Teach me physiology of thyroid gland and steps in hormone synthesis with peripheral conversion of T4 to T3 and thyroid function test in simplified manner as I'm 3rd year pg resident of medicine appearing for muhs theory exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the content needed to write a comprehensive, exam-focused answer. Let me compile everything.
Thyroid Gland - Complete Guide for MUHS PG Medicine Theory Exam
PART 1: ANATOMY & HISTOLOGY - Quick Recap
The thyroid gland is composed of spherical follicles, each lined by a single layer of follicular (epithelial) cells surrounding a central lumen filled with colloid (mainly thyroglobulin). Between follicles lie parafollicular C cells that secrete calcitonin.
Follicular cell height varies with activity:
- Flat/cuboidal = inactive (high colloid)
- Tall columnar = active (little colloid, scalloped edges = resorption lacunae)
PART 2: THYROID HORMONE PHYSIOLOGY
The HPT Axis (Hypothalamic-Pituitary-Thyroid)
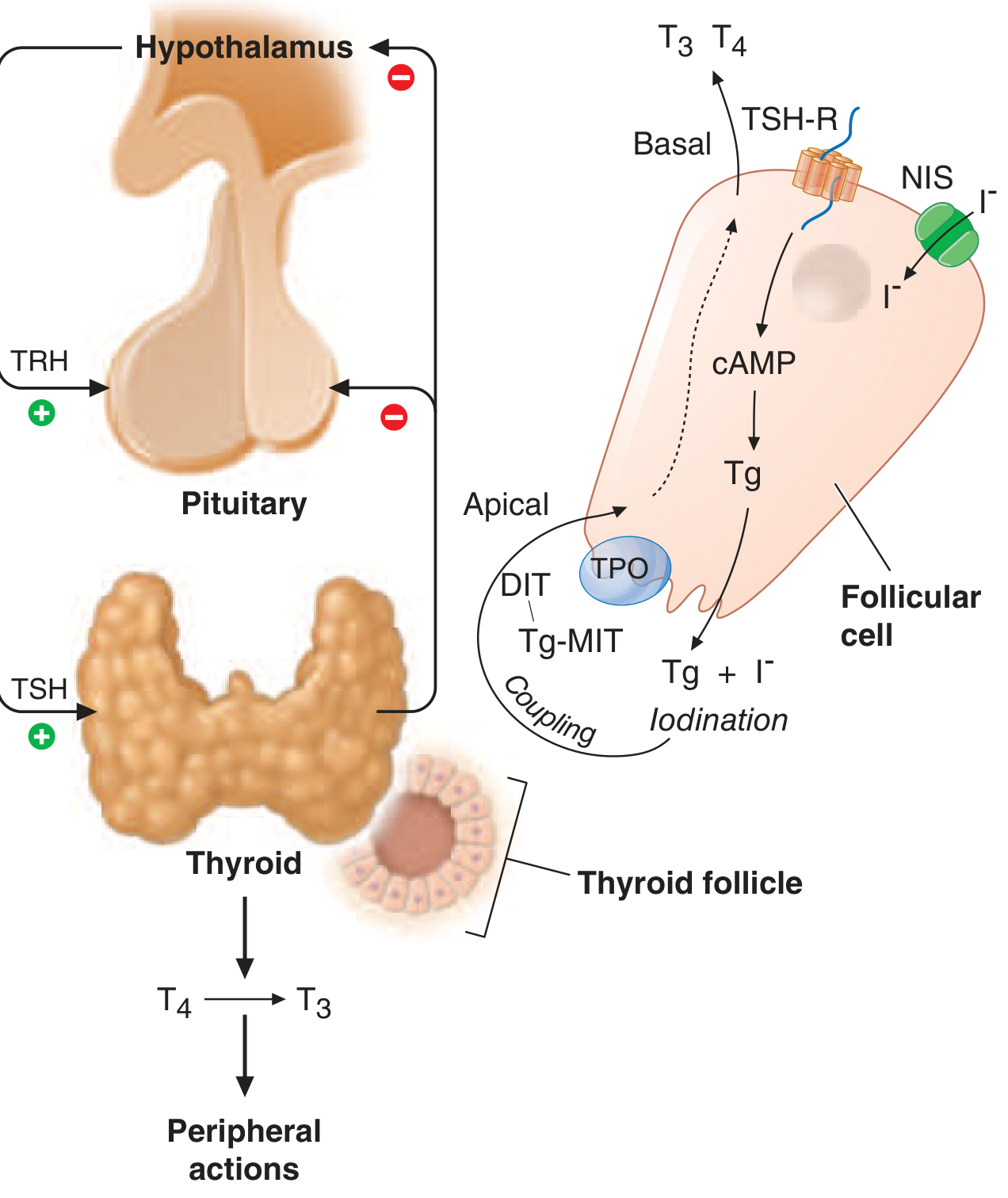
The axis works like this:
Hypothalamus → TRH (thyrotropin-releasing hormone)
↓
Anterior Pituitary → TSH (thyroid-stimulating hormone)
↓
Thyroid Gland → T4 (80 µg/day) + T3 (4 µg/day)
↓
NEGATIVE FEEDBACK: T3/T4 inhibit both hypothalamus and pituitary
Key points for exam:
- TRH is a tripeptide; acts via Gq/IP3/DAG → increases TSH
- TSH acts via Gs/cAMP → stimulates ALL steps of thyroid hormone synthesis
- TSH receptor (TSH-R) is also stimulated by TSI (thyroid-stimulating immunoglobulin) in Graves' disease
- T3 is 3-4x more potent than T4 and provides the main feedback signal (TSH secretion is inhibited by intrapituitary T3 generated by type 2 deiodinase from circulating T4)
PART 3: STEPS IN THYROID HORMONE SYNTHESIS
