3. Normal flora help protect the body from pathogens A. By producing toxins that kill pathogens B. By competing with pathogenic bacteria C. By directly attacking pathogens D. By altering the body's immune response
Answer: B. By competing with pathogenic bacteria
How It Works
- Nutrients and essential minerals (e.g., iron) - normal flora scavenges these resources, leaving little for invading pathogens
- Attachment sites - they physically occupy receptors on host cells that pathogens need to bind to
- Space - dense microbial communities physically crowd out newcomers
Supporting Textbook Evidence
"The microbes provide needed metabolic functions, stimulate innate and regulatory immunity, and prevent colonization with unwanted pathogens... Within the colon, some bacteria wage interspecies warfare to establish their niche with bacteriocins (e.g., colicins produced by E. coli), other antibacterial proteins, and metabolites that deter other species from growing. These molecules also benefit the host by eliminating invading bacteria including Salmonella, Shigella, Clostridium difficile, Bacillus cereus, and other pathogens."
Why the Other Options Are Mostly Wrong
| Option | Assessment |
|---|---|
| A. Producing toxins that kill pathogens | Partially true - some flora produce bacteriocins (e.g., colicins). However, this is a secondary mechanism and not the primary/general answer; the question asks about the main protective mechanism. |
| B. Competing with pathogenic bacteria | CORRECT - This is the principal, well-established mechanism known as colonization resistance. |
| C. Directly attacking pathogens | Incorrect - normal flora are commensal organisms, not immune cells; they do not directly attack pathogens. |
| D. Altering the body's immune response | Normal flora does influence immune development (e.g., stimulating regulatory T cells and MALT), but this is not their primary mechanism for protecting against pathogens in the context of this question. |
Clinical Relevance
What are bacteriocins and how do they work?st most?
bacteriocins mechanism of action types colicins lantibiotics microbiology
The second most abundant antibody is A. IgG B. IgM C. Ig A D. IgE E. IgD then hwta is the 1st most?
Answer: C. IgA is the second most abundant antibody in serum
Serum Immunoglobulin Concentrations (Ranking)
| Rank | Class | Serum Concentration | Key Feature |
|---|---|---|---|
| 1st | IgG | 8-16 mg/mL | Major serum immunoglobulin; only Ig that crosses placenta |
| 2nd | IgA | 1.4-4 mg/mL | Guards mucosal surfaces |
| 3rd | IgM | 0.5-2 mg/mL | First antibody produced in response to infection |
| 4th | IgD | 0-0.4 mg/mL | On lymphocyte surface; activation/suppression |
| 5th | IgE | Trace only | Allergic and parasitic reactions |
Why IgG is #1
"IgG is the major class of immunoglobulin present in the serum... IgG is the only immunoglobulin class to cross the placenta and therefore is the most abundant immunoglobulin in newborns."
- It is the main product of secondary (memory) immune responses - repeated lifetime exposures keep levels high
- It has the longest half-life (~23 days) of all immunoglobulins
- It has 4 subclasses (IgG1-4) that collectively add up to the highest total
Why IgA is #2 (with an important nuance)
Which of the following is characteristically produced by the Th2 CD4 cells which provide help for antibody production, but not by Th1 cells? A. IFNy B. Lymphotoxin (TNFB) C. Granulocyte-macrophage colony-stimulating factor (GM-CSF) D. IL-4 E. IL-1 can u please explain this?
Answer: D. IL-4
Understanding the Th1 vs Th2 Divide
| Th1 | Th2 | |
|---|---|---|
| Job | Kill intracellular pathogens (viruses, bacteria inside cells) | Help B cells make antibodies; fight parasites |
| Signature cytokine | IFN-γ | IL-4 |
| Other cytokines | IL-2, TNF-α, Lymphotoxin (TNF-β) | IL-5, IL-13, IL-10 |
| Activates | Macrophages, cytotoxic T cells | B cells, eosinophils, mast cells |
| Inhibits | Th2 responses | Th1 responses |
Now Let's Go Through Each Option
What Does IL-4 Actually Do?
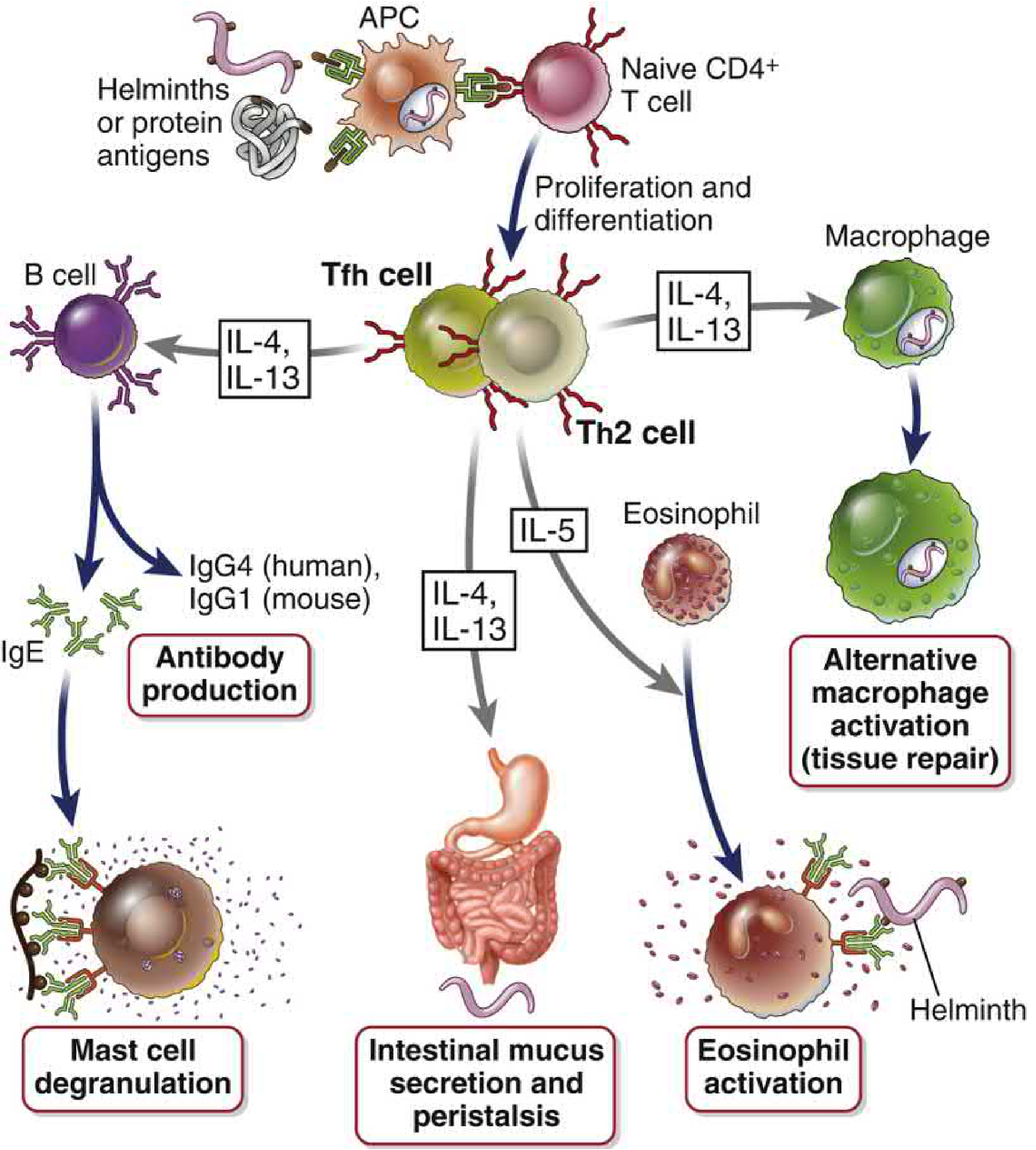
- B cell class switching to IgE - IL-4 (with IL-13) signals B cells to switch from making IgM to making IgE, which binds to mast cells and triggers allergic reactions
- B cell class switching to IgG4 - promotes this non-inflammatory subclass
- Th2 self-amplification - IL-4 drives naive CD4+ T cells to become more Th2 cells (positive feedback loop)
- Alternative macrophage activation - IL-4 and IL-13 suppress the classical (Th1-driven) macrophage activation, promoting tissue repair instead of killing
Why Does This Matter Clinically?
- Allergies and asthma: Overactive Th2/IL-4 responses cause IgE overproduction → mast cell sensitization → allergic reactions
- Parasitic infections: Th2/IL-4 responses are protective against helminths (worms)
- Dupilumab: A monoclonal antibody drug that blocks the IL-4 receptor, used to treat severe eczema and asthma - directly targeting this pathway
- HIV: The virus destroys CD4+ T cells, wiping out both Th1 and Th2 responses
nosocomial infections? meaning
Nosocomial Infections - Complete Explanation
Definition
"Nosocomial infections, also called hospital-acquired infections (HAI), are infections acquired during hospital care which are not present or incubating at the time of admission. Infections occurring more than 48 hours after admission are usually considered nosocomial."
