breast implant rupture; intracapsular and extracapsular
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast implant rupture" AND intracapsular
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full detailed answer:
Breast Implant Rupture: Intracapsular vs. Extracapsular
Background
Approximately 3.5 million people in the United States have breast implants. Rupture risk increases with implant age, typically after 20 years, and is most often spontaneous - though blunt trauma can cause it as well. The type and extent of rupture differs significantly between saline and silicone implants, and in silicone implants, the key distinction is whether rupture is intracapsular or extracapsular.
- Tintinalli's Emergency Medicine, p. 703
The Fibrous Capsule
After implant placement, the body invariably forms a fibrous periprosthetic capsule around the implant. This capsule is the anatomical boundary that defines the rupture classification:
- Intracapsular rupture: The implant shell (plastic envelope) breaks, but leaked silicone remains contained within the fibrous capsule.
- Extracapsular rupture: Silicone escapes beyond the fibrous capsule into surrounding breast tissue, and potentially into axillary lymph nodes or distant sites.
Saline Implants
Saline rupture is clinically obvious and straightforward to diagnose:
-
The breast visibly deflates and asymmetry is immediately apparent on physical exam.
-
The saline is absorbed harmlessly by the body.
-
Typically painless; outpatient follow-up and elective implant exchange are appropriate.
-
