Supracondylar fracture of humerus treatment
Reading File
Finding Sources
Searching PubMed
"supracondylar fracture" AND "humerus" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
supracondylar fracture humerus classification treatment K-wire
Loading Image
Loading Image
Here is a comprehensive overview of supracondylar fracture of the humerus treatment, drawn from Bailey & Love's Surgery, Rosen's Emergency Medicine, and Tintinalli's Emergency Medicine.
Supracondylar Fracture of the Humerus — Treatment
Overview
Supracondylar humeral fractures are the most common elbow fracture in children (ages 5–10) but also occur in adults from high-velocity injuries. The distal fragment displaces posteriorly in extension-type (>95%) and anteriorly in flexion-type (<5%). Treatment is guided by the modified Gartland classification.
Gartland Classification & Treatment Algorithm
| Type | Description | Treatment |
|---|---|---|
| Type I | Minimal/no displacement | Immobilization: long-arm posterior splint/collar & cuff, elbow at 75–90°, neutral forearm rotation; 3 weeks; discharge with 24–48 hr follow-up |
| Type IIA | Displaced, posterior cortex intact, no rotation | Closed reduction + above-elbow cast (elbow flexed 110–120°) using intact posterior periosteum as tension band; 3–4 weeks |
| Type IIB | Displaced, posterior cortex intact, WITH rotation | Closed reduction + percutaneous K-wire fixation (rotation makes cast alone unreliable) |
| Type III | Completely displaced, no cortical contact, periosteal contact present | Emergent orthopedic consultation; closed reduction + percutaneous K-wire fixation; admit for neurovascular monitoring |
| Type IV | Multidirectional instability, complete circumferential periosteal disruption | Closed or open reduction + K-wire fixation; open reduction if closed fails |
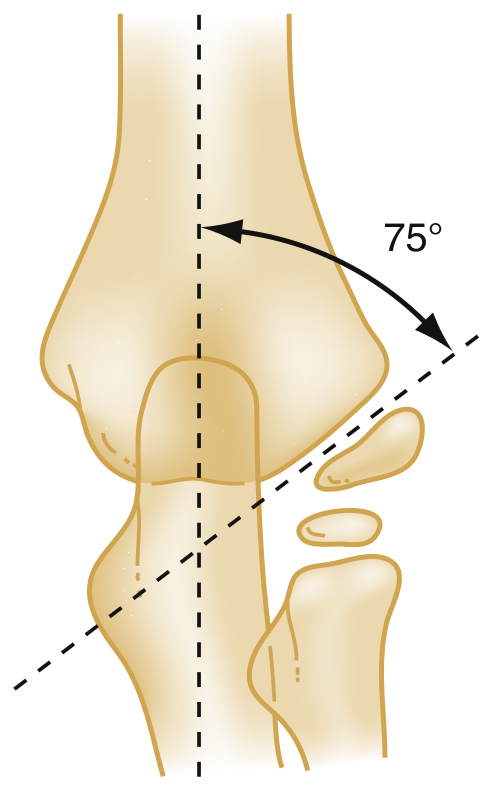
Key radiographic aid: Baumann's angle (~75°) on AP film — angle between humeral shaft axis and capitellum growth plate — used to confirm acceptable reduction.
Closed Reduction Technique (Types II–III)
- Procedural sedation/anesthesia
- Assistant fixes the upper arm; operator grasps the wrist
- Apply steady traction in line with the limb (forearm in neutral/thumb-up)
- Correct medial/lateral displacement with the free hand at the elbow
- Once length and angulation corrected: thumb on anterior proximal fragment, fingers behind olecranon → gently flex elbow to reduce distal fragment
- Immobilize in above-elbow cast at 110–120° flexion (if no vascular risk)
- Do NOT hyperflex if there is significant swelling → risk of vascular compromise
>20° of angulation after reduction warrants orthopedic consultation for K-wire pinning.