The 48-Hour Rule
- Patient admitted → infection appears within 48 hours = community-acquired (patient already had it)
- Patient admitted → infection appears after 48 hours = nosocomial (acquired in hospital)
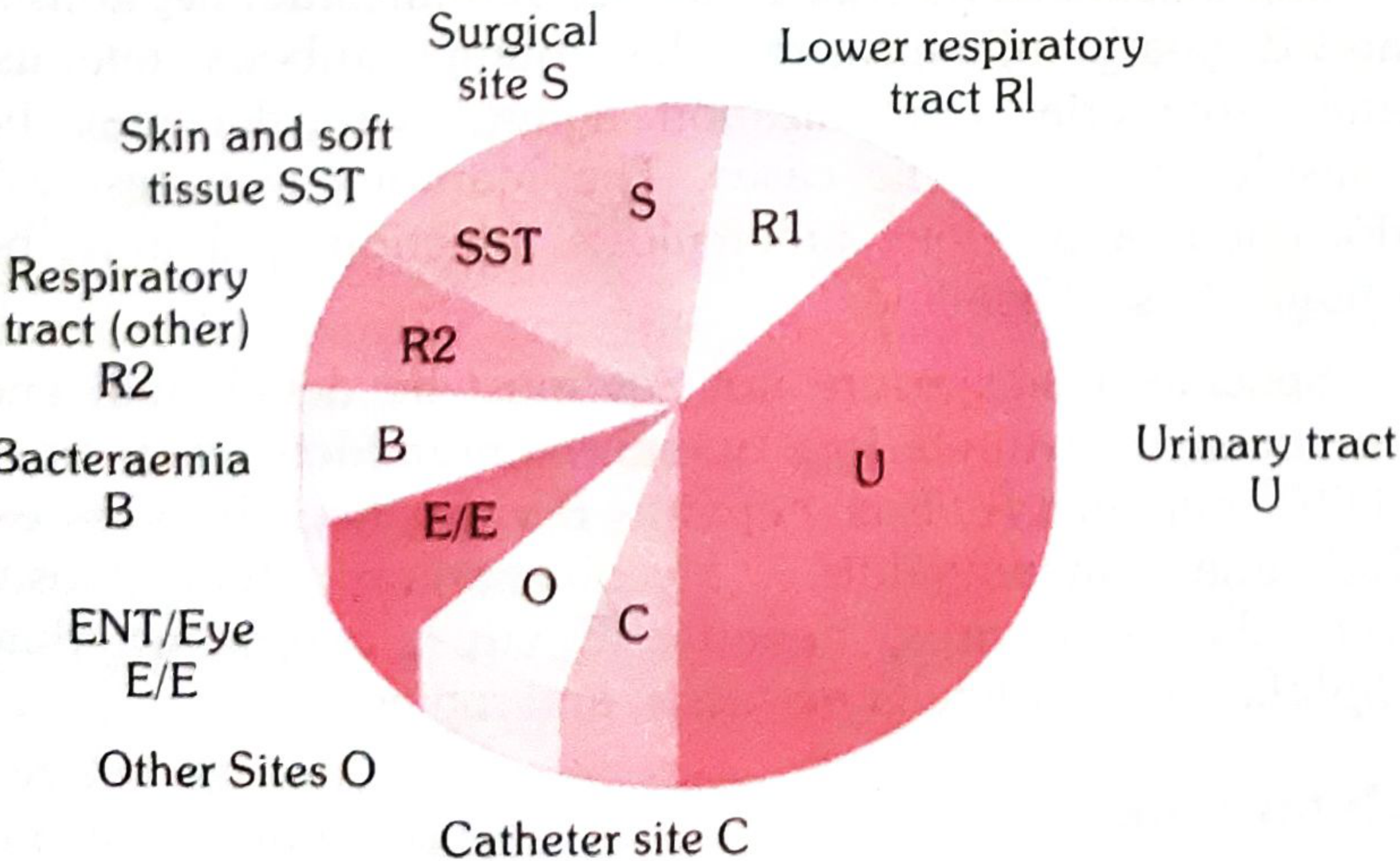
The 4 Most Common Nosocomial Infections
| # | Infection | Associated Device/Procedure |
|---|---|---|
| 1 | Urinary Tract Infection (UTI) | Urinary catheter (most common overall) |
| 2 | Surgical Site Infection (SSI) | Surgery/wounds |
| 3 | Pneumonia (HAP/VAP) | Mechanical ventilator (ventilator-associated pneumonia) |
| 4 | Bloodstream Infection (Bacteremia) | IV catheters, central lines |
Sites of Nosocomial Infection (Pie Chart from Park's)
Sources (Where Do the Germs Come From?)