Remember this with the mnemonic: "TOPIC" - Trapping → Oxidation → Protein binding (organification) → Iodotyrosine coupling → Cleavage & secretion
Step-by-Step (Ganong + Katzung)
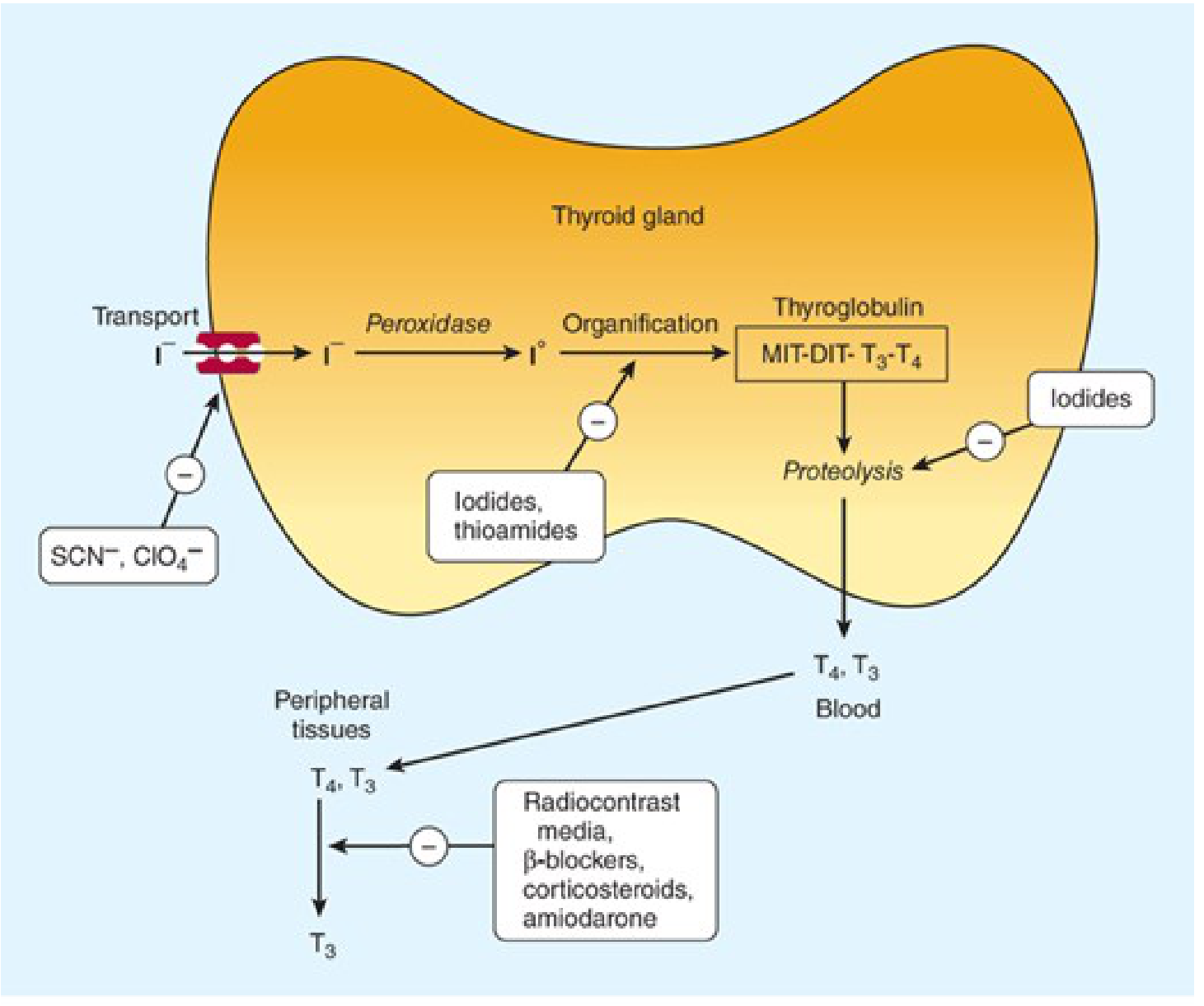
Step 1: Iodide Trapping (Active Transport)
- Iodide (I⁻) is actively transported from blood into the follicular cell against a concentration gradient via the NIS (Sodium-Iodide Symporter) at the basolateral membrane
- NIS co-transports 2 Na⁺ with each I⁻ (secondary active transport)
- Normal gradient is 20:1 (thyroid:plasma); in Graves' disease it rises to 70-90:1
- Inhibited by: thiocyanate (SCN⁻), perchlorate (ClO₄⁻), pertechnetate (TcO₄⁻) - these are competitive anion inhibitors
- TSH upregulates NIS expression
At the apical membrane, iodide is effluxed into the colloid by pendrin (encoded by SLC26A4)
- Pendrin mutation → Pendred syndrome (goiter + sensorineural deafness)
Step 2: Oxidation of Iodide → Iodine
- Iodide (I⁻) is oxidized to iodine (I⁰) by thyroid peroxidase (TPO) using H₂O₂
- H₂O₂ is generated by NADPH oxidase (Dual oxidase/DUOX)
- TPO is a membrane-bound enzyme on the apical surface
Blocked by: thioamide drugs (PTU, carbimazole/methimazole) - these are the most clinically important inhibitors; also blocked transiently by high intrathyroidal iodide (Wolff-Chaikoff effect)
Step 3: Organification (Iodination of Thyroglobulin)
- Iodine (I⁰) reacts with tyrosine residues on thyroglobulin (Tg) in the colloid
- Thyroglobulin is a large glycoprotein (660 kDa) with 123 tyrosine residues - only 4-8 are actually iodinated
- Products formed:
- Iodination of 1 tyrosine → MIT (monoiodotyrosine)
- Iodination of 2 positions → DIT (diiodotyrosine)
- This step is also catalyzed by TPO
- Also blocked by thioamides and high iodide (Wolff-Chaikoff effect)
Step 4: Coupling (Condensation)
