Give me evaluation and management of DIC from Harrison
Reading File
Finding Sources
Searching PubMed
"disseminated intravascular coagulation" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the complete evaluation and management of DIC from Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 121.
Disseminated Intravascular Coagulation (DIC)
Definition
The ISTH (2001) defines DIC as "an acquired syndrome characterized by the intravascular activation of coagulation with loss of localization arising from different causes that can originate from and cause damage to the microvasculature, which if sufficiently severe, can produce organ dysfunction."
Common Causes (Table 121-2)
| Category | Examples |
|---|---|
| Sepsis | Bacterial (Staphylococci, streptococci, pneumococci, meningococci, gram-negative bacilli), viral, mycotic, parasitic, rickettsial |
| Trauma & Tissue Injury | Brain injury (gunshot), extensive burns, fat embolism, rhabdomyolysis |
| Obstetric Complications | Abruptio placentae, amniotic fluid embolism, eclampsia, retained dead fetus, septic abortion |
| Malignancy | Mucin-producing adenocarcinomas, acute promyelocytic leukemia (APL) |
| Vascular Disorders | Giant hemangiomas (Kasabach-Merritt syndrome), large vessel aneurysms (e.g., aorta) |
| Immunologic Disorders | Acute hemolytic transfusion reaction, organ/tissue transplant rejection, immunotherapy, graft-versus-host disease |
| Drugs | Fibrinolytic agents, aprotinin, warfarin (especially in neonates with protein C deficiency), prothrombin complex concentrates, recreational drugs (amphetamines) |
| Liver Disease | Acute hepatic failure |
| Envenomation | Snake, insects |
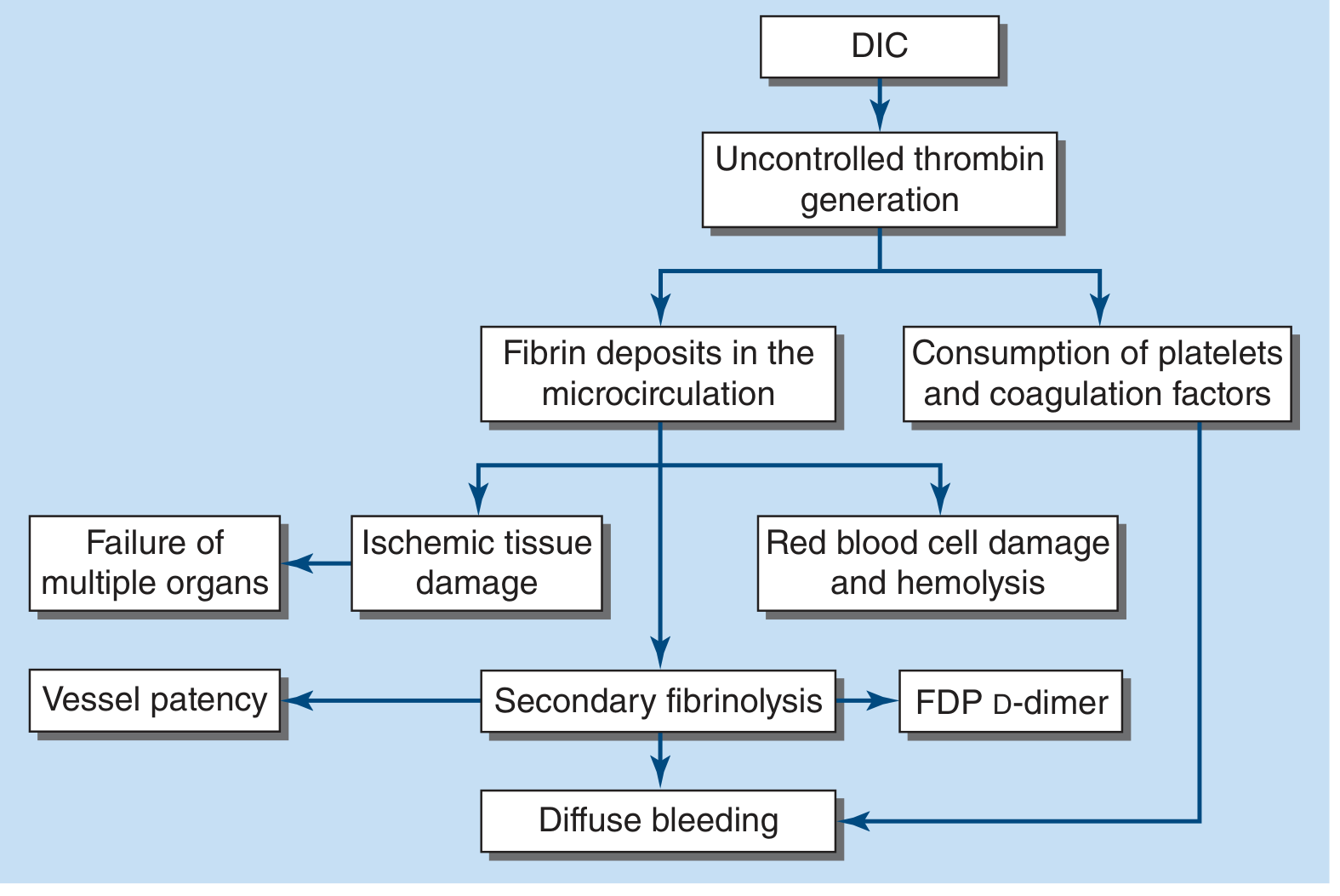
Pathophysiology
