Myocarditis vs infarction
Reading File
Finding Sources
Finding Sources
Searching PubMed
myocarditis versus myocardial infarction differentiation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive comparison. Here is the full structured response:
Myocarditis vs. Myocardial Infarction
1. Core Definition
| Myocarditis | Myocardial Infarction (MI) | |
|---|---|---|
| Essence | Inflammation of the myocardium - infectious, immune, or toxic | Ischemic necrosis of myocardium from arterial occlusion |
| Primary mechanism | Immune/inflammatory injury to myocytes | Oxygen supply-demand mismatch due to plaque rupture + thrombosis |
| Vessels | Normal coronary arteries (usually) | Atherosclerotic coronary artery occlusion |
2. Pathogenesis
Myocarditis
The most common cause in the US is viral infection - coxsackie B viruses and enteroviruses predominate historically; more recently parvovirus B19, HHV-6, SARS-CoV-2, and HIV are increasingly implicated. Injury occurs via two mechanisms:
- Direct viral cytotoxicity - viral proteins disrupt sarcolemmal integrity
- Immune-mediated injury - virus-specific T cells attack infected myocytes; molecular mimicry can trigger cross-reactive immune response against myosin heavy chain
Three disease stages have been proposed:
- Acute - cytotoxicity, focal necrosis
- Subacute - humoral autoimmune injury
- Chronic - diffuse fibrosis, dilated cardiomyopathy (DCM) in up to 16% of adults, 46% of children
Non-viral causes include Trypanosoma cruzi (Chagas disease - endemic in Latin America, ~300,000 infected in the US), Toxoplasma, Lyme disease (Borrelia - presents mainly as AV block), drug hypersensitivity, SLE, polymyositis, and post-mRNA COVID-19 vaccination (rare, mainly young males after the second dose, usually self-limited).
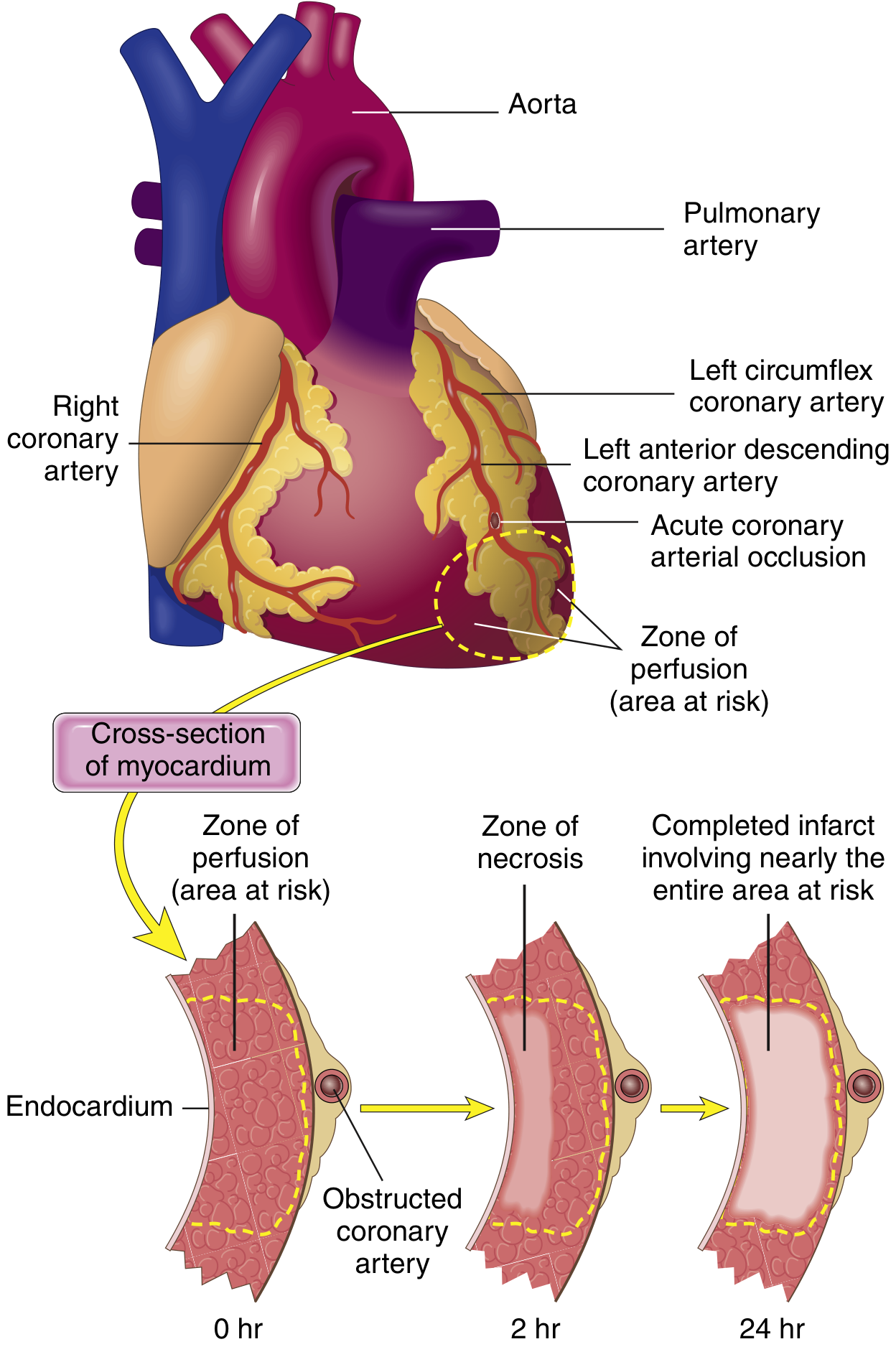
Myocardial Infarction
The vast majority are caused by acute coronary thrombosis overlying a disrupted or eroded atherosclerotic plaque. The sequence:
- Plaque erosion/rupture exposes subendothelial collagen and necrotic plaque contents
- Platelets adhere and release TXA2, ADP, serotonin - further aggregation and vasospasm
- Coagulation activation via tissue factor
- Complete luminal occlusion within minutes
In ~10% of MIs, occlusive atherosclerosis is absent - causes include coronary vasospasm, emboli from mural thrombi (e.g. AF), valve vegetations, small vessel vasculitis, amyloid deposition, or sickle cell disease. Within 4 hours, angiography shows thrombosis in ~90% of STEMI cases.
3. Who Gets It? (Epidemiology)
| Myocarditis | MI | |
|---|---|---|
| Age | Young (teens-40s); no strong age predilection | Risk rises progressively with age; 45% occur before age 65 |
| Sex | Males more common (especially post-vaccine myocarditis) | Men > women; gap narrows after menopause |
| Risk factors | Viral illness, autoimmune disease, immunosuppression, drug exposure | Atherosclerosis risk factors (HTN, DM, dyslipidemia, smoking, family history) |
| Prodrome | Flu-like symptoms (fever, myalgias, fatigue) 1-2 weeks prior | Usually none; or unstable angina prodrome |
4. Clinical Presentation
| Feature | Myocarditis | MI |
|---|---|---|
| Chest pain | Variable; pleuritic or positional component possible | Severe, crushing, pressure-like; radiates to arm/jaw |
| Fever | Common | Absent (mild inflammatory fever may occur 24-48h post-MI) |
| Dyspnea | Common (especially in children) | Present if significant LV dysfunction |
| Palpitations/arrhythmias | Prominent - PVCs, NSVT, AV block | Present - VF most feared early complication |
| Hemodynamic instability | Can be fulminant, especially in infants | Cardiogenic shock in large STEMI |
| Prodrome | Flu-like illness precedes by days-weeks | Typically absent or pre-existing angina |
Key clinical clue from Rosen's Emergency Medicine: "Patients with myocarditis are usually young and have few risk factors for coronary artery disease. In myocarditis, chest pain continues without evolving ischemic ECG changes."