- Two iodotyrosines are coupled (still on thyroglobulin) by TPO via an oxidative condensation reaction:
- DIT + DIT → T4 (thyroxine, 3,5,3',5'-tetraiodothyronine)
- MIT + DIT → T3 (3,5,3'-triiodothyronine)
- MIT + MIT → rT3 (reverse T3, biologically inactive) - minor pathway
- The ratio of T4:T3 in thyroglobulin is approximately 5:1
- MIT and DIT that are not used in coupling remain stored in thyroglobulin
Step 5: Storage in Colloid
- Thyroglobulin (containing MIT, DIT, T3, T4) is stored in the colloid
- Humans can go up to 2 months without dietary iodine before hormone levels fall - this is the largest hormone store in the body
Step 6: Reabsorption & Proteolysis (Secretion)
- TSH stimulates endocytosis of colloid back into the follicular cell
- Lysosomes fuse with the endosomes → proteolytic cleavage of Tg by cathepsins
- Free T4 and T3 are released into the cytosol and then into capillaries
- MIT and DIT are deiodinated by iodotyrosine deiodinase (microsomal enzyme) within the gland → iodide is recycled back for new synthesis
- Congenital absence of this enzyme → MIT/DIT in urine → iodine deficiency symptoms
Blocked by: high iodide (Wolff-Chaikoff), lithium
Summary Table: Drugs and Their Blockade Points
| Drug | Step Blocked |
|---|---|
| Thiocyanate, Perchlorate | Iodide trapping (NIS) |
| PTU, Methimazole/Carbimazole | Oxidation + Organification + Coupling (TPO inhibition) |
| PTU additionally | Peripheral T4→T3 conversion (D1 inhibition) |
| High dose iodide (Wolff-Chaikoff) | Organification + Proteolysis |
| Lithium | Proteolysis/secretion |
PART 4: PERIPHERAL CONVERSION OF T4 → T3
The Key Concept
The thyroid secretes:
- ~80 µg T4/day (major secretory product - a "prohormone")
- ~4 µg T3/day
- ~2 µg rT3/day
But 80% of circulating T3 comes from peripheral deiodination of T4, not direct thyroid secretion!
