Sglt2 inhibitor drug causing fourniers
Reading File
Finding Sources
Searching PubMed
SGLT2 inhibitor Fournier gangrene
Reading File
Reading File
Reading File
Here is a complete summary of SGLT2 inhibitors and Fournier's gangrene, drawn from multiple authoritative textbooks:
SGLT2 Inhibitors and Fournier's Gangrene
The Drug Class
All SGLT2 inhibitors carry this risk as a class effect. The approved agents in the US are:
- Canagliflozin
- Dapagliflozin
- Empagliflozin
- Ertugliflozin
No single agent is uniquely implicated - the FDA warning applies to the entire class.
What is Fournier's Gangrene?
Fournier's gangrene (also called necrotizing fasciitis of the perineum) is:
-
A severe, rapidly progressing necrotizing infection of the external genitalia, perineum, or perianal area
-
Polymicrobial in nature (mixed aerobic and anaerobic organisms)
-
Life-threatening without urgent surgical intervention
-
Dermatology 2-Volume Set, 5e
FDA Warning (2018)
In August 2018, the FDA released a safety communication based on 12 post-marketing cases of Fournier's gangrene associated with SGLT2 inhibitor use - a rare but serious adverse effect. This prompted labeling updates for all drugs in the class.
- Fuster and Hurst's The Heart, 15th Edition
Mechanism / Why SGLT2 Inhibitors Cause This
SGLT2 inhibitors work by causing glycosuria (spilling glucose into the urine). This creates a glucose-rich perineal environment that:
- Promotes bacterial and fungal overgrowth in the genital/perineal area
- Increases susceptibility to urogenital infections (a well-known class effect)
- In predisposed patients (especially diabetics, immunocompromised), this can progress to deep-tissue necrotizing infection
The underlying diabetes itself is an independent risk factor for Fournier's gangrene, as is immunosuppression.
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Lippincott Illustrated Reviews: Pharmacology
Other Risk Factors That Compound the Risk
| Risk Factor | Notes |
|---|---|
| Diabetes mellitus | Independent predisposing condition |
| Immunosuppression | Reduces ability to fight infection |
| Poor perineal hygiene | Direct risk factor |
| Combination with sulfonylurea/insulin | Increases hypoglycemia risk, worsens metabolic milieu |
Management of Fournier's Gangrene
- Emergency surgical debridement - wide and extensive
- Prolonged systemic antibiotics (broad-spectrum, covering polymicrobial flora)
- Discontinue the SGLT2 inhibitor immediately
- Supportive care / ICU level management
Other Notable Adverse Effects of SGLT2 Inhibitors (for context)
- Genital mycotic infections (most common; same glycosuria mechanism)
- UTIs
- Volume depletion / hypotension
- DKA at near-normal glucose levels ("euglycemic DKA")
- Bone fractures (canagliflozin)
- Modest LDL increase (canagliflozin, empagliflozin: 4-8%)
- Renal insufficiency (especially in CKD)
Key exam point: Fournier's gangrene with SGLT2 inhibitors is a class effect, not specific to one drug. The mnemonic to remember: glycosuria → perineal glucose → necrotizing infection. Patients should be counseled on perineal hygiene and to seek urgent care for any genital/perineal pain, swelling, or fever.
Stain of hsv
Finding Sources
Reading File
Reading File
Loading Image
Staining for HSV - Complete Summary
1. Tzanck Smear (Classic / Most Tested)
How it is done:
- Scrape the base of a freshly ruptured vesicle
- Stain with Giemsa or Wright's stain (Papanicolaou stain can also be used)
- Examine microscopically for multinucleated giant cells (Tzanck cells)
What you see:
