Neurocysticercosis
Reading File
Finding Sources
Searching PubMed
neurocysticercosis
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full response.
Neurocysticercosis (NCC)
Definition and Epidemiology
Neurocysticercosis is CNS infection by the larval stage (cysticercus) of the pork tapeworm Taenia solium. It is the most common parasitic disease of the human CNS and the leading cause of symptomatic/provoked epilepsy worldwide.
- Endemic in Latin America, Sub-Saharan Africa, India, China, and Southeast Asia
- Estimated 0.45-1.35 million epilepsy cases due to NCC in Latin America; ~1 million in India; 0.31-4.6 million in Africa
- In the US: 1,320-5,050 new cases/year, driven by immigration from endemic regions
- Also occurs in non-endemic countries through immigration of tapeworm carriers
- Bradley and Daroff's Neurology in Clinical Practice, p. 980
Life Cycle and Pathogenesis
Humans act as either the definitive host (adult tapeworm in intestine = taeniasis) or the intermediate host (larval cysts in tissues = cysticercosis).
Two routes of human infection:
- Taeniasis - ingestion of undercooked, contaminated pork containing cysticerci → adult tapeworm in intestine
- Cysticercosis - ingestion of T. solium eggs (fecal-oral route from a tapeworm carrier, including auto-infection) → oncospheres released, penetrate intestinal wall, disseminate via bloodstream to tissues including brain
The tapeworm scolex attaches to the intestinal mucosa via sucking disks and an armed rostellum. Each mature proglottid produces ~50,000 eggs. Eggs are immediately infective. In the CNS, cysts lodge preferentially at the grey-white matter interface.
Key point: You do NOT need to eat pork to get NCC - you only need to ingest eggs from a carrier.
- Harrison's Principles of Internal Medicine 22E, p. 1878
Classification by Location
| Form | Features |
|---|---|
| Parenchymal (most common) | Brain parenchyma; seizures predominate; at grey-white interface |
| Intraventricular | 4th > 3rd > lateral ventricles; risk of acute obstructive hydrocephalus and sudden death |
| Subarachnoid / Leptomeningeal | Basal cisterns, Sylvian fissures, CP angle; arachnoiditis, vasculitis, hydrocephalus |
| Racemose | Multilobulated cysts without scolex in subarachnoid space; "bunch of grapes" appearance |
| Spinal | Intra- or extramedullary; rare |
| Ocular | Vitreous, subretinal space |
- Grainger & Allison's Diagnostic Radiology, p. 1482
Stages of Parenchymal NCC (Radiological)
| Stage | Pathology | Imaging Findings |
|---|---|---|
| 1. Vesicular | Viable larva with scolex | Thin-walled cyst, CSF-isointense fluid, no/minimal enhancement, no edema; scolex hyperintense on T1/FLAIR/DWI - "hole with a dot" sign |
| 2. Colloidal vesicular | Larva degenerating; host immune response triggered | Ring-enhancing lesion, perilesional edema, mass effect; cyst fluid more proteinaceous (T1/FLAIR hyperintense) |
| 3. Granular nodular | Larva dead; cyst collapsing | Thick enhancing cyst walls, progressive edema, cyst shrinking |
| 4. Calcified nodular | Inactive/burnt-out | 2-10 mm calcifications, no edema/enhancement (may recur peri-seizure) |
Only vesicular and colloidal vesicular stages are treated with antiparasitic drugs. Calcified lesions have no role for antiparasitics.