When the clinical exam is equivocal, mammography easily visualizes the collapsed implant shell.
-
Current Surgical Therapy 14e, p. 826
Silicone Implant Rupture
Silicone rupture is more diagnostically challenging because the gel is cohesive and may not leak visibly or cause symptoms - especially in intracapsular cases.
Intracapsular Rupture
- The implant shell is broken but silicone gel stays inside the fibrous capsule.
- Often clinically silent - no change in breast shape, no palpable mass, no pain.
- Mammography has low sensitivity (11%-69%) for detection and may appear normal.
- Ultrasound can be helpful, showing disruption of the implant shell with the classic "stepladder" sign (multiple parallel echogenic lines within the implant).
- MRI is the gold standard (sensitivity and specificity >90%) and is the recommended screening modality.
Classic MRI signs of intracapsular rupture:
| Sign | Description |
|---|---|
| Linguini sign (also "wavy line" sign) | The collapsed, ruptured implant shell floats within the escaped silicone gel, appearing as multiple curvilinear dark lines |
| Keyhole sign | Silicone tracking into implant folds |
| Salad oil sign | Bright dot of water-like material within the implant (seen on T2) - represents water droplets within silicone |
Note: False-positive MRI interpretations can occur when normal implant folds are mistaken for the wavy/linguini sign.
MRI (T2-weighted) - Intracapsular Rupture:
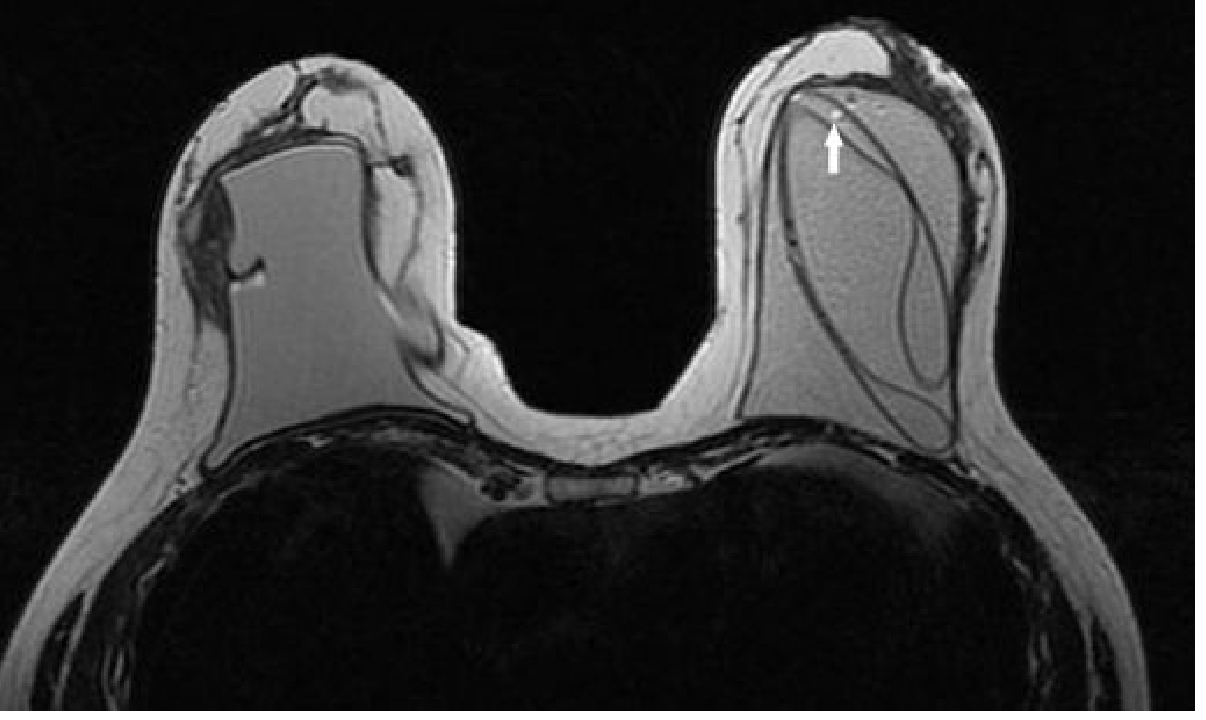
T2-weighted fast spin-echo MRI: the plastic shell of the left implant is seen floating within the silicone (linguini/wavy line sign). The white arrow indicates the bright "salad oil" sign (tiny water droplet within silicone).