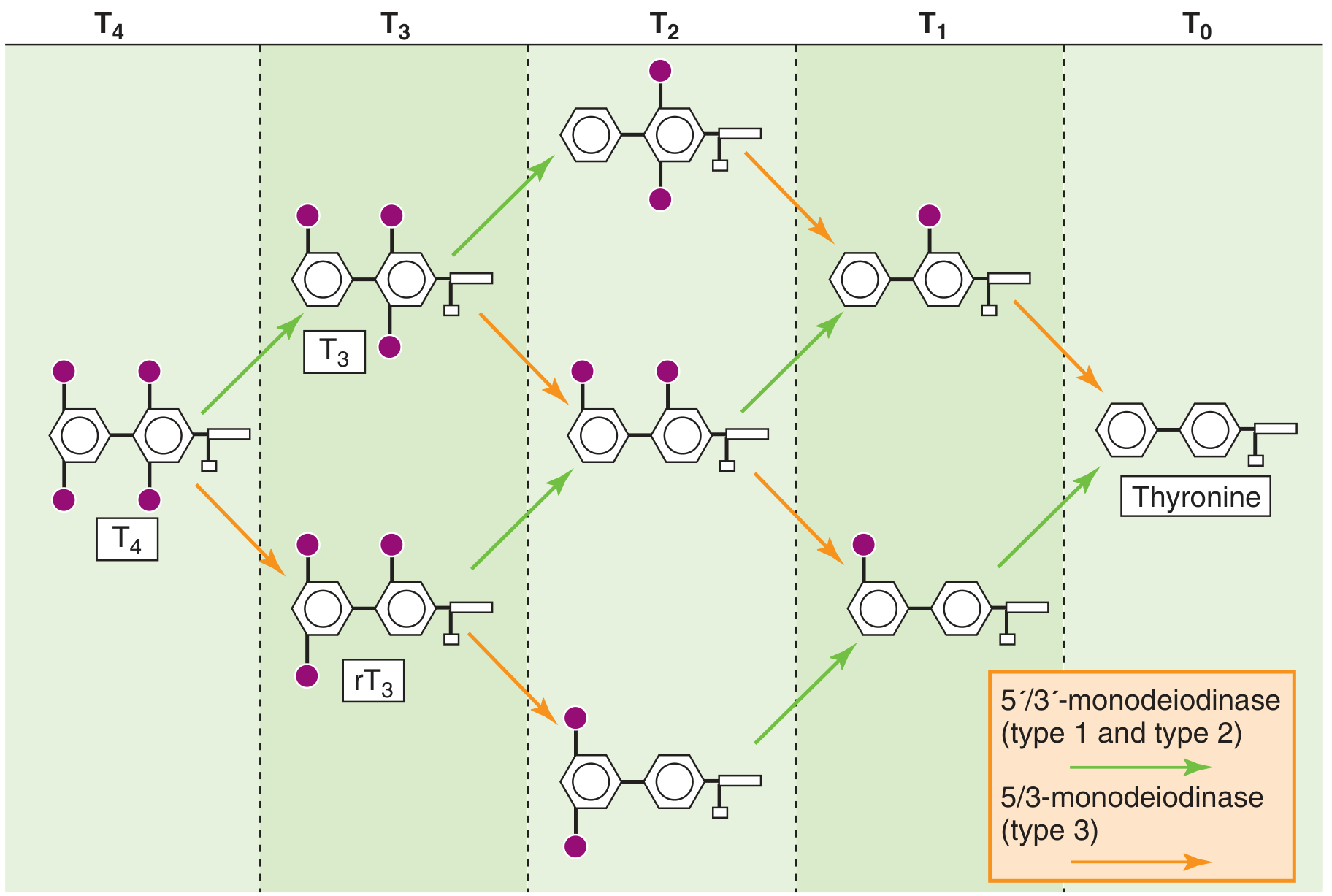
The Three Deiodinase Enzymes (Medical Physiology - Boron & Boulpaep)
| Enzyme | Location | Action | Product | Clinical relevance |
|---|---|---|---|---|
| Type 1 (D1) 5'-deiodinase | Liver, kidney, skeletal muscle, thyroid | Removes I from outer ring | T4 → T3 (active) | Responsible for ~24% circulating T3; inhibited by PTU, amiodarone, steroids, starvation |
| Type 2 (D2) 5'-deiodinase | Pituitary, CNS, placenta, brown fat | Removes I from outer ring (local use) | T4 → T3 (local) | Supplies local T3 to pituitary for TSH feedback (64% of peripheral T3); NOT inhibited by caloric restriction |
| Type 3 (D3) 5-deiodinase | Placenta, brain, skin | Removes I from inner ring | T4 → rT3 (inactive) T3 → T2 | Inactivating enzyme; high in fetal life; high in illness |
The Outer Ring vs Inner Ring Concept
Think of T4 as having two benzene rings joined by an ether bridge:
- Outer ring (phenolic/distal ring) - iodine at 3' and 5' positions
- Inner ring (tyrosyl/proximal ring) - iodine at 3 and 5 positions
Removing iodine from the outer ring (5' position) by D1/D2 → T3 (biologically ACTIVE - 3-4x more potent than T4)
Removing iodine from the inner ring (5 position) by D3 → rT3 (reverse T3 - biologically INACTIVE)
Sick Euthyroid Syndrome (Low T3 Syndrome) - Exam High Yield
In critical illness, starvation, caloric restriction:
- D1 activity decreases → less T4→T3 conversion → low T3
- D3 activity increases → more T4→rT3 → high rT3
- D2 (pituitary) is UNAFFECTED → local T3 in pituitary remains normal → TSH does not rise (no compensatory rise)
- Pattern: Low T3, high rT3, normal/low TSH, normal/low T4
This is teleologically appropriate - reduced metabolic rate is beneficial in severe illness/starvation.
PART 5: TRANSPORT OF THYROID HORMONES IN BLOOD