The central mechanism is uncontrolled thrombin generation via multiple pathways. Simultaneous disruption of physiologic anticoagulant mechanisms and abnormal fibrinolysis further accelerate this process. Key pathways include:
- Increased tissue factor expression (via inflammatory cytokines, neutrophil extracellular traps, polyphosphates)
- Damage to vascular endothelium (loss of antithrombotic properties)
- SIRS / cytokine storm - exuberant inflammatory response associated with increased mortality
Figure 121-4 - Pathophysiology of DIC:
Clinical Features
- Bleeding (most common): petechiae, ecchymoses, oozing from venipuncture sites, severe hemorrhage from GI tract, lungs, or CNS
- Thrombosis: microvascular occlusion causing organ failure; thrombosis of large vessels and cerebral embolism can also occur
- Shock: hemodynamic compromise is common in acute DIC
- Purpura fulminans: severe DIC with extensive skin thrombosis - predominantly in young children post-viral/bacterial infection (especially with protein C pathway deficiencies)
- Chronic DIC: discrete, restricted bleeding to skin or mucosal surfaces
- Mortality: 30 to >80% in acute DIC
Evaluation / Diagnosis
ISTH Scoring Tool for Overt DIC (Table 121-3)
| Parameter | Value | Points |
|---|---|---|
| Platelets | >100,000 × 10⁹/L | 0 |
| 50-100 × 10⁹/L | 1 | |
| <50 × 10⁹/L | 2 | |
| D-Dimer | Normal | 0 |
| Moderate increase | 2 | |
| Severe increase | 3 | |
| PT prolonged | <3 sec | 0 |
| 3-6 sec | 1 | |
| >6 sec | 2 | |
| Fibrinogen | >1 g/L | 0 |
| <1 g/L | 1 | |
| Total Score | <5 = Low-grade/nonovert DIC (repeat every 1-2 days) | |
| ≥5 = Overt DIC (repeat labs daily) |
Note: This scoring tool is not to be used in pregnant patients.