- Grainger & Allison's Diagnostic Radiology, p. 1659
Extracapsular Rupture
- The fibrous capsule has also been breached; silicone gel escapes freely into breast tissue.
- More likely to produce symptoms: palpable mass, breast pain, firmness, or change in shape.
- Free silicone can migrate to axillary lymph nodes, chest wall, or distant sites.
- Silicone granulomas form as a foreign body reaction to extruded silicone.
Imaging findings in extracapsular rupture:
- Ultrasound: Highly useful - shows free silicone and silicone granulomas with the characteristic "snowstorm" appearance (strongly echogenic, posterior acoustic shadowing).
Ultrasound - Extracapsular Silicone Granuloma:
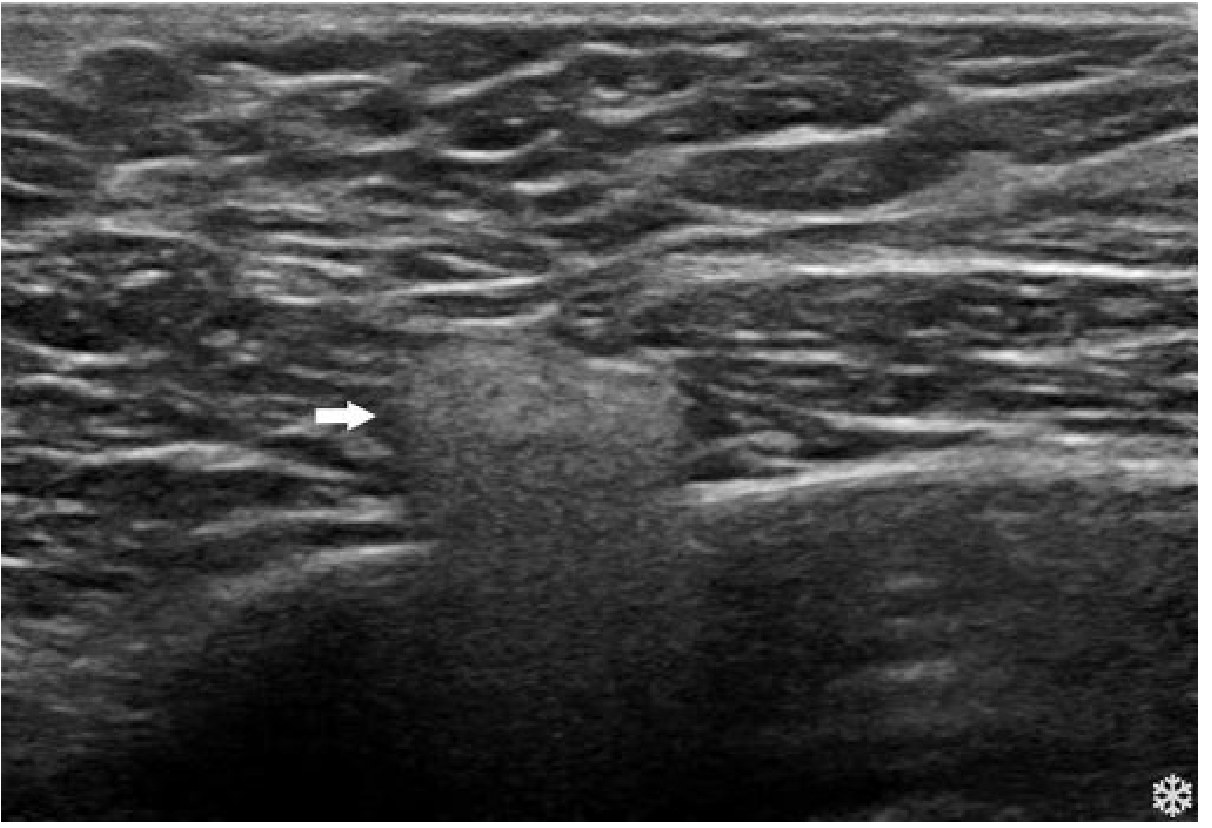
US image: silicone granuloma adjacent to breast implant (arrow) with the characteristic "snowstorm" echogenic appearance.
- Silicon-containing axillary lymph nodes may be detected on ultrasound.
- MRI remains the most accurate overall modality (sensitivity 80%-90%, specificity 90%-97%), demonstrating the linguini sign within the implant AND silicone signal outside the capsule (as a bulge or free silicone in breast tissue).
MRI - Extracapsular and Combined Ruptures:
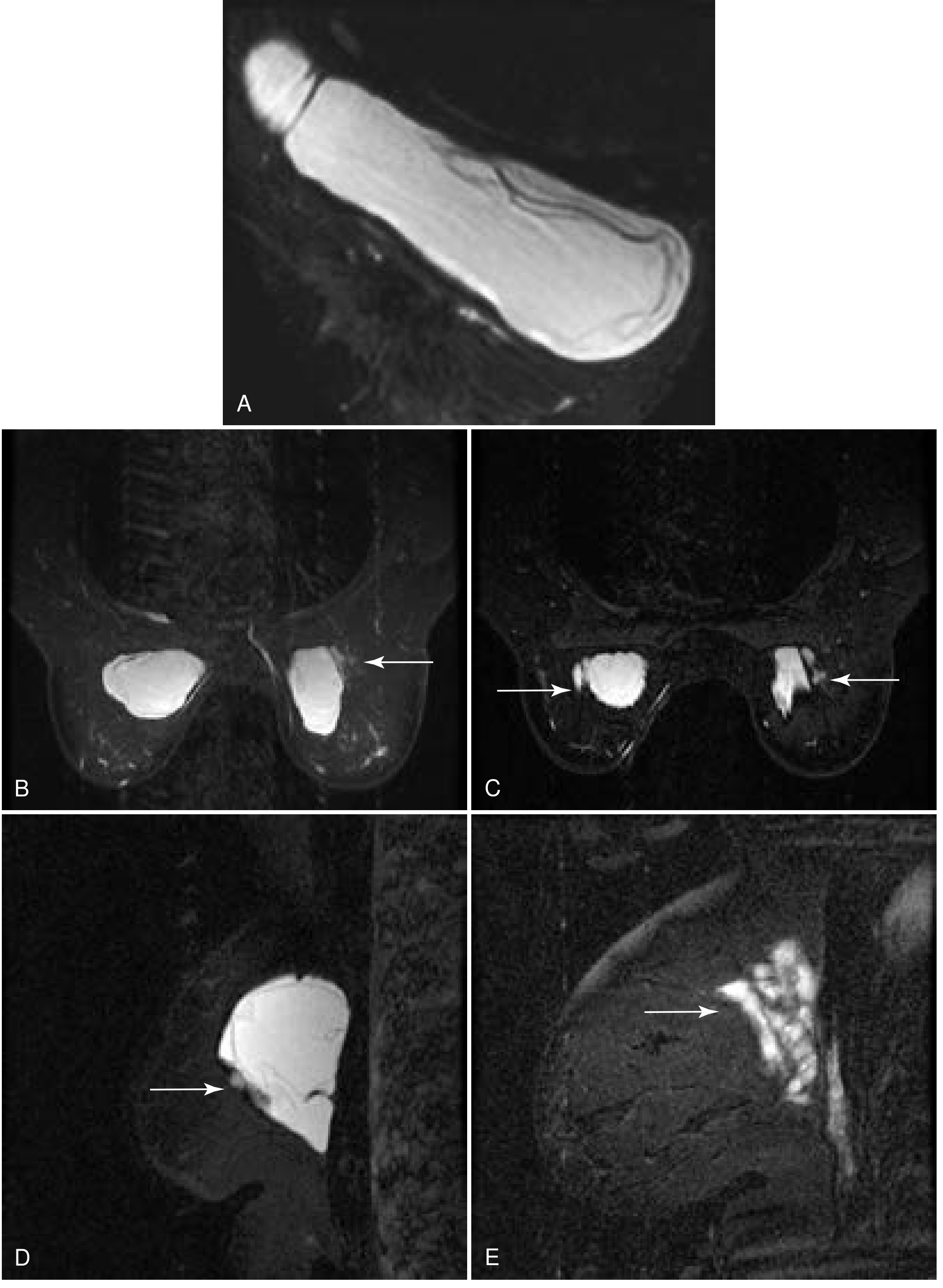
(A) Axial MRI: extracapsular rupture - silicone bulge in axillary portion of implant; linguini sign within implant. (B-C) Axial three-point Dixon MRI: bilateral extracapsular rupture with extravasated silicone laterally (arrows). (D) Sagittal view: intracapsular + extracapsular rupture; silicone anterior to implant. (E) Extravased silicone far lateral within breast tissue.