- Grainger & Allison's Diagnostic Radiology, p. 1483
Neuroimaging
Multiple MRI and CT sequences showing different stages of NCC (vesicular cysts with scolex, intraventricular, and calcified lesions):
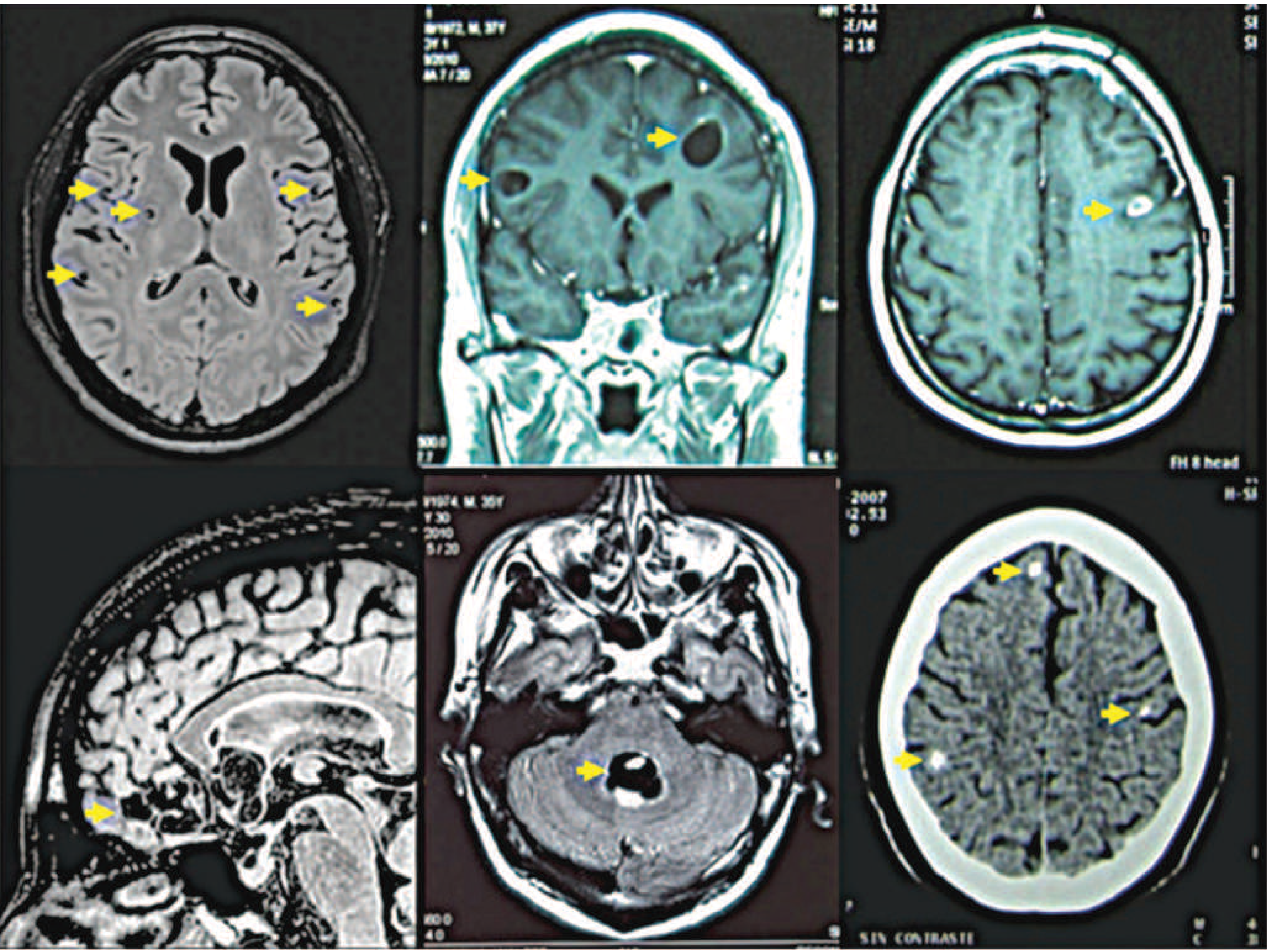
CT findings:
- 1-2 cm cystic lesion with thin walls and 1-3 mm mural nodule (scolex)
- Ring-enhancing lesion with perilesional edema
- Calcified foci (burnt-out cysts)
- Hydrocephalus
MRI advantages:
- Superior detection of the scolex (pathognomonic)
- Better visualization of intraventricular, subarachnoid, and brainstem lesions
- FLAIR sequences highlight cyst fluid and scolex
- Tintinalli's Emergency Medicine, p. 1198; Grainger & Allison's Diagnostic Radiology
Clinical Manifestations
Parenchymal NCC:
- Seizures - most common presentation (focal or generalized); typically occur as the parasite degenerates
- Headache
- Focal neurological deficits
- 80-90% of enhancing lesions resolve within 3-6 months; ~20% of patients continue to have seizures
Extraparenchymal NCC:
- Obstructive hydrocephalus (intraventricular)
- Elevated ICP, sudden death (4th ventricle cysts that float and obstruct = "ball-valve" effect)
- Chronic meningitis, vasculitis, brain infarcts (subarachnoid/leptomeningeal)
- Diplopia, cranial nerve palsies
CSF findings (when analyzed):
- Pleocytosis (lymphocytes, neutrophils, or eosinophils)
- Elevated protein
- Usually normal glucose (can be markedly reduced)
Recent evidence (2026): A systematic review (PMID 42087630) specifically characterizes NCC-associated meningitis as a significant complication requiring recognition. Movement disorders are an underappreciated manifestation (PMID 40822429).
Diagnosis
Del Brutto Revised Criteria (2017)
Absolute criteria (any one = definitive diagnosis):
- Histologic demonstration of cysticercus in biopsy specimen
- Cystic lesion with scolex on CT/MRI
- Direct visualization of subretinal parasite
Major neuroimaging criteria:
- Cystic lesion without scolex
- Ring-enhancing lesion (1-2 cm)
- Multilobulated cystic lesion in subarachnoid space
- CT hyperdense or calcified parenchymal lesion
Minor neuroimaging criteria:
- Obstructive hydrocephalus or abnormal leptomeningeal enhancement
Major clinical/exposure criteria:
- Specific anticysticercal antibodies detected by EITB (enzyme-linked immunoelectrotransfer blot) - >99% specific and sensitive in patients with multiple cysts (note: single lesions or calcifications may be seronegative)
- Cysticercosis outside the CNS
- Household contact with T. solium infection
Minor clinical/exposure criteria:
- Clinical manifestations suggestive of NCC (seizures, obstructive hydrocephalus)
- Residence in an endemic region