T4 and T3 are lipophilic and travel bound to proteins:
| Protein | Binds | Notes |
|---|---|---|
| TBG (thyroxine-binding globulin) | ~70% T4, ~80% T3 | Main carrier; most clinically important |
| Transthyretin (TTR/prealbumin) | ~20% T4 | Also a carrier for retinol |
| Albumin | ~10% T4 | Low affinity, high capacity |
Free hormone fractions:
- Free T4: ~0.02-0.04% of total T4
- Free T3: ~0.2-0.4% of total T3
- Only free hormones are biologically active and provide feedback
TBG is increased by: pregnancy, OCP, estrogens, hepatitis, hypothyroidism → total T4/T3 elevated but free hormone normal
TBG is decreased by: androgens, steroids, nephrotic syndrome (urinary loss), malnutrition, hypothyroidism → total T4/T3 low but free hormone normal
PART 6: THYROID FUNCTION TESTS (TFTs)
Test Hierarchy: "TSH First" Policy
Step 1: TSH (best initial screening test)
→ Normal TSH = essentially excludes thyroid dysfunction
→ Abnormal TSH → Add Free T4
→ If hyperthyroid and T4 normal → Add Free T3 (rule out T3-toxicosis)
Interpretation Table (Quick Compendium of Clinical Pathology)
| Condition | TSH | Free T4 | Free T3 | Total T4 | rT3 |
|---|---|---|---|---|---|
| Primary Hyperthyroidism | ↓↓ | ↑ | ↑ | ↑ | → |
| Primary Hypothyroidism | ↑↑ | ↓ | ↓ | ↓ | →/↓ |
| Secondary/Tertiary Hypothyroidism (pituitary/hypothalamic) | ↓ or → | ↓ | ↓ | ↓ | - |
| Sick Euthyroid Syndrome | →/↓ | →/↓ | ↓↓ | →/↓ | ↑↑ |
| Subclinical Hypothyroidism | ↑ | → (normal) | → | → | - |
| Subclinical Hyperthyroidism | ↓ | → (normal) | → | → | - |
| T3-toxicosis | ↓ | → | ↑ | → | - |
| TBG excess (pregnancy, OCP) | → | → | → | ↑ (total) | - |
High-yield point: TSH is the most sensitive indicator of thyroid status because of the log-linear relationship - small changes in free T4 cause large changes in TSH.