- Current Surgical Therapy 14e, p. 826-827
Comparison Table
| Feature | Intracapsular | Extracapsular |
|---|---|---|
| Silicone location | Within fibrous capsule | Beyond fibrous capsule |
| Clinical presentation | Often silent | Palpable mass, pain, shape change |
| Breast shape | Usually preserved | May be distorted |
| Mammography | Low sensitivity (11%-69%) | May show free silicone |
| Ultrasound | Stepladder sign; less sensitive | Snowstorm appearance; silicone granulomas; axillary nodes |
| MRI | Linguini/wavy line, keyhole, salad oil signs | Linguini sign + free silicone outside capsule |
| MRI sensitivity/specificity | >90% / >90% | 80%-90% / 90%-97% |
| Granuloma formation | No | Yes (foreign body reaction) |
| Lymph node involvement | No | Possible axillary spread |
Management
-
Acutely ruptured silicone implants may present with an inflamed, painful breast mass due to silicone extravasation - treatment involves surgical removal of the implant and capsule (capsulectomy).
-
Patients should be reassured that there is no systemic danger from silicone leakage (no evidence of systemic toxicity or increased cancer risk).
-
The FDA recommends MRI screening starting 5-6 years after implant placement and every 2-3 years thereafter for silent rupture detection in silicone implants.
-
Extracapsular rupture generally requires surgical intervention; asymptomatic intracapsular rupture management can be individualized.