Definitive diagnosis = 1 absolute criterion; OR 2 major criteria; OR 1 major neuroimaging + 1 major clinical/exposure + exclusion of other pathologies
- Harrison's Principles of Internal Medicine 22E (Del Brutto 2017 criteria)
Serology Notes
- EITB using lentil lectin-purified glycoproteins: >99% specific, highly sensitive for multiple cysts
- Standard ELISAs: HIGH false-positive and false-negative rates - should be avoided
- Antigen-detection assays (CSF, blood, urine) available in Europe; not in the US
- PCR increasingly used for extraparenchymal disease follow-up
Treatment
Step 1: Stabilize First
- Antiparasitic treatment is never an emergency and should never be started with elevated ICP
- Control seizures with antiseizure medications first
- Address hydrocephalus before antiparasitics
Step 2: Antiparasitic Therapy (by form)
| Form | Regimen |
|---|---|
| Parenchymal - 1-2 viable/enhancing cysts | Albendazole monotherapy + steroids |
| Parenchymal - >2 cysts | Albendazole + praziquantel combination + steroids |
| Calcified cysts | No antiparasitic treatment |
| Diffuse encephalitis / cerebral edema | No antiparasitics; steroids only |
| Intraventricular (surgically removable) | Neuroendoscopic removal (lateral/3rd ventricle); micro- or neuroendoscopic for 4th ventricle |
| Intraventricular (not removable) | Ventricular shunt FIRST, then antiparasitics + steroids |
| Subarachnoid | Shunt if hydrocephalus, then prolonged antiparasitics (albendazole ± praziquantel) |
| Ocular | Surgical resection (antiparasitics are contraindicated - inflammatory response destroys retina) |
| Spinal | Surgical removal or antiparasitics + steroids (individualized) |
- Bradley and Daroff's Neurology, Treatment Table 79.7 (IDSA/ASTMH 2018 guidelines)
Albendazole (Drug of Choice)
- Dose: 15 mg/kg/day (or 400 mg twice daily) for 8-28 days
- Preferred over praziquantel because:
- Shorter course
- Lower cost
- Better penetration into subarachnoid space
- Drug levels increase when given with corticosteroids (praziquantel levels decrease with steroids)
- Combination therapy (albendazole + praziquantel 50 mg/kg/day) is more effective for >2 cystic lesions or multiple subarachnoid cysts
Praziquantel
- Single dose 10 mg/kg for intestinal taeniasis
- Avoid initiating for taeniasis if CNS cysticercosis may be present (can trigger CNS inflammation)
- Used as adjunct to albendazole for multiple/extraparenchymal disease
Anti-inflammatory Therapy
- Always co-administer corticosteroids with antiparasitics (dexamethasone 0.1-0.4 mg/kg/day or prednisone 60 mg/day)
- Rationale: both antiparasitics cause inflammatory response around dying larvae → can worsen seizures or hydrocephalus
