Dysthyroid ophthalmology
Reading File
Finding Sources
Searching PubMed
thyroid eye disease Graves ophthalmopathy
!
HTTP 500 for https://eutils.ncbi.nlm.nih.gov/entrez/eutils/esummary.fcgi?tool=orrisai&email=dev%40orris.ai&api_key=***&db=pubmed&id=39664569%2C38215463%2C39952471&retmode=json
We encountered an error while processing your request. Please try again or reach out to us for help.
Dysthyroid ophthalmology
Reading File
Finding Sources
Searching PubMed
thyroid eye disease Graves ophthalmopathy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have rich, comprehensive content now. Let me compile the full answer.
Dysthyroid Ophthalmopathy (Thyroid Eye Disease)
Synonyms: Thyroid-associated orbitopathy (TAO), Graves' ophthalmopathy (GO), thyroid-related orbitopathy
Thyroid eye disease (TED) is the most common cause of both unilateral and bilateral proptosis in adults. It is an organ-specific autoimmune disorder most often associated with Graves' disease, though it can occur in euthyroid (~5-10%) and hypothyroid (~5-10%) patients.
Epidemiology & Risk Factors
- Women are 5x more likely to be affected, primarily reflecting the higher incidence of Graves' disease in women
- Peak onset: 4th-5th decade
- Smoking is the major modifiable risk factor - risk scales with cigarettes per day; cessation reduces risk
- Radioactive iodine (RAI) therapy for hyperthyroidism can worsen TED
- Association with other autoimmune disorders (myasthenia gravis co-occurs in a minority)
Pathogenesis
Anti-thyrotropin-receptor antibodies (TRAb) react against both thyroid gland cells and orbital fibroblasts. Both the insulin-like growth factor-1 receptor (IGF-1R) and the thyroid-stimulating hormone receptor (TSHR) are upregulated in orbital and brow fat.
This triggers:
- Inflammatory infiltration of extraocular muscles, interstitial tissues, orbital fat, and lacrimal glands (pleomorphic cellular infiltrate)
- Increased glycosaminoglycan secretion → osmotic water imbibition → orbital volume expansion (muscles can swell up to 8x normal)
- Lipogenesis by fibroblasts/preadipocytes → orbital fat enlargement
- Secondary elevation of intraorbital pressure and optic nerve compression
- Eventual muscle fibre degeneration → fibrosis → restrictive myopathy and diplopia
(Kanski's Clinical Ophthalmology 10th ed.)
Disease Course
TED proceeds through two stages:
- Congestive (active/inflammatory) phase: red, painful eyes; typically lasts 1-3 years
- Fibrotic (quiescent/inactive) phase: white eyes, painless; residual motility defects may persist
Only ~10% of patients develop serious long-term ocular problems.
Clinical Features

Thyroid-related orbitopathy with bilateral upper eyelid retraction and proptosis (Wills Eye Manual)
Features are classified into 5 categories:
1. Soft Tissue Involvement
- Periorbital and eyelid edema, conjunctival injection and chemosis
- Epibulbar hyperaemia over horizontal rectus muscle insertions
- Superior limbic keratoconjunctivitis (SLK)
- Tearing, photophobia, orbital discomfort
- Reduced blink rate
2. Lid Signs (highly characteristic)
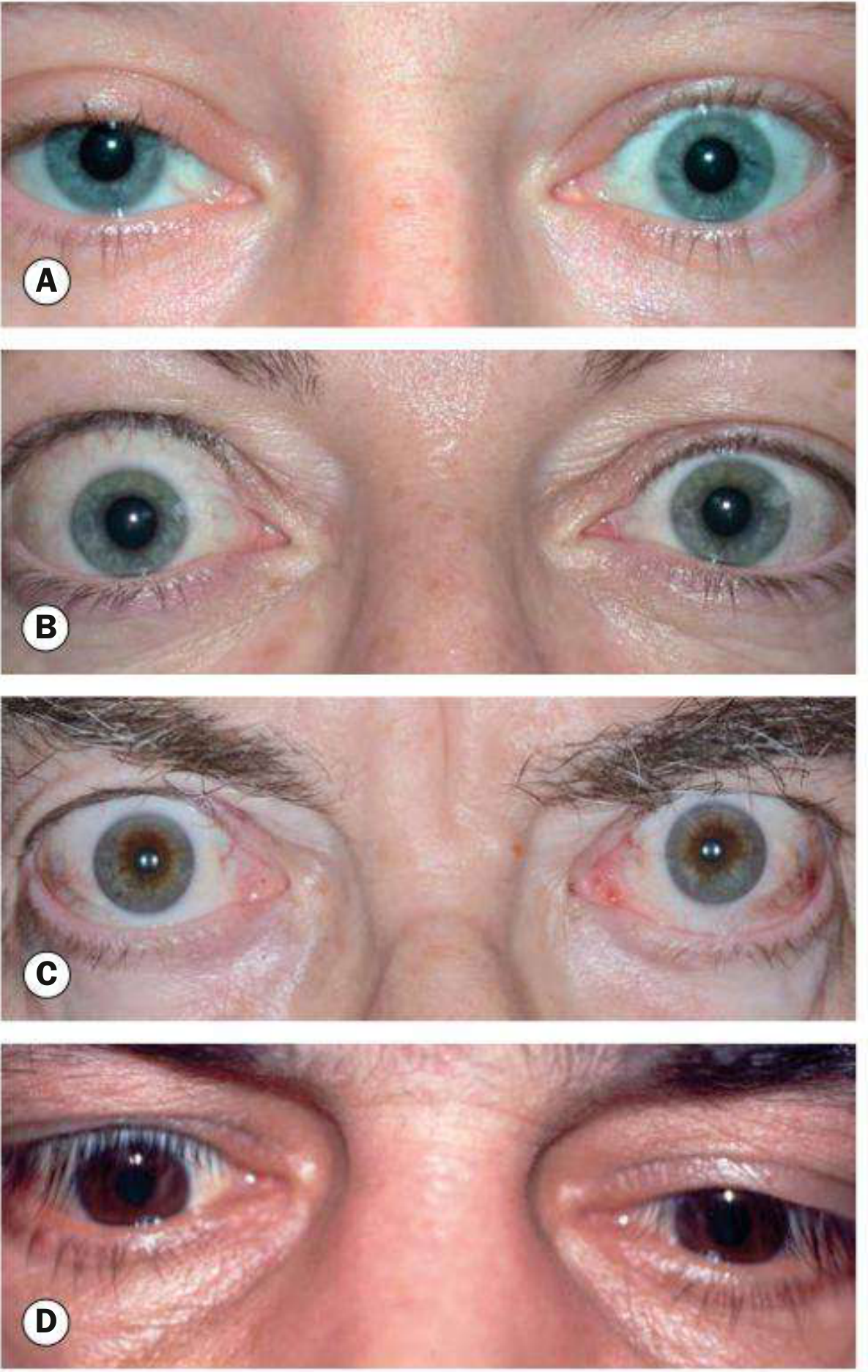
Lid signs in TED. (A) Mild unilateral lid retraction; (B) Dalrymple sign - bilateral asymmetric retraction; (C) Kocher sign - bilateral severe retraction with staring appearance; (D) von Graefe sign - lid lag on downgaze (Kanski's)
| Sign | Description |
|---|---|
| Dalrymple sign | Lid retraction in primary gaze - widened palpebral fissure |
| Kocher sign | Staring/frightened expression on attentive fixation |
| von Graefe sign | Retarded descent of upper lid on downgaze (lid lag) |
| Lateral flare | Lateral flaring of upper eyelid - highly specific for TED |
Upper lid margin at or above superior limbus = scleral show = lid retraction. Lower lid retraction (inferior scleral show) is less specific.