-
Tintinalli's Emergency Medicine, p. 703; Current Surgical Therapy 14e, p. 826-827; Grainger & Allison's Diagnostic Radiology, p. 1659
Additional Note: BIA-ALCL
Ultrasound is also highly sensitive for detecting peri-implant fluid, which is the hallmark presentation of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) - a rare T-cell lymphoma associated particularly with textured implants. This should be distinguished from rupture-related fluid collections. - Current Surgical Therapy 14e, p. 827
satellite nodules
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"satellite nodules" AND "breast cancer"
Finding Sources
Finding Sources
Searching PubMed
"satellite nodules" AND "breast cancer" AND staging
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I now have everything needed for a thorough answer. Here it is:
Satellite Nodules in Breast Cancer
Definition
Satellite (skin) nodules in breast cancer are ipsilateral macroscopic tumor nodules in the skin of the same breast, separate from but associated with the primary tumor. They represent direct tumor extension through dermal lymphatics or subcutaneous spread to the overlying skin, appearing as discrete, separate tumor deposits on or just under the breast skin surface.
They are distinct from the primary mass and must be macroscopically visible - microscopic dermal invasion alone does not qualify.
TNM Staging - T4b Classification
Satellite nodules are a T4 feature under the AJCC/UICC 8th Edition TNM system, placing the primary tumor in the T4b category regardless of primary tumor size:
| Stage | Criteria |
|---|---|
| T4 | Tumor of any size with direct extension to chest wall and/or skin (ulceration or macroscopic nodules); invasion of the dermis alone does not qualify as T4 |
| T4a | Extension to the chest wall (invasion/adherence to pectoralis muscle alone does NOT qualify) |
| T4b | Ulceration and/or ipsilateral macroscopic satellite nodules and/or edema (including peau d'orange) of the skin - provided it does not meet criteria for inflammatory carcinoma |
| T4c | Both T4a and T4b present |
| T4d | Inflammatory carcinoma |
- Schwartz's Principles of Surgery 11e, TNM table; Fischer's Mastery of Surgery 8e, Table 66.1
The key qualifier: the satellite nodules must be macroscopic (visible/palpable) and ipsilateral. Dermal invasion alone without skin ulceration or satellite nodules does not reach T4.
Clinical Context: Locally Advanced Breast Cancer (LABC)
Satellite skin nodules are a feature of locally advanced breast cancer (LABC), which includes:
- Large primary tumors (>5 cm)
- Tumors involving the chest wall
- Skin involvement, ulceration, or satellite skin nodules
- Inflammatory carcinoma
- Bulky or fixed axillary nodes
- Clinically apparent internal mammary or supraclavicular nodal involvement
LABC corresponds to stages IIB, IIIA, IIIB, and IIIC. T4b disease (satellite nodules) specifically maps to Stage IIIB when combined with N0-N2 nodal status.
- Sabiston Textbook of Surgery, p. 1411-1412
T4b vs. Inflammatory Carcinoma (T4d) - Key Distinction
| Feature | T4b (Satellite nodules/peau d'orange) | T4d (Inflammatory carcinoma) |
|---|---|---|
| Skin appearance | Discrete satellite nodules, ulceration, or focal edema | Diffuse erythema, edema, warmth involving >1/3 of breast skin |
| Lymphatic invasion | May or may not be present | Hallmark: diffuse dermal lymphatic involvement |
| Discrete mass | Usually present | Often absent |
| Onset | Variable | Rapid (weeks to 3 months) |
| Staging | T4b → Stage IIIB | T4d → Stage IIIB (or higher with nodal involvement) |
| Sentinel node biopsy | May be considered | Contraindicated (high false-negative rate; ALND always performed) |
Treatment Implications
Because T4b disease (including satellite nodules) represents locally advanced cancer:
-
Multimodal treatment is standard: neoadjuvant chemotherapy + mastectomy + post-mastectomy radiotherapy (PMRT) + appropriate systemic therapy.
-
Surgery alone or RT alone has historically been inadequate, with local relapse rates of 30%-50% and mortality of ~70% with single-modality treatment.
-
With combined-modality treatment, locoregional recurrence rates have fallen significantly.
-
Immediate breast reconstruction is generally deferred given the need for PMRT.