Percutaneous K-Wire Fixation
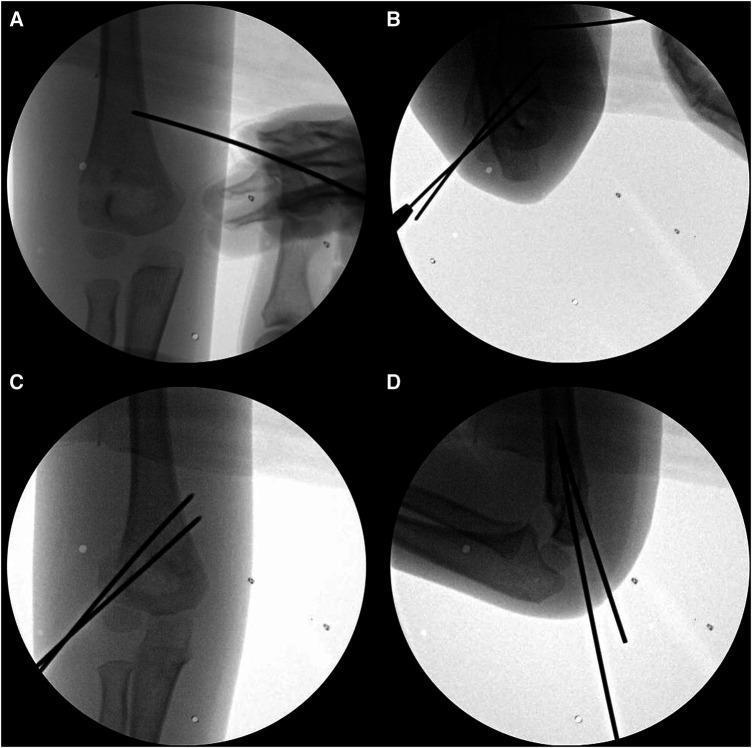
- Standard approach: 2 lateral divergent pins ± 1 medial pin
- If periosteal hinge is broken, K-wires are mandatory, supplemented by above-elbow cast
- Supplemented with an above-elbow cast post-operatively
- Trend toward delayed fixation (up to 24 hrs) is now accepted unless emergent indications exist
Timing of Surgery
| Indication | Urgency |
|---|---|
| Vascular insufficiency / white pulseless hand | Emergent (immediate) |
| Open fracture | Emergent |
| Irreducible fracture | Emergent |
| Nerve injury / displaced without vascular compromise | Urgent (within 24 hrs) |
| Stable displaced (no neurovascular compromise) | Semi-urgent (delayed fixation acceptable) |
Neurovascular Complications — Management
White Pulseless Hand
- Surgical emergency: immediate reduction
- If pulse does not return after reduction → vascular exploration by vascular surgeon
Pink Pulseless Hand (controversial)
- If adequate limb perfusion, no compartment syndrome, and no neurological deficit:
- Reduce and stabilize the fracture
- Expectant approach to vascular injury — pulse often returns within 24–48 hours
Nerve Injury
- Common (often anterior interosseous nerve with extension-type); usually a neuropraxia
- Most resolve with fracture reduction, stabilization, and resolution of swelling
- No immediate surgical exploration unless vascular injury co-exists
Volkmann's Ischaemic Contracture
- Rare but feared complication from missed compartment syndrome due to excessive swelling
- Do not place elbow in deep flexion if significant swelling is present
- If deep flexion is the only way to hold the fracture → proceed to K-wire fixation instead
Malunion
- Cubitus varus ("gunstock deformity") is the most common malunion — from inadequate reduction of varus angulation
- The elbow remodels flexion-extension plane deformity well; varus/valgus malunion remodels poorly
- Requires careful attention to reduction quality and K-wire placement to avoid angular malunion
Flexion-Type Fractures
- Rare (<5%); distal fragment displaced anteriorly
- More difficult to reduce and maintain
- Usually require K-wire fixation for stability
Sources: Bailey & Love's Short Practice of Surgery, 28th ed.; Rosen's Emergency Medicine, 9th ed. (Ch. 44); Tintinalli's Emergency Medicine, 9th ed. (Ch. 270)
This is a shared conversation. Sign in to Orris to start your own chat.