- Other patients - infected wounds, respiratory infections, UTIs, TB
- Hospital staff - hands of doctors/nurses (most common route = unwashed hands)
- The hospital environment - contaminated equipment, dust, air, bedpans, catheters, IV lines
Routes of Spread
| Route | Example |
|---|---|
| Direct contact | Doctor/nurse hands touching patient (most common) |
| Droplet | Coughing/sneezing in open wards |
| Airborne | TB, measles in hospital |
| Hospital procedures | Catheterization, IV lines, surgery, dressings |
Who Is Most at Risk?
- Severely ill patients (weakened immune defenses)
- ICU patients (most procedures, most devices)
- Patients on corticosteroids (immunosuppressed)
- Urological ward patients
- Geriatric patients
- Newborns in special care units
Common Pathogens
| Pathogen | Common Nosocomial Infection |
|---|---|
| E. coli, Klebsiella | UTI (catheter-related) |
| Staphylococcus aureus (MRSA) | Wound infections, bloodstream |
| Pseudomonas aeruginosa | Pneumonia (VAP), burns |
| Candida spp. | Bloodstream (immunocompromised) |
| C. difficile | Diarrhea after antibiotics |
Prevention (Key Points)
- Hand hygiene - single most effective measure (WHO "Clean Care is Safer Care" 2009)
- Isolation of infectious patients
- Sterile technique for all invasive procedures
- Dust control - wet dusting, vacuum cleaning (not dry sweeping)
- Staff with infections must not work until cured
- Disinfection of instruments, bedpans, secretions
- Hospital Infection Control Committee to set and monitor policies
epistaxis meaning
Epistaxis = Nosebleed
Types by Location
| Type | Location | Frequency | Severity |
|---|---|---|---|
| Anterior | Front of nasal septum (Kiesselbach's plexus) | Most common (80%) | Usually mild, self-limiting, easy to control |
| Posterior | Back two-thirds of nasal cavity | Less common (20%) | More severe, harder to control, may need specialist |
Common Causes
| Category | Examples |
|---|---|
| Local/Trauma | Nose picking, dry weather, nose blowing hard, facial injury |
| Systemic | High blood pressure (hypertension), blood thinners (aspirin, warfarin, heparin) |
| Bleeding disorders | Clotting factor deficiencies, hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease) |
| Tumors | Intranasal tumors (especially in adolescent boys - think juvenile nasopharyngeal angiofibroma) |
| Infections | Sinusitis, rhinitis, COVID-19 |
First Aid Management (Anterior Epistaxis)
- Sit upright, lean slightly forward (not backward - avoids swallowing blood)
- Pinch the soft lower part of the nose firmly for 10-15 minutes without releasing
- Breathe through the mouth
- Apply ice pack to the bridge of the nose
- Do NOT tilt the head back
When Is It Dangerous?
- Bleeding doesn't stop after 20-30 minutes
- Blood loss is heavy (patient feels faint, dizzy)
- Epistaxis follows significant head trauma
- Patient is on blood thinners
- Airway is compromised
Clinical Significance
- Uncontrolled hypertension - always check BP
- Leukemia or lymphoma (spontaneous bleeding)
- Vitamin K deficiency or anticoagulant overdose
- Liver disease (impaired clotting factor production)
- Hereditary hemorrhagic telangiectasia - a genetic vascular disorder causing recurrent bleeds
what is HERD immunity that attributes to vaccination
Herd Immunity and Vaccination - Full Explanation
What Is Herd Immunity?
"Herd immunity (or community immunity) describes a type of immunity that occurs when the vaccination of a portion of the population provides protection to unprotected individuals. The higher the number of immune individuals, the lower the likelihood that a susceptible person will come in contact with an infectious agent."