-
Sabiston Textbook of Surgery, p. 1411-1412
Summary
Satellite nodules in breast cancer = ipsilateral macroscopic skin tumor deposits separate from the primary tumor → classify as T4b (AJCC 8th ed.) → Locally Advanced Breast Cancer, Stage IIIB → requires multimodal treatment (neoadjuvant chemotherapy, mastectomy, radiotherapy).
axillary clearance
Finding Sources
Finding Sources
Searching PubMed
"axillary lymph node dissection" AND "breast cancer" AND "sentinel node"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the material needed for a thorough, well-illustrated answer.
Axillary Clearance (Axillary Lymph Node Dissection - ALND)
Definition
Axillary clearance, or axillary lymph node dissection (ALND), is the surgical removal of the axillary lymph node-bearing fat pad. In breast cancer surgery, a standard ALND removes levels I and II of the axilla and typically yields 10-30 lymph nodes (a minimum of 10 is required to be considered adequate).
Axillary Levels - Anatomy
The axilla is divided into three levels defined by their relationship to the pectoralis minor muscle:
| Level | Location | Nodes |
|---|---|---|
| Level I | Inferolateral to pectoralis minor | Majority of axillary nodes; the usual sentinel node location |
| Level II | Posterior (deep) to pectoralis minor | Also includes interpectoral (Rotter's) nodes |
| Level III | Superomedial to pectoralis minor (apex) | Highest level; removed only if grossly involved |
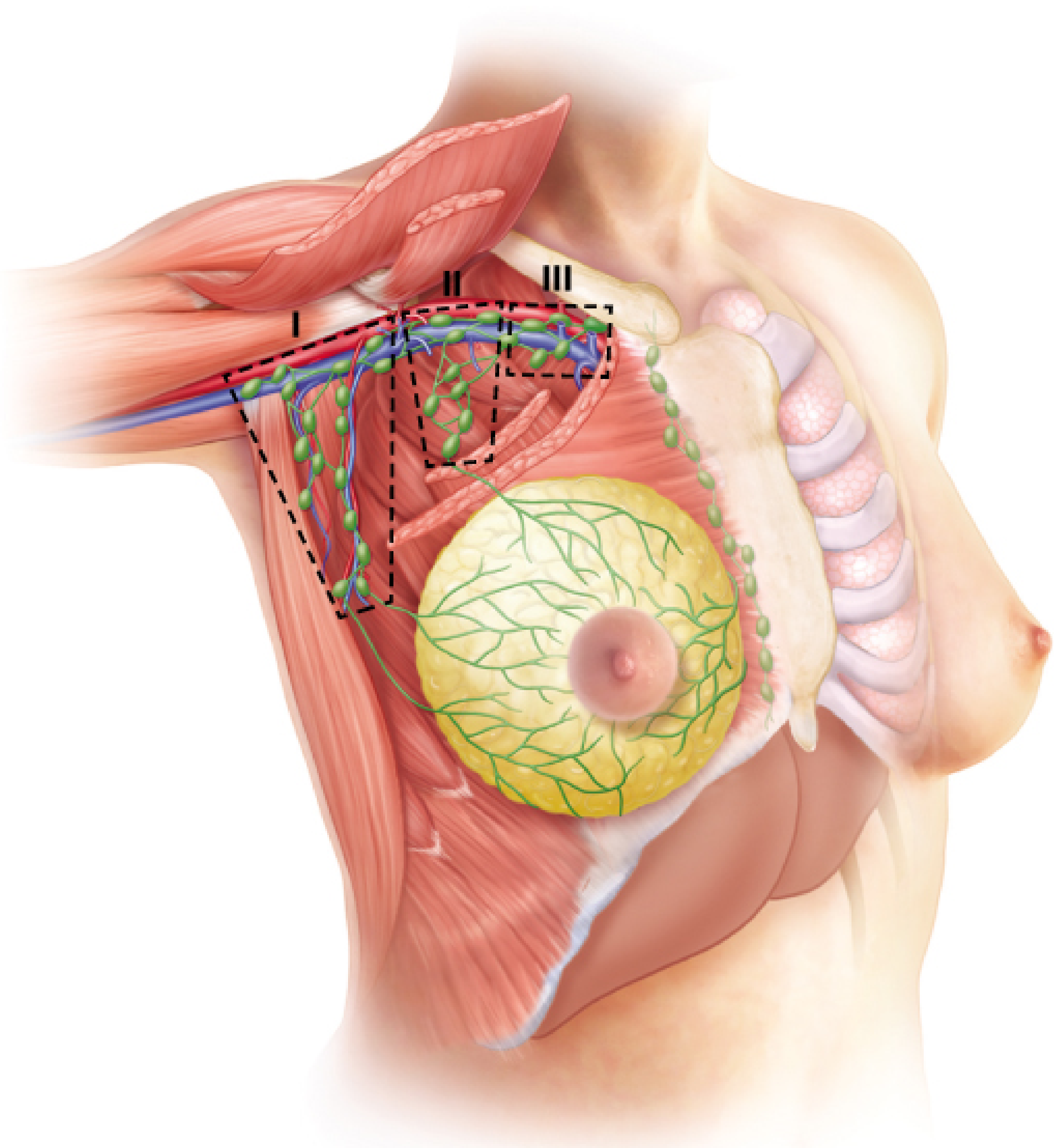
Anatomical illustration showing the three levels of axillary lymph nodes (I, II, III) in relation to the pectoralis minor muscle and breast lymphatic drainage pathways.
- Fischer's Mastery of Surgery 8e, p. 1539; Current Surgical Therapy 14e, p. 807
Why Levels I + II (not just I alone)?
- Level I alone risks missing "skip metastases" that bypass level I and go directly to level II or III - this occurs in 20%-25% of patients.