Laboratory Findings
Acute DIC:
- Thrombocytopenia
- Prolonged PT and aPTT
- Low fibrinogen (<100 mg/dL)
- Elevated D-dimer / fibrin degradation products (FDPs)
- Red cell fragmentation (microangiopathic hemolytic anemia) on blood smear
Chronic DIC:
- Elevated D-dimer / FDP
- PT, aPTT, fibrinogen may be within normal range or high
- Mild thrombocytopenia or normal platelet count
- Lower degree of red cell fragmentation than acute DIC
Differential Diagnosis
- Severe liver disease: Also has thrombocytopenia, reduced clotting factor synthesis, elevated D-dimer - but unlike DIC, lab parameters do not change rapidly; serial measurements help distinguish
- Microangiopathic disorders (TTP): Acute thrombocytopenia, red cell fragmentation, multiorgan failure - but presence of an inhibitor to ADAMTS13 assists diagnosis
Management
"The morbidity and mortality associated with DIC are primarily related to the underlying disease. Management of the underlying disease is required to control and eliminate DIC; however, support with platelets and coagulation factors may be needed until the inciting cause is under control."
1. Treat the Underlying Cause
This is the cornerstone of DIC management. Many patients require ICU-level care for shock and multiorgan manifestations.
2. Management of Hemorrhagic Symptoms
- Transfusion support is indicated for active bleeding or high risk of bleeding (e.g., before invasive procedures or after chemotherapy)
- Transfusion solely to correct mildly-moderately abnormal coagulation parameters is NOT indicated
| Product | Indication / Target |
|---|---|
| Platelets | Transfuse for count <10,000-20,000/μL |
| FFP | Source of coagulation factors when PT is prolonged >3 sec above ULN |
| Cryoprecipitate or fibrinogen concentrate | Maintain fibrinogen >150 mg/dL |
| Vitamin K | Should be given to all patients with DIC |
Patients must be frequently monitored and transfusion support adjusted as clinical status changes.
3. Replacement of Coagulation/Fibrinolysis Inhibitors
| Agent | Role / Indication |
|---|---|
| Low-dose continuous-infusion heparin (5-10 U/kg per hour) | May be effective in low-grade DIC associated with solid tumors, APL, or recognized thrombosis. Also indicated for purpura fulminans. In acute hemorrhagic DIC, heparin likely aggravates bleeding. Despite improved coagulation parameters in severe DIC, no survival benefit is proven; professional society recommendations vary widely. |
| Antithrombin concentrates | Demonstrated little efficacy in all sepsis patients; post-hoc analysis in sepsis + confirmed DIC suggests survival advantage - requires further study |
| Thrombomodulin concentrates | Same as antithrombin - post-hoc benefit in sepsis/DIC subgroup, not yet established |
| Activated Protein C (drotrecogin alfa) | Withdrawn from market after failing to show benefit in septic shock |
4. Management of Primary Hyperfibrinolytic State
- In DIC with a primary hyperfibrinolytic state and severe bleeding, antifibrinolytics (e.g., tranexamic acid) may be considered
- Due to thrombosis risk, concomitant use of heparin is considered
- Patients most likely to benefit: acute promyelocytic leukemia or chronic DIC with giant hemangiomas
Summary of Key Management Principles
- Treat the underlying cause - no definitive treatment otherwise
- Transfuse only for active bleeding or high procedural risk - not to normalize labs alone
- Maintain fibrinogen >150 mg/dL with cryoprecipitate or fibrinogen concentrate
- Heparin - reserved for low-grade DIC, APL, purpura fulminans; avoid in acute hemorrhagic DIC
- Monitor daily with platelet count, PT, aPTT, fibrinogen, D-dimer; adjust support accordingly
- ICU care for hemodynamic stabilization in acute severe DIC
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 121
Recent evidence note: A 2025 ISTH systematic review and meta-analysis (PMID: 40383152) confirmed that DIC mortality remains high and varies by etiology, broadly consistent with Harrison's figures. Japan's 2024 clinical practice guidelines for DIC in hematologic malignancy (PMID: 39674834) offer additional disease-specific management guidance for APL and related conditions.
This is a shared conversation. Sign in to Orris to start your own chat.