3. Proptosis (Exophthalmos)
- Axial, unilateral or bilateral, often asymmetric; measured with Hertel exophthalmometer
- Severe proptosis + lid retraction + tear dysfunction → exposure keratopathy, corneal ulceration
4. Restrictive Myopathy
- Affects 30-50% of TED patients; may be permanent
- Muscles involved in order of frequency: inferior rectus > medial rectus > superior rectus > lateral rectus (mnemonic: "I'M SaLt")
- Elevation defect (IR fibrosis) is the most common motility deficit - may mimic SR palsy
- Adduction deficit may mimic VI nerve palsy
- Positive forced duction testing confirms restriction (distinguishes from true palsy)
5. Compressive Optic Neuropathy (CON)
- Occurs in 5-7% of TED patients
- Caused by EOM thickening at the orbital apex compressing the optic nerve (NOT usually from severe proptosis)
- Proptosis is often absent or mild in CON
- Must be excluded at every visit in every patient
- Signs: RAPD, dyschromatopsia, visual field loss, reduced VA, optic disc swelling or pallor
Key point: CON almost invariably occurs with restrictive strabismus and increased resistance to retropulsion. Always check IOP in upgaze (elevation correlates with inferior rectus enlargement severity).
Other Signs
- Elevated IOP (especially in upgaze)
- Superficial punctate keratopathy / corneal ulceration (exposure)
- Rarely choroidal folds
EUGOGO Classification (2021 - Kanski)
Activity - Clinical Activity Score (CAS)
One point each for:
- Spontaneous retrobulbar pain
- Pain on attempted up or downward gaze
- Redness of eyelids
- Redness of conjunctiva
- Swelling of conjunctiva or plica
- Swelling of eyelids
- Swollen caruncle
CAS ≥ 3/7 = active disease (immunosuppressive treatment indicated)
At follow-up, additional points for: proptosis increase ≥2 mm; uniocular excursion decrease ≥8°; Snellen acuity decrease ≥1 line (total out of 10).
Severity
- Mild: Minor soft tissue signs, mild proptosis (<3 mm above normal), transient/no diplopia, corneal exposure responding to lubricants; no optic nerve involvement
- Moderate-severe: More significant soft tissue involvement, proptosis ≥3 mm above normal, inconstant/constant diplopia, incomplete lid closure
- Sight-threatening (very severe): Dysthyroid optic neuropathy and/or corneal breakdown
Systemic Associations
- Hyperthyroidism in ≥80%; hypothyroid or euthyroid in 5-10% each
- TED does NOT necessarily follow thyroid status - it may precede or follow thyroid dysfunction by months to years
- Check TFTs (TSH, T3, T4), TSI (thyroid-stimulating immunoglobulin), TPO antibodies
- Elevated TSI helps confirm TED in atypical cases and can guide treatment intensity
Workup
- History: Duration, pain, vision change, thyroid history, smoking, cancer history
- Complete ocular exam:
- Slit-lamp with fluorescein (exposure keratopathy)
- RAPD, dyschromatopsia, visual fields, OCT (optic nerve compression)
- Extraocular motility - versions and ductions
- Prism/Maddox rod for diplopia measurement
- Hertel exophthalmometer for proptosis
- Resistance to retropulsion
- IOP in primary and upgaze
- Dilated fundus exam
- Imaging: CT or MRI orbits - shows spindle-shaped EOM enlargement sparing the tendons (distinguishes from orbital myositis, which involves tendons); thickening at orbital apex
- Bloods: TFTs (T3, T4, TSH), TSI, anti-TPO; vitamin D level; myasthenia workup if indicated
Treatment
All Patients
- Smoking cessation - explicitly documented
- Endocrinology referral for thyroid management
- Euthyroid TED: TFTs every 6-12 months (many will develop thyroid dysfunction within 2 years)
Mild Disease
- Topical lubricants (artificial tears, lubricating ointment)
- Eyelid taping at night, swim goggles
- Head elevation to reduce periorbital edema
- Sunglasses, prisms for mild photophobia/strabismus
- Selenium supplementation 100 µg PO twice daily for 6 months - reduces severity/progression in mild-moderate active disease (evidence from European RCTs; benefit unclear where selenium deficiency is absent)
- Botulinum toxin injection for isolated lid retraction
Moderate-Severe Active Disease (CAS ≥3)
IV corticosteroids are first-line and superior to oral:
- Methylprednisolone 500 mg IV weekly × 6 weeks, then 250 mg IV weekly × 6 weeks (total ≤8 g to reduce hepatic risk)
- Oral prednisolone 60-100 mg/day is an alternative; response in 33-63%
- Combination of IV steroids + mycophenolate sodium (0.72 g/day × 24 weeks) is superior to IV steroid monotherapy and is the regimen of choice in specialized centres
- Contraindications to IV steroids: significant hepatic dysfunction, cardiovascular disease, uncontrolled hypertension/diabetes
Other immunosuppressives:
- Azathioprine (effective combined with RT or steroids, not alone)
- Methotrexate (monotherapy for steroid-resistant or steroid-dependent cases)
- Mycophenolate mofetil (MMF) - inhibits lymphocyte proliferation; less disease reactivation
Orbital radiotherapy:
- Low-dose fractionated RT: 20 Gy in 10-14 fractions over 2 weeks
- Most beneficial for improving ocular motility in active TED
- ~60% response rate; positive response within 6 weeks, maximum by 4 months
- Contraindicated in diabetics (retinopathy risk), used cautiously in vasculopaths
- Mechanism: non-specific anti-inflammatory effect on orbital lymphocyte infiltrate; inhibits fibroblast proliferation and glycosaminoglycan secretion
Sight-Threatening Disease (Optic Neuropathy)
- Pulsed high-dose IV methylprednisolone: 0.5-1 g on 3 successive days or on alternate days 3-6 times; maximum cumulative dose <8 g; then taper to oral
- If steroids fail or contraindicated → urgent orbital decompression
- Monitor LFTs; start gastric protection and osteoporosis prophylaxis
Biologics (Newer Therapies)
- Teprotumumab (IGF-1R monoclonal antibody) - FDA-approved; reduces proptosis, diplopia, and CAS in active moderate-severe TED. A 2025 systematic review/meta-analysis confirmed efficacy and safety (PMID: 39952471)
- Tocilizumab (anti-IL-6R) - systematic review 2024 supports efficacy/safety (PMID: 38215463)
- Rituximab, adalimumab - promising in small trials; mixed results in larger studies
Surgical Management
Surgery is performed only in the inactive/quiescent phase (except vision-threatening emergencies). The sequence must be followed:
Step 1: Orbital Decompression
Indications: Optic neuropathy, severe/worsening exposure keratopathy, globe luxation, uncontrollably elevated IOP, morbid proptosis
- Walls removed: floor, medial wall, lateral wall, roof (various combinations per Naffziger classification)
- Endoscopic and transconjunctival approaches are common
- Complication: new or worsened diplopia (common); globe malposition
Step 2: Strabismus Surgery
- Only after orbital decompression is complete and stable
- Adjustable sutures preferred due to restrictive nature
- Aim: eliminate diplopia in primary and reading position
Step 3: Eyelid Surgery
- Lid lengthening procedures (recession of retractors) for lid retraction
- Blepharoplasty for fat prolapse
- Done last to achieve optimal functional and cosmetic result
Altering this surgical sequence leads to unpredictable outcomes.
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Orbital myositis | Acute pain, tendons involved on imaging, steroid response rapid |
| Cavernous sinus thrombosis | Fever, sepsis, VI nerve palsy, ophthalmoplegia |
| Orbital pseudotumor (IOID) | Painful, may involve any orbital structure, tendons involved |
| Myasthenia gravis | Fatigable ptosis (not retraction), variable diplopia, no proptosis, normal imaging |
| Metastatic orbital disease | History of primary cancer, irregular muscle borders |
Recent Evidence (2024-2025)
- Teprotumumab: A 2025 systematic review and meta-analysis (PMID: 39952471) confirmed significant reductions in proptosis, CAS, and diplopia with a favorable safety profile
- Tocilizumab: A 2024 systematic review (PMID: 38215463) in Ophthalmic Plastic & Reconstructive Surgery found efficacy and acceptable safety as a steroid-sparing agent
- Biomarkers: A 2024 multi-omics systematic review (PMID: 39664569) identified novel candidate biomarkers for TED activity and severity that may guide individualized treatment in future
Sources: Kanski's Clinical Ophthalmology 10th ed. | Wills Eye Manual | Cummings Otolaryngology | Localization in Clinical Neurology 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.