- Skip metastases to level III with levels I and II negative occur in only 2%-3% of cases - so routine level III clearance is not warranted unless grossly involved.
Surgical Anatomy and Key Structures to Protect
The boundaries of dissection are:
- Superior: Axillary vein
- Medial: Chest wall / serratus anterior
- Anterior: Pectoralis major muscle
- Posterior/lateral: Latissimus dorsi muscle
Nerves at risk - identification and preservation are mandatory:
| Nerve | Innervates | Injury consequence |
|---|---|---|
| Long thoracic nerve (of Bell) | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Latissimus dorsi | Arm/shoulder weakness and dysfunction |
| Medial pectoral nerve | Pectoralis major and minor | Denervation atrophy of pectoralis |
| Intercostobrachial nerve(s) | Skin of medial upper arm | Numbness/paresthesia in underarm and posterior shoulder (often sacrificed) |
- Current Surgical Therapy 14e, p. 807-808
Operative Technique (Steps)
- Incision: A separate transverse axillary incision is used for lumpectomy cases; ALND can be done through the mastectomy wound in mastectomy patients.
- Entry: Incise the clavipectoral fascia at the lateral border of pectoralis major, progressing superiorly toward the apex.
- Lateral approach to identify the axillary vein (safest - no critical structures laterally): follow the latissimus dorsi muscle superiorly to find the vein where it crosses anterior to the latissimus tendon.
- Dissect the axillary vein free, clip and divide tributaries, progressing laterally to medially.
- Identify and protect the thoracodorsal neurovascular bundle (enters deeply in the center of the specimen, halfway between chest wall and latissimus).
- Identify and protect the long thoracic nerve (runs deep along serratus anterior).
- Retract pectoralis minor to access Level II nodes; use appendiceal retractor or separate pectoralis minor fibers for Level III if needed.
- Close suction drain placed; clavipectoral fascia closed with absorbable sutures; skin closed subcuticularly.