- Subarachnoid/giant cysticercosis requires prolonged anti-inflammatory treatment
- Katzung's Basic and Clinical Pharmacology 16th Ed., p. 1462; Harrison's, p. 1878
Seizure Management
- Antiseizure monotherapy is usually sufficient
- Single enhancing lesions: taper ASMs after 6 months if imaging normalizes and no breakthrough seizures
- Multiple parenchymal lesions: more prolonged therapy (~2 years), especially if calcifications develop
- Calcified lesions with perilesional edema/enhancement: higher risk of recurrent seizures
Intraventricular Hydrocephalus
- Neuroendoscopic cyst removal is preferred
- Avoid antiparasitics before surgery (make cysts friable and harder to remove)
- Shunt failure was historically a major problem; mitigated by antiparasitics + corticosteroids post-shunt
- Recent meta-analysis (PMID 40381508, 2025): Neuroendoscopic management of intraventricular NCC shows favorable outcomes as the preferred surgical approach
Prevention
- Access to clean water and sanitation
- Proper handwashing, especially when handling food
- Well-cooked pork (56°C for 5 minutes destroys cysticerci)
- Refrigeration or freezing (-10°C for 9 days) kills parasites
- Inspection of pork
- Treatment of tapeworm carriers prevents egg shedding and community transmission
Key Points Summary
- NCC = CNS infection by T. solium larvae; most common cause of epilepsy in the developing world
- Transmission is via ingestion of T. solium eggs, NOT contaminated pork (that causes intestinal taeniasis)
- Four radiological stages: vesicular → colloidal vesicular → granular nodular → calcified nodular
- Only vesicular and colloidal stages are treated with antiparasitics
- Albendazole is the drug of choice; combine with praziquantel for >2 cysts
- Always co-administer corticosteroids; never start antiparasitics with raised ICP
- Intraventricular cysts: neuroendoscopic removal is the primary approach
- EITB is the preferred serologic test (avoid standard ELISAs)
- Ocular cysticercosis: surgical only - antiparasitics contraindicated
Sources: Bradley and Daroff's Neurology in Clinical Practice | Harrison's Principles of Internal Medicine 22E | Katzung's Basic and Clinical Pharmacology 16th Ed. | Grainger & Allison's Diagnostic Radiology | Tintinalli's Emergency Medicine | Washington Manual of Medical Therapeutics | IDSA/ASTMH 2018 Clinical Practice Guidelines (White et al.)
Recent literature: Neuroendoscopic management meta-analysis (PMID 40381508, 2025); NCC-associated meningitis systematic review (PMID 42087630, 2026); Movement disorders in NCC (PMID 40822429, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.