5. ECG Findings
| Myocarditis | MI | |
|---|---|---|
| Pattern | Non-specific; sinus tachycardia, low voltages, prolonged QT, widened QRS | Evolving pattern: hyperacute T waves → ST elevation → Q waves → T inversion |
| ST changes | Diffuse or multifocal ST changes (not following one coronary territory) | ST changes in specific coronary territory (e.g. II/III/aVF for inferior MI) |
| AV block | Can occur (especially in Lyme, Chagas) | Can occur in inferior MI (RCA occlusion) |
| Key distinction | ECG abnormalities may extend beyond the distribution of a single coronary artery | Changes localized to one vascular territory |
| Q waves | Absent | Develop in STEMI (transmural necrosis) |
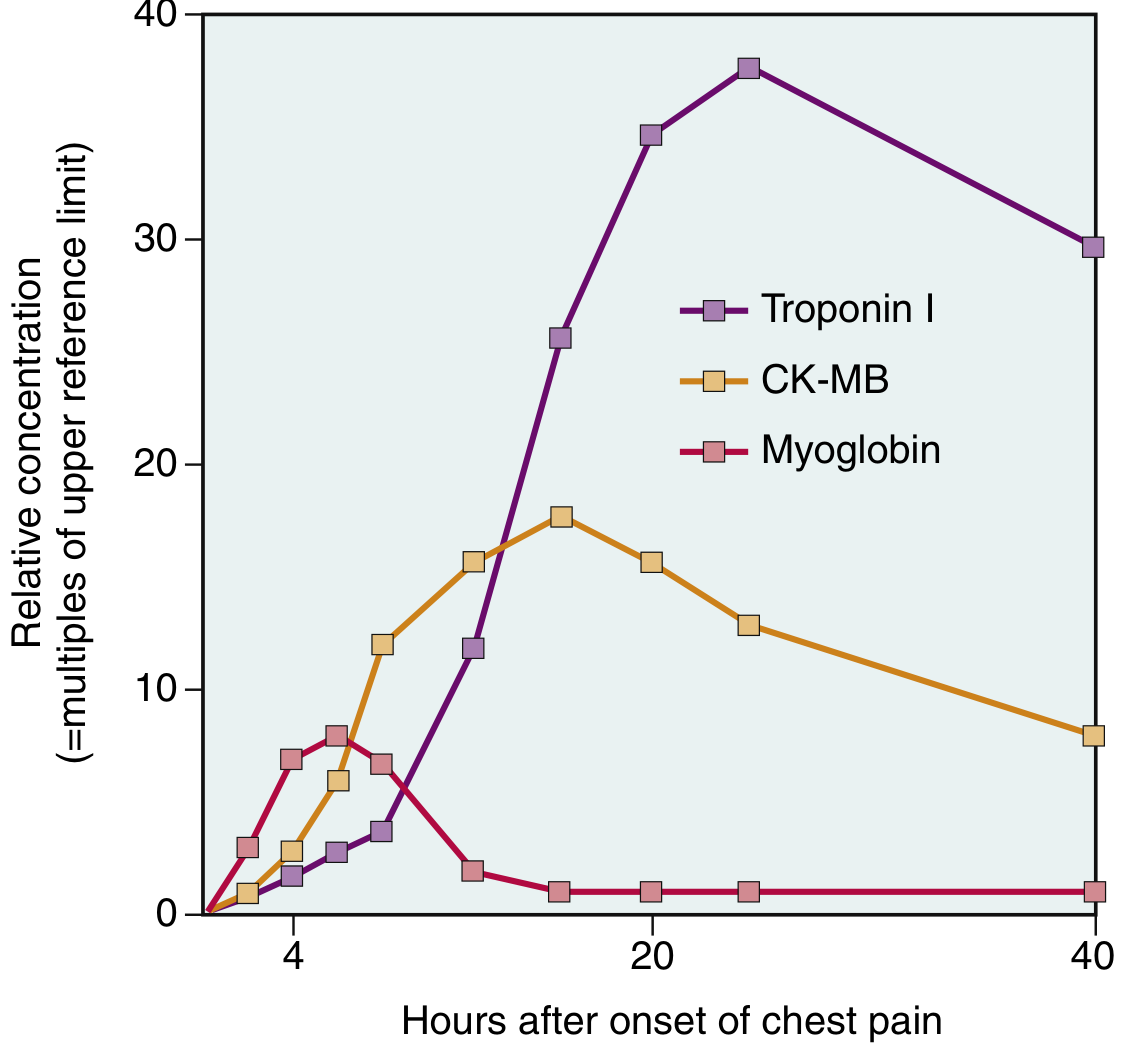
6. Biomarkers
Both conditions elevate troponin - this is a common pitfall.