- Current Surgical Therapy 14e, p. 807-808; Fischer's Mastery of Surgery 8e, p. 1538-1540
Indications for ALND
ALND is currently indicated in:
- Clinically node-positive disease (biopsy-proven) undergoing primary surgery (without neoadjuvant chemotherapy or as a contraindication to it)
- Inflammatory breast cancer (SLNB is contraindicated due to high false-negative rate)
- Residual nodal disease after neoadjuvant chemotherapy (ypN+ or cN2/cN3 before treatment)
- Positive sentinel node in situations not meeting Z0011 criteria (see below)
- Recurrent axillary disease
- Current Surgical Therapy 14e, p. 2322
ALND vs. Sentinel Lymph Node Biopsy (SLNB) - The Paradigm Shift
Sentinel Node Biopsy (SLNB)
SLNB using blue dye and/or technetium-99m sulfur colloid injected into the subareolar plexus has replaced ALND for axillary staging in clinically node-negative patients. The subareolar injection approach is standard because the entire breast drains through the subareolar plexus - allowing one set of sentinel nodes to represent the whole breast.
Key validation trials:
- Milan trial (2003): SLNB accuracy 96.9%, sensitivity 91.2%, specificity 100%; reduced arm pain and improved arm mobility vs. ALND
- NSABP B32: Equivalent overall survival, DFS, and regional control between SLNB alone (if negative) vs. SLNB + ALND
- ACOSOG Z0010: <0.5% axillary recurrence at 8.4-year median follow-up with SLNB alone in T1/T2 node-negative patients
- ALMANAC trial: Significantly lower lymphedema, sensory loss, drain use, and length of stay with SLNB vs. ALND
ACOSOG Z0011 Trial - Avoiding Completion ALND in Positive Sentinel Nodes
This landmark trial fundamentally changed practice for patients with limited sentinel node involvement:
Eligibility: Clinical T1-T2 invasive breast cancer, no palpable adenopathy, 1-2 positive sentinel nodes, treated with breast-conserving surgery + whole-breast irradiation + systemic therapy.
Randomized to: Completion ALND vs. sentinel node alone.
| Outcome | ALND | Sentinel node alone |
|---|---|---|
| 5-year overall survival | 91.8% | 92.5% |
| 5-year disease-free survival | 82.2% | 83.9% |
Conclusion: No inferior survival with sentinel node alone - completion ALND can be omitted in this selected population.
The key premise: systemic therapy decisions are now driven by tumor phenotype (ER/PR/HER2), not by the exact number of positive nodes, making complete ALND less relevant for risk stratification.
- Schwartz's Principles of Surgery 11e, p. 1913-1914; Current Surgical Therapy 14e, p. 2353-2365
Recent evidence (2023 meta-analysis, PMID 37495945): Confirms no significant difference in overall survival or disease-free survival between ALND and no axillary surgery in sentinel node-positive patients, supporting selective use of ALND.
Complications
| Complication | Rate | Details |
|---|---|---|
| Lymphedema (BCRL) | Most significant long-term morbidity | Risk increases with extent of dissection, radiation |
| Seroma | Up to 21% | Most common early complication |
| Wound infection | Up to 15% | |
| Hematoma | <2% | |
| Neuropathic pain / paresthesia | 15%-83% | Intercostobrachial nerve injury - numbness/discomfort in upper inner arm |
| Winged scapula | <1% | Long thoracic nerve injury |
| Arm/shoulder weakness | Uncommon | Thoracodorsal nerve injury |
Complication rates are consistently higher after ALND than SLNB across multiple prospective and randomized trials.
- Fischer's Mastery of Surgery 8e, p. 1540-1541
Postoperative Care
-
Closed suction drain is left in situ; removed when output ≤20-30 mL/24 hours
-
Early physiotherapy - range of motion and strengthening exercises from POD #1
-
Outpatient physiotherapy within 7-14 days for continued range of motion, strengthening, and lymphedema education
-
Fischer's Mastery of Surgery 8e, p. 1540
Summary
Axillary clearance (levels I+II ALND) was historically the standard axillary procedure for all node-positive breast cancer. SLNB has now replaced it for staging in clinically node-negative patients, and the Z0011 trial has further reduced the need for completion ALND even when 1-2 sentinel nodes are positive in selected patients undergoing breast-conserving surgery with radiation and systemic therapy. ALND remains the standard for clinically evident nodal disease, inflammatory breast cancer, residual post-neoadjuvant nodal disease, and cases outside Z0011 criteria.
This is a shared conversation. Sign in to Orris to start your own chat.