How Vaccination Creates Herd Immunity
WITHOUT herd immunity:
Infected person → spreads to susceptible person → spreads further → EPIDEMIC
WITH herd immunity (enough vaccinated):
Infected person → hits immune person (vaccinated) → CHAIN BROKEN → disease dies out
- Long-lived plasma cells producing pre-existing antibodies
- Memory B cells that rapidly produce antibodies on re-exposure
- Memory T cells (both CD4+ and CD8+) ready to respond immediately
The Herd Immunity Threshold (HIT)
"The proportion of immune individuals in a population, above which a disease may no longer persist, is the herd immunity threshold. Its value varies with the virulence of the disease, the efficacy of the vaccine and the contact parameter for the population."
HIT = 1 - (1/R₀)
| Disease | R₀ (infectiousness) | Herd Immunity Threshold |
|---|---|---|
| Measles | 12-18 | ~95% (very high - very contagious) |
| Polio | 5-7 | ~80-85% |
| Diphtheria | 6-7 | ~75-85% |
| Mumps | 4-7 | ~75-86% |
| COVID-19 | 2-6 | ~50-85% |
| Influenza | 2-3 | ~50-67% |
| Smallpox | 5-7 | ~80-85% |
What Contributes to Herd Immunity?
- Natural infection - people who recover from disease become immune
- Vaccination - artificial, controlled way to build immunity without suffering disease
- Herd structure - population composition (births, deaths, migration, age distribution)
Real-World Examples
| Disease | Result of Herd Immunity via Vaccination |
|---|---|
| Smallpox | Eradicated globally in 1980 |
| Polio | Eliminated from most countries |
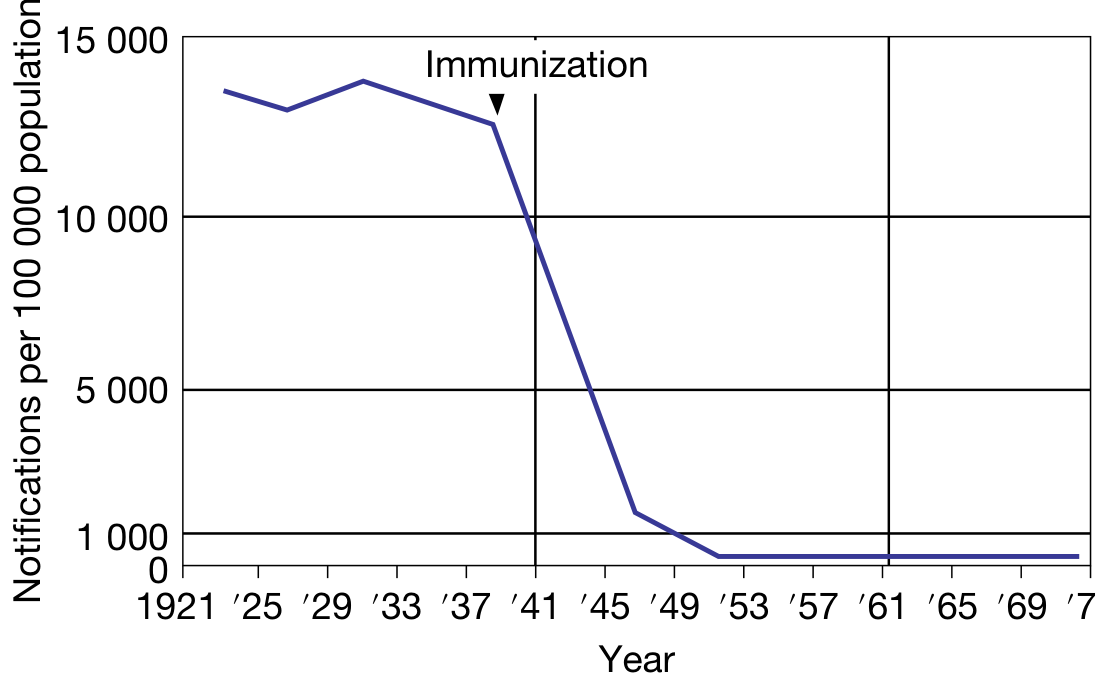
| Diphtheria | Dramatically reduced - diphtheria disappeared from communities where ~75% of children were immunized (Roitt's Immunology) |
| Measles | Controlled where >95% vaccinated; outbreaks occur in unvaccinated communities |
Who Does Herd Immunity Protect?
- Newborns (too young for many vaccines)
- Immunocompromised patients (cancer, HIV, organ transplant patients)
- Pregnant women (some vaccines contraindicated)
- People with severe allergies to vaccine components
- Elderly with waning immunity
Important Limitations
"Individuals protected by herd immunity remain susceptible to infection upon direct exposure. This can lead to outbreaks when a group of susceptible individuals accumulate - such as mumps outbreaks among university students."