Individual Tests Explained
1. TSH (0.4 - 4.0 mIU/L)
- Best single test; third-generation immunometric assay can detect down to 0.01 mIU/L
- Pitfalls: Do not use TSH alone when:
- Central hypothyroidism suspected (pituitary/hypothalamic disease - TSH is low/normal but T4 is low)
- Critically ill patients (sick euthyroid)
- Early in treatment (TSH lags - takes 6-8 weeks to normalize after treatment)
- Dopamine infusion, high-dose steroids (suppress TSH spuriously)
2. Free T4 (fT4) - 0.8 to 1.8 ng/dL
- Reflects biologically active hormone unaffected by TBG changes
- Second-line test when TSH is abnormal
- Preferred over total T4 in pregnancy and states altering binding proteins
3. Free T3 (fT3)
- Used to diagnose T3-toxicosis (elevated T3 with normal T4)
- Useful in monitoring hyperthyroid treatment
4. Total T4 and Total T3
- Affected by TBG levels - less reliable
- Still used in some settings
5. rT3
- Elevated in sick euthyroid syndrome
- Helps distinguish sick euthyroid from true hypothyroidism
6. Thyroglobulin (Tg)
- Tumor marker after total thyroidectomy for differentiated thyroid cancer
- Rising Tg = recurrence
7. TPO Antibodies (Anti-TPO)
- Present in ~95% Hashimoto's thyroiditis, ~80% Graves' disease
- Best test for autoimmune thyroid disease
8. TSI / TRAb (TSH Receptor Antibody)
- Pathognomonic for Graves' disease
- Useful in pregnancy to predict neonatal Graves'
9. T3 Resin Uptake (T3RU) - now largely obsolete
- Radiolabeled T3 added to patient serum → binds unoccupied TBG sites
- Low T3RU = more TBG sites available = low T3 state (hypothyroidism/elevated TBG)
- High T3RU = fewer TBG sites = high T3 state (hyperthyroidism/low TBG)
- Free Thyroxine Index (FTI) = Total T4 × T3RU (corrects for TBG changes)
When TSH-First Policy Should Be Abandoned
- Critically ill patients - sick euthyroid distorts all parameters
- Central hypothyroidism - TSH is low/normal despite T4 deficiency
- Early treatment monitoring - TSH lags weeks behind clinical response; use free T4
- Dopamine or high-dose steroids - suppress TSH independently
PART 7: ACTIONS OF THYROID HORMONES (Brief - for completeness)
T3 enters the cell nucleus and binds thyroid hormone receptors (TR-alpha, TR-beta) which heterodimerize with Retinoid X Receptors (RXR) and bind to Thyroid Response Elements (TRE) on DNA.
- Without T3: TR binds co-repressors → gene silencing
- With T3: co-repressors released → co-activators recruited → gene transcription
Effects of T3:
- Increases BMR, O₂ consumption (calorigenesis)
- Increases heart rate and cardiac output (upregulates beta-adrenergic receptors)
- Promotes growth and CNS development (critical in fetal/neonatal life)
- Promotes protein synthesis and gluconeogenesis
- Essential for normal bone maturation
EXAM MEMORY AIDS
Steps in synthesis - mnemonic "TOPIC":
T - Trapping (NIS, basolateral)
O - Oxidation (TPO + H₂O₂)
P - Protein iodination / organification (MIT, DIT formed on Tg)
I - Iodotyrosine Coupling (DIT+DIT=T4; MIT+DIT=T3)
C - Cleavage & secretion (endocytosis → lysosomal proteolysis → T3/T4 released)
Deiodinases - mnemonic "1 and 2 ACTIVATE, 3 INACTIVATES":
- D1/D2 = outer ring removal = T3 (active)
- D3 = inner ring removal = rT3 (inactive)
- PTU blocks D1 (not D2, not D3) - clinically useful in thyroid storm
TFT pattern to memorize:
- Low TSH + High T4 = Hyperthyroid (primary)
- High TSH + Low T4 = Hypothyroid (primary)
- Low TSH + Low T4 = Central hypothyroidism or sick euthyroid
- Normal TSH + Low T4 = Check TBG (TBG deficiency or sick euthyroid)
Sources: Ganong's Review of Medical Physiology 26e; Harrison's Principles of Internal Medicine 22e (2025); Katzung's Basic and Clinical Pharmacology 16e; Medical Physiology (Boron & Boulpaep); Quick Compendium of Clinical Pathology 5e
This is a shared conversation. Sign in to Orris to start your own chat.