid suppression |
| Pill-induced or caustic esophagitis | Discrete ulceration |
| Bile/duodenal reflux | Bile-stained mucosa, greenish fluid in stomach |
| Gastric mucosal abnormality | Rule out residual gastric pathology |
| Peptic stricture | Dysphagia may be subtle |
Reference: Goldman-Cecil Medicine - "endoscopy is indicated for cases with persistent symptoms... to exclude eosinophilic esophagitis, pill-induced esophagitis, stricture, Barrett esophagus, and malignancy."
Step 3 - Ambulatory 24-hour pH-Impedance Monitoring (Most Important Functional Test)
This is the gold standard for evaluating refractory symptoms on therapy.
Two scenarios:
A. Off vonoprazan (after 7-14 day washout) - "off therapy" pH study:
- Use wireless Bravo capsule (48-96 hours) or nasal catheter
- Determines if there is true pathological acid exposure (DeMeester score, % time pH <4)
- If normal: favors functional heartburn or hypersensitivity, not true GERD
B. On vonoprazan - "on therapy" pH-impedance study:
- Combined multichannel intraluminal impedance (MII) + pH catheter
- Detects both acid and non-acid reflux events
- Evaluates symptom-reflux association (Symptom Index, Symptom Association Probability)
- If non-acid reflux episodes are temporally linked to symptoms: weakly acidic or alkaline reflux is driving symptoms - acid suppression alone will not help
Reference: Harrison's 22nd Edition - "Combined esophageal pH and impedance testing using a transnasal catheter while on PPI therapy can define if a patient with persistent or atypical symptoms has esophageal hypersensitivity or regurgitation of nonacidic or weakly acidic fluid."
Step 4 - High-Resolution Esophageal Manometry (HRM)
Directly relevant given the known low LES pressure.
What it evaluates:
- LES resting pressure (confirm degree and type of hypotension)
- Transient LES relaxations (TLESRs) - the most common mechanism of reflux even in low LES pressure states
- Esophageal body motility - ineffective esophageal motility (IEM) is common in GERD and impairs acid clearance
- Hiatal hernia - manometric identification and sizing
- Rule out major motor disorders that mimic GERD:
- Achalasia - can present with regurgitation and be misdiagnosed as GERD (very important to exclude)
- Hypercontractile esophagus (Jackhammer)
- Distal esophageal spasm
Reference: Washington Manual - "Esophageal manometry, particularly HRM, may identify motor processes contributing to refractory symptoms." Yamada's Gastroenterology - "Esophageal manometry is useful for detecting major motor disorders or evaluating peristalsis before antireflux surgery."
Step 5 - Gastric Emptying Study (Rule out Gastroparesis)
Why relevant in this patient:
- Halitosis + refractory symptoms on acid suppression despite H. pylori negativity raises concern
- Delayed gastric emptying increases gastric distension, raises intragastric pressure, worsens reflux, and can cause regurgitation and halitosis independent of acid
- 20% of gastroparesis patients have pain predominance rather than nausea/vomiting
Test:
- 4-hour solid-meal gastric scintigraphy (radiolabeled technetium-99m egg meal) - gold standard
- Alternative: 13C-octanoate breath test (non-radioactive)
- Alternative: Wireless motility capsule (SmartPill) - also assesses small bowel/colon transit
Step 6 - Laryngoscopy / ENT Evaluation
Why this patient:
- Halitosis is present - while gastroparesis and reflux are common causes, laryngopharyngeal reflux (LPR) should be evaluated
- LPR may persist or worsen even with good esophageal acid control because brief pharyngeal acid exposures are sufficient for laryngeal injury
- ENT exam: posterior laryngeal erythema, cobblestoning, vocal cord edema (Belafsky Reflux Finding Score)
- Consider dedicated hypopharyngeal-esophageal multichannel pH-impedance or pharyngeal pH probe (Restech) if LPR is suspected
Step 7 - Rumination Syndrome Assessment
- Low LES pressure + regurgitation + refractory symptoms on acid suppression are all consistent with rumination syndrome which is commonly misdiagnosed as GERD
- Diagnostic criteria (Rome IV): recurrent regurgitation of recently ingested food, not preceded by retching, cessation when material becomes acidic