- Tetanus - herd immunity does NOT protect individuals because it is not spread person-to-person (spores live in soil); every individual needs their own vaccination
- Herd immunity requires maintenance - if vaccination rates drop, susceptible populations build up and outbreaks occur (e.g., measles resurgence in anti-vaccine communities)
Key Takeaway
Vaccination does not just protect the individual - it protects the entire community by breaking chains of transmission. This is why vaccination is considered a public health responsibility, not just a personal choice.
45. Which of the following is NOT treated with antibiotics? A) tularemia B) anthrax C) plague D) ebola E) lyme disease correct answe and explain why
Answer: D. Ebola
The Core Reason: Bacteria vs. Virus
Antibiotics kill or inhibit BACTERIA. They have NO effect on VIRUSES.
- Options A, B, C, and E are all caused by bacteria → treated with antibiotics ✅
- Option D (Ebola) is caused by a virus → antibiotics are completely useless against it ✅
Each Disease Explained
✅ A. Tularemia - TREATED WITH ANTIBIOTICS
- Caused by: Francisella tularensis (bacterium)
- Transmitted by: tick/deer fly bites, handling infected animals (rabbits), inhalation
- Antibiotic treatment: Gentamicin or streptomycin (first choice); fluoroquinolones or doxycycline as alternatives
- From Fishman's Pulmonary Diseases: "Streptomycin was the first effective antibiotic for treating all forms of tularemia"
✅ B. Anthrax - TREATED WITH ANTIBIOTICS
- Caused by: Bacillus anthracis (spore-forming bacterium)
- Forms: cutaneous (skin), inhalation (most deadly), gastrointestinal
- Antibiotic treatment: Ciprofloxacin (drug of choice), doxycycline, penicillin, vancomycin
- From Goldman-Cecil Medicine: "The timely administration of antibiotics is essential for all forms of anthrax... current treatment of choice is a fluoroquinolone (e.g., ciprofloxacin)"
- Note: Treatment is for 60 days to eliminate any remaining spores
✅ C. Plague - TREATED WITH ANTIBIOTICS
- Caused by: Yersinia pestis (bacterium)
- Forms: bubonic (swollen lymph nodes/buboes), septicemic, pneumonic
- Antibiotic treatment: Streptomycin, gentamicin, doxycycline, or fluoroquinolones
- From Jawetz Medical Microbiology: "Treatment consists of supportive care and antibiotic treatment with streptomycin, gentamicin, doxycycline, or a fluoroquinolone antibiotic"
❌ D. Ebola - NOT TREATED WITH ANTIBIOTICS ← CORRECT ANSWER
- Caused by: Ebola virus (family Filoviridae) - a negative-sense RNA virus
- Transmission: Contact with blood/body fluids of infected people or animals; primarily in Africa
- Why no antibiotics? Antibiotics target bacterial structures (cell walls, ribosomes, DNA gyrase) that viruses simply do not have
- Actual treatment: Supportive care (IV fluids, electrolytes, oxygen) + two approved monoclonal antibody treatments:
- Atoltivimab/miftivimab/odesivimab (cocktail)
- Ansuvimab - binds to Ebola virus surface glycoprotein (GP1.2), blocking it from entering cells
- From Sherris Medical Microbiology: "Two monoclonal antibodies against Ebola surface GP for treatment"
✅ E. Lyme Disease - TREATED WITH ANTIBIOTICS
- Caused by: Borrelia burgdorferi (spirochete bacterium)
- Transmitted by: Ixodes tick bites
- Classic sign: Bull's-eye rash (erythema migrans)
- Antibiotic treatment: Doxycycline (first line), amoxicillin, cefuroxime; IV ceftriaxone for neurological/cardiac involvement
- From Harrison's: Lyme carditis "resolves within 1-2 weeks of antibiotic treatment"
Summary Table
| Disease | Causative Agent | Type | Antibiotic? | Treatment |
|---|---|---|---|---|
| Tularemia | F. tularensis | Bacterium | ✅ Yes | Gentamicin, streptomycin |
| Anthrax | B. anthracis | Bacterium | ✅ Yes | Ciprofloxacin, doxycycline |
| Plague | Y. pestis | Bacterium | ✅ Yes | Streptomycin, gentamicin |
| Ebola | Ebola virus | VIRUS | ❌ NO | Supportive + monoclonal antibodies |
| Lyme disease | B. burgdorferi | Bacterium | ✅ Yes | Doxycycline, amoxicillin |