| Myocarditis | MI | |
|---|---|---|
| Troponin | May be elevated (timing uncertain; negative serial troponin does NOT rule out) | Rises 2-4h, peaks 48h, remains elevated 7-10 days |
| CK-MB | May be elevated | Rises 2-4h, peaks 24-48h, normalizes ~72h |
| Pattern | Scattered, unpredictable | Predictable rise-and-fall kinetics |
| Inflammatory markers | ESR/CRP/WBC often elevated, but of no specific diagnostic value | Mild elevation post-MI (inflammatory response) |
7. Echocardiography
| Myocarditis | MI | |
|---|---|---|
| Wall motion | Global hypokinesis (diffuse, not matching a coronary territory) | Regional wall motion abnormality (territory-specific) |
| EF | Often reduced | Reduced in proportion to infarct size |
| Distinguishing feature | Wall motion abnormalities do NOT follow coronary artery anatomy | Wall motion abnormalities ARE in a coronary artery distribution |
| Pericardial effusion | Can be present (myopericarditis) | Rare (Dressler syndrome, days-weeks post-MI) |
8. Advanced Imaging: Cardiac MRI (CMR)
CMR is the most powerful non-invasive tool for differentiation:
| CMR Finding | Myocarditis | MI |
|---|---|---|
| Late gadolinium enhancement (LGE) pattern | Patchy, mid-wall or epicardial, non-coronary distribution; often septal | Subendocardial or transmural, following a coronary territory |
| T2 signal (edema) | Diffuse or patchy myocardial edema | Edema in area at risk (territory-specific) |
| Microvascular obstruction | Absent | Present in large STEMIs ("no-reflow") |
| Prognostic role | Septal/mid-wall LGE predicts SCD and VT risk | Infarct size predicts HF and mortality |
9. Coronary Angiography
- Myocarditis: Normal coronary arteries (key diagnostic finding when coronary disease is suspected)
- MI: Culprit lesion with plaque rupture and thrombus; angiography demonstrates thrombotic occlusion in ~90% of STEMIs within 4 hours
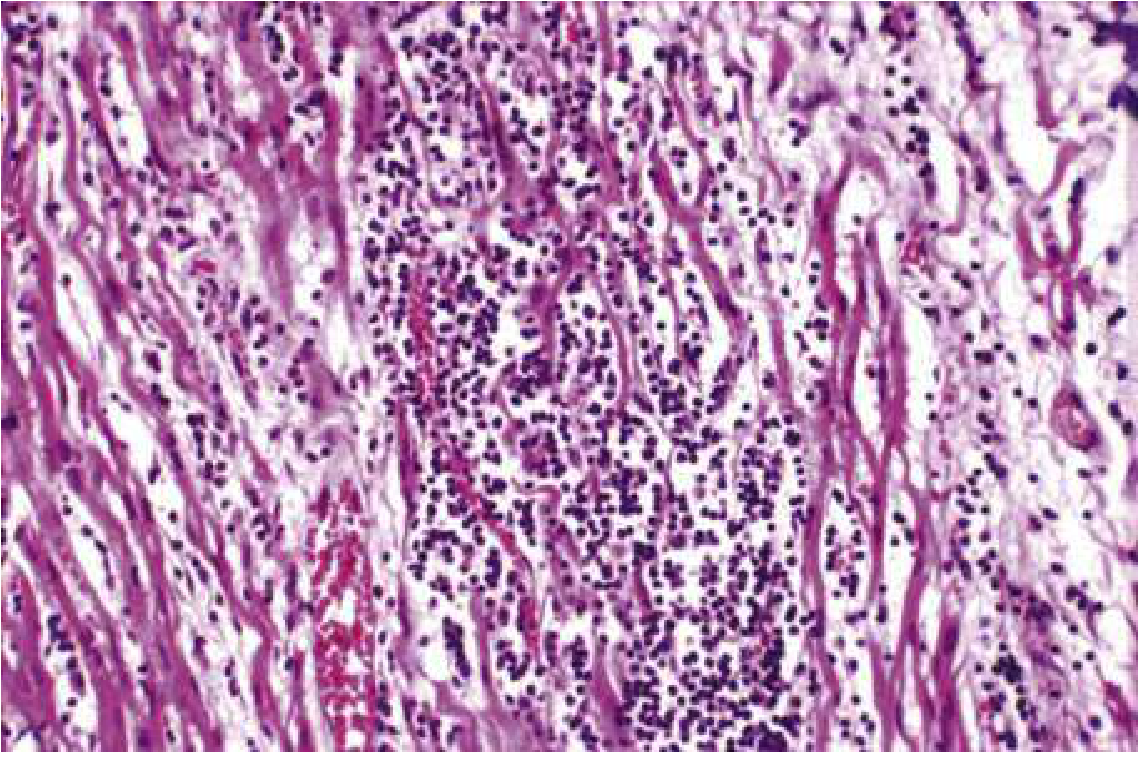
10. Histopathology
Myocarditis (Dallas Criteria)
Formal diagnosis requires endomyocardial biopsy showing:
- Interstitial mononuclear (lymphocytic) infiltrate
- Myocyte injury/necrosis adjacent to the infiltrate
- Edema and hemorrhage in active disease
- No ischemic pattern - not subendocardial-predominant
Myocardial Infarction
Follows a predictable temporal sequence of morphological changes:
| Time | Gross | Microscopy |
|---|---|---|
| 0-4h | None | Waviness of fibers at border |
| 4-12h | Occasional dark mottling | Coagulative necrosis, edema, hemorrhage begins |
| 12-24h | Dark mottling | Ongoing coagulation necrosis; pyknosis; early neutrophils |
| 1-3 days | Mottling with yellow center | Neutrophilic infiltrate; loss of nuclei and striations |