- Confirmed on HRM: characteristic pattern of intra-abdominal pressure rises immediately post-prandially preceding regurgitation
- Important because this is behavioural/physiotherapy-managed - not medication-managed
Step 8 - Additional Blood Tests
| Test | Rationale |
|---|---|
| FBC / CBC | Exclude anemia from esophagitis/peptic disease |
| Serum gastrin (fasting) | Vonoprazan can elevate gastrin; rule out Zollinger-Ellison syndrome if markedly elevated |
| Thyroid function (TSH) | Hypothyroidism causes gastroparesis and dysmotility mimicking GERD |
| HbA1c and fasting glucose | Family history of diabetes; insulin resistance/early diabetes can cause gastroparesis |
| Calcium, PTH | Hypercalcemia / hyperparathyroidism causes peptic disease and dysmotility |
| Serum IgA + tissue transglutaminase | Celiac disease mimics upper GI symptoms |
| Esophageal eosinophil biopsy result | From endoscopy (Step 2) |
Diagnostic Algorithm Summary
Refractory symptoms on vonoprazan
↓
Step 1: Compliance check + medication/diet/lifestyle review
↓
Step 2: Upper endoscopy + biopsies
→ Barrett's? EoE? Hiatal hernia? Bile reflux? Stricture?
↓
Step 3: 24h pH-impedance monitoring (on therapy)
→ True acid reflux? Non-acid reflux? Hypersensitivity? Functional heartburn?
↓
Step 4: High-resolution esophageal manometry
→ Low LES confirmed? Achalasia excluded? IEM? Rumination pattern?
↓
Step 5: Gastric emptying scintigraphy
→ Gastroparesis contributing to reflux/halitosis?
↓
Step 6: ENT / laryngoscopy for LPR
↓
Step 7: Blood panel (gastrin, thyroid, HbA1c, celiac screen)
Key Diagnoses to Definitively Exclude in This Patient
| Diagnosis | Why it fits | Key test |
|---|---|---|
| Non-acid / bile reflux | Low LES, refractory to acid suppression | pH-impedance on therapy |
| Esophageal hypersensitivity | Symptoms without pathological reflux | pH-impedance + symptom correlation |
| Functional heartburn | Rome IV criteria; no true reflux | pH-impedance off therapy |
| Hiatal hernia with mechanical reflux | Low LES pressure may be partly from hernia | HRM + endoscopy |
| Achalasia | Regurgitation mimics GERD, refractory to all acid suppressants | HRM |
| Eosinophilic esophagitis | Refractory to acid suppression, normal BMI, young patients | Endoscopy + biopsy |
| Gastroparesis | Halitosis, worsens reflux, H. pylori negative | Gastric emptying scan |
| LPR | Halitosis, throat symptoms | ENT + pharyngeal pH probe |
| Rumination syndrome | Regurgitation, low LES on manometry | HRM + Rome IV criteria |
| Early diabetes-related dysmotility | Strong family history of diabetes | HbA1c, fasting glucose |
Note on Vonoprazan Specifically
Vonoprazan (P-CAB) provides stronger, more consistent acid suppression than PPIs by blocking the H⁺/K⁺-ATPase pump in a potassium-competitive manner, with less CYP2C19 dependence. Persistent symptoms on vonoprazan 20 mg are therefore strong evidence that acid alone is not the problem - the diagnostic workup above is essential to identify the true driver.
Recent evidence (PMID 40450492 - Italian GERD Guidelines 2025; PMID 41616396 - GERD in the 21st century, 2026) reinforces the stepwise approach: endoscopy first, then pH-impedance monitoring to phenotype the refractory patient, followed by manometry.
Sources: Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine, Sleisenger & Fordtran's GI and Liver Disease, Yamada's Textbook of Gastroenterology 7e, Washington Manual of Medical Therapeutics, Current Surgical Therapy 14e; supplemented with Italian GERD Guidelines 2025 (PMID 40450492) and GERD 21st Century Review 2026 (PMID 41616396).
How to examine and tell if a child is in pain and which part medically
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
pediatric pain assessment tools examination techniques localize pain in children clinical 2024
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
How to Examine and Determine if a Child is in Pain - and Where
Assessing pain in children is one of the most important - and most challenging - skills in pediatric clinical practice. The approach depends entirely on the child's age and developmental stage, because young children cannot verbally report pain the way adults do.
Part 1 - General Signs That a Child Is in Pain
Before applying any formal tool, look for these universal indicators across all ages:
Physiologic (Autonomic) Signs
These appear most strongly in acute pain and may fade with chronic or ongoing pain:
| Sign | What to Look For |
|---|---|
| Tachycardia | Heart rate elevated above age-normal |
| Hypertension | BP elevated for age |
| Tachypnea | Rapid breathing, irregular pattern |
| Oxygen desaturation | SpO2 drop in monitored patients |
| Diaphoresis | Sweating unexplained by fever |
| Pallor or flushing | Skin colour change |
| Dilated pupils | Sympathetic activation |
Note: Do NOT use vital signs alone as your only pain measure - they lack specificity and sensitivity for pain quantification. (Tintinalli's Emergency Medicine)
Behavioural Signs (Observable in All Ages)
| Sign | Details |
|---|---|
| Crying | High-pitched, persistent, inconsolable cry |
| Facial grimacing | Furrowed brow, quivering chin, clenched jaw, brow bulging, nasolabial deepening |
| Body posturing | Guarding, arching, rigidity, drawing knees to chest |
| Leg movement | Kicking, drawing up legs, tensing thighs |
| Restlessness | Shifting, writhing, inability to be still |
| Withdrawal | Pulling away when touched in a specific area - a localizing clue |
| Disturbed sleep | Pain-related waking, refusal to sleep |
| Inconsolability | Cannot be soothed by parent, toy, or distraction |
| Protective posturing | Child holds or guards a body part |
| Reduced activity | Stops playing, becomes very still or limp |
Part 2 - Age-Based Assessment with Validated Tools
A. Neonates and Infants (0 - 3 years)
Cannot self-report. Rely entirely on observation.
Neonatal Infant Pain Scale (NIPS) - for preterm and full-term neonates up to 6 weeks:
| Category | 0 Points | 1 Point | 2 Points |
|---|---|---|---|
| Facial expression | Relaxed | Contracted (grimace) | - |
| Cry | Absent | Mumbling/whimpering | Vigorous/screaming |
| Breathing | Relaxed | Different from baseline | - |
| Arms | Relaxed | Flexed or stretched | - |
| Legs | Relaxed | Flexed or stretched | - |
| Alertness | Sleeping/calm | Uncomfortable/agitated | - |
Score >3 = need for analgesia.
FLACC Scale - for infants and children up to 3-4 years old (also used in non-verbal/cognitively impaired patients at any age):
| Category | 0 | 1 | 2 |
|---|---|---|---|
| Face | No expression or smile | Occasional grimace, withdrawn, disinterested | Frequent/constant quivering chin, clenched jaw |
| Legs | Normal or relaxed | Uneasy, restless, tense | Kicking, or drawn up |
| Activity | Lying quietly, normal position | Squirming, shifting, tense | Arched, rigid, or jerking |
| Cry | No cry | Moans/whimpers, occasional complaint | Crying steadily, screams, frequent complaints |
| Consolability | Content, relaxed | Reassured by touch, hugging, talking; distractible | Difficult to console or comfort |
Score 0-10. Score >6 = need for analgesia.
(Harriet Lane Handbook, 23rd Edition; Tintinalli's Emergency Medicine)
B. Preschool Children (3 - 8 years)
Beginning to self-report but need picture-based tools.
Faces Pain Scale - Revised (FPS-R) - usable from age 3:
- Show child a series of faces ranging from neutral (no pain) to distressed (maximum pain)
- Child points to the face that matches how they feel
- Scores range 0 - 10
Wong-Baker FACES Scale - widely used from age 3-4+:
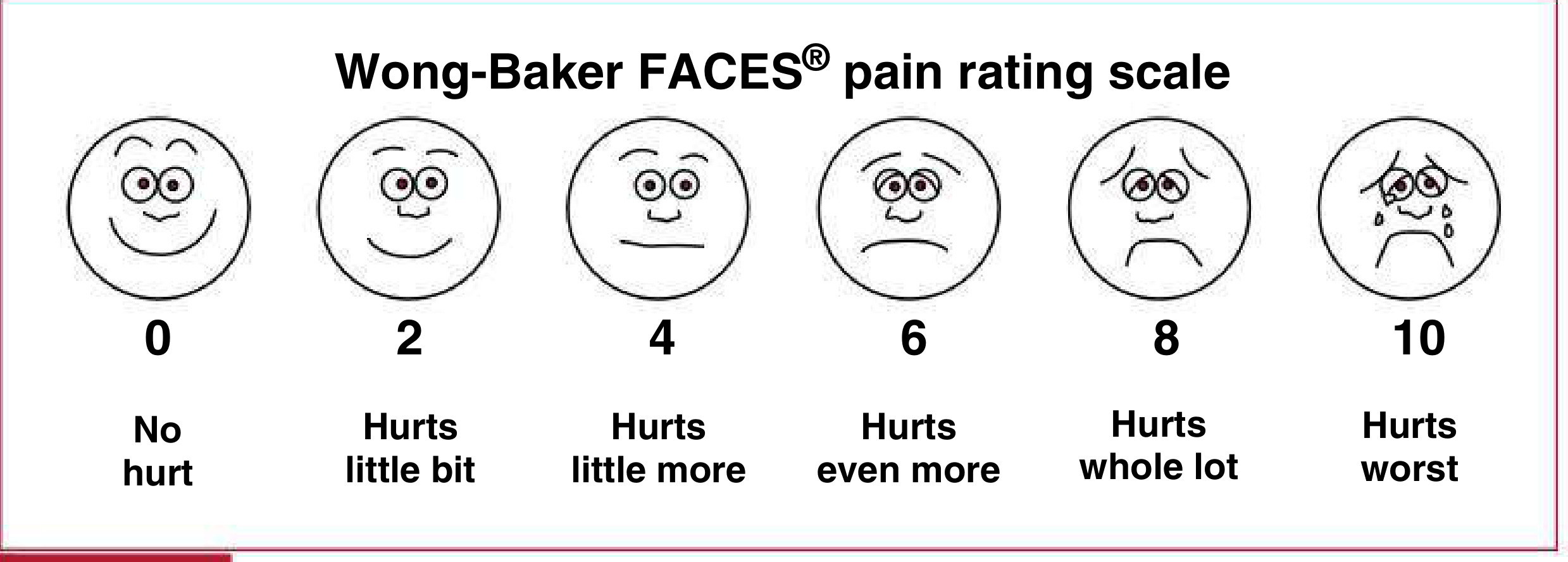
The child simply points to the face that best matches their pain.
C. School-Age and Adolescents (6 - 18 years)
Can use numerical self-report tools.
Numeric Rating Scale (NRS-11):
- "On a scale of 0 to 10, where 0 is no pain and 10 is the worst pain you can imagine, how much does it hurt?"
- Valid and reliable from age 6-7 upward
- No equipment needed
Visual Analog Scale (VAS):
- A 100 mm horizontal line from "no pain" to "worst pain"
- Child makes a mark on the line
- Distance measured in mm = pain score
- Valid from age 8 upward; sensitive to change with treatment
Age-to-Tool Quick Reference
| Age | Recommended Tool(s) |
|---|---|
| 0 - 6 weeks (neonate) | NIPS |
| 6 weeks - 3 years (infant/toddler) | FLACC Scale |
| 3 - 7 years (preschool) | Wong-Baker FACES / FPS-R |
| 6 - 18 years (school age/adolescent) | NRS-11, VAS |
| Any age with cognitive impairment | Revised FLACC (r-FLACC) |
Part 3 - How to Localise WHERE the Pain Is
1. Verbal Children (Age 3+) - Ask Directly
Use age-appropriate language:
- "Show me where it hurts" - let them point or place their own hand
- "Does it hurt here? What about here?" while touching systematically
- Use a body map/pain chart - a front-and-back outline of a child's body; ask them to colour or mark where it hurts
2. Non-Verbal/Pre-Verbal Children - Observe and Elicit
| Technique | What You Do | What It Tells You |
|---|---|---|
| Systematic palpation | Gently press each body region in sequence; watch face and hands | Child grimaces, pulls away, cries, or goes rigid at the painful area |
| Watch for guarding | Observe spontaneous posturing - which area do they protect or hold? | Child keeping hand on belly, ear, leg |
| Provocation test | Gently move the suspected area (limb, neck, abdomen) | Pain on movement = musculoskeletal or peritoneal |
| Rebound tenderness | In abdomen: press slowly then release rapidly | Release pain = peritoneal irritation |
| Percussion | Tap body wall gently over different areas | Pain on percussion pinpoints visceral or bone source |
| Parent observation | Ask parent: "Which part does she hold? What makes it worse?" | Invaluable for non-verbal children |
3. Regional Examination Clues by Body Area
| Region | Signs That Point to That Area |
|---|---|
| Head | Holding head, pressing temples, photophobia, phonophobia, rocking, refusing to look at light; in infants - high-pitched cry, bulging fontanelle |
| Ears | Pulling or tugging at one or both ears, rolling head, crying with jaw movement or lying down |
| Throat/mouth | Drooling, refusing to swallow, pawing at mouth, hoarse cry |
| Chest | Grunting respirations, splinting (holding breath to avoid deep breathing), tachypnea, leaning forward, holding chest wall |
| Abdomen | Knees drawn to chest, rigid or tense abdomen on palpation, guarding (tensing on approach of examiner's hand), rebound tenderness, facial grimace localised to palpation of a specific quadrant, refusal to move |
| Musculoskeletal / limb | Not moving a limb (pseudoparalysis), refusing to weight-bear, crying with passive range of motion, swelling, point tenderness on palpation |
| Back / spine | Abnormal posture, refusal to bend, pain on spinal percussion (vertebral tenderness) |
| Genitourinary | Holding groin/genitals, crying with urination, distended bladder |
4. The Pain Quality Gives Diagnostic Clues
| Pain Quality | Type | Common Cause |
|---|---|---|
| Sharp, stabbing, well-localised | Somatic (skin, muscle, bone, joint) | Fracture, laceration, muscle injury |
| Deep, dull, crampy, poorly localised | Visceral (organs) | Appendicitis, intussusception, renal colic |
| Burning, shooting, electric, "pins and needles" | Neuropathic | Nerve injury, post-herpetic, neuropathy |
| Colicky (comes and goes in waves) | Visceral / hollow organ | Bowel obstruction, intussusception, biliary/renal colic |
Part 4 - Children with Special Needs / Cognitive Impairment
These children are at high risk of undertreated pain because their behavioral responses to pain may be atypical. Key observable categories include:
| Category | Examples |
|---|---|
| Vocalization | Crying, moaning, gasping, sharp intake of breath |
| Facial reaction | Grimacing, squinting, frowning, teeth grinding |
| Interaction | Inconsolable, withdrawn, seeking comfort |
| Sleep | Disturbed sleep, increased or decreased sleep |
| Activity/tone | Restlessness, startles easily, pulls away when touched, posturing (arching/stiffening) |
| Physiologic | Tachycardia, pallor, sweating, tears |
| Atypical | Breath-holding, self-injurious behaviour, laughter (paradoxical) |
Use the r-FLACC (Revised FLACC) - same scoring 0-10, but parent-individualised to the specific child's pain behaviors.
(Harriet Lane Handbook, 23rd Edition - from Hauer & Houtrow, Pediatrics 2017)
Part 5 - Key Clinical Principles
- Reassess after every intervention - pain score should be recorded before and after any treatment, with timing appropriate to the drug's expected onset
- Never assume a non-communicating child feels no pain - cognitive disability does not equal absence of pain perception
- Parent input is essential - parents know their child's baseline and can identify deviations that clinicians will miss
- Physiologic signs alone are insufficient - vital sign changes are non-specific; always combine with behavioral observation
- Use the same scale consistently within an institution for serial comparisons
- A child who goes very still (not playing, not engaging) may be in MORE pain than one who is crying - profound pain can cause withdrawal rather than distress
Sources: The Harriet Lane Handbook 23rd Edition (Johns Hopkins); Tintinalli's Emergency Medicine 9th Edition; Katzung Basic & Clinical Pharmacology 16th Edition; Cummings Otolaryngology; Canadian Paediatric Society Pain Assessment Guidelines 2024
This is a shared conversation. Sign in to Orris to start your own chat.