| 3-7 days | Hyperemic border, yellow-tan center | Dead myofibers; macrophage infiltration begins |
| 7-10 days | Maximally yellow-tan, soft | Granulation tissue at margins |
| Weeks | White scar forming | Progressive fibrosis |
Key: coagulative necrosis (not liquefactive), subendocardial predilection, neutrophil-then-macrophage-then-fibrosis sequence. Myocardial necrosis proceeds to scar without significant regeneration.
11. Complications
| Myocarditis | MI | |
|---|---|---|
| Acute | Arrhythmias, AV block, fulminant heart failure, cardiogenic shock, SCD | VF/VT (80-90% of cardiac deaths in acute phase), pump failure, mechanical complications (free wall rupture, papillary muscle rupture, VSD) |
| Chronic | Dilated cardiomyopathy (16% adults, 46% children), persistent VT circuits from scar, SCD | LV aneurysm, Dressler syndrome, chronic HF, recurrent ischemia |
| SCD in young | Myocarditis is among the top causes of SCD in patients <21 years | CAD is top cause in patients >30 years |
12. Management
| Myocarditis | MI | |
|---|---|---|
| Specific therapy | Supportive; treat underlying cause (antivirals if applicable, immunosuppression in autoimmune forms) | Urgent reperfusion - thrombolysis or PCI (STEMI); antithrombotic therapy |
| HF management | ACEi, diuretics, beta-blockers | ACEi, beta-blockers, aldosterone antagonists, diuretics |
| Activity | Restrict exercise (risk of SCD during myocarditis) | Graduated cardiac rehabilitation |
| Arrhythmia | Beta-blockers, amiodarone; consider ICD after recovery if EF remains low | ICD if EF <35% at 40 days post-MI |
| Transplant | In refractory fulminant myocarditis | In end-stage ischemic cardiomyopathy |
13. Quick Differentiation Summary
| Clue | Points to Myocarditis | Points to MI |
|---|---|---|
| Age | Young (teens-40s) | Older; cardiovascular risk factors |
| Prodrome | Flu-like illness | None (or angina) |
| Chest pain character | Pleuritic, variable | Crushing, pressure, radiating |
| ECG ST changes | Multi-territory, non-focal | Single coronary territory |
| Echo wall motion | Global, non-territorial | Regional, territorial |
| CMR LGE | Mid-wall/epicardial, patchy | Subendocardial/transmural |
| Coronary angiography | Normal | Culprit lesion/thrombus |
| Biopsy | Lymphocytic infiltrate + myocyte necrosis | Coagulative necrosis, no inflammation initially |
Sources:
- Robbins & Kumar Basic Pathology, Myocardial Infarction (p. 353-359) and Myocarditis (p. 375-376)
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Myocarditis (p. 1119-1120)
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, Myocarditis and Arrhythmias
- Goldman-Cecil Medicine, Myocarditis and Myocardial Infarction chapters
This is a shared conversation. Sign in to Orris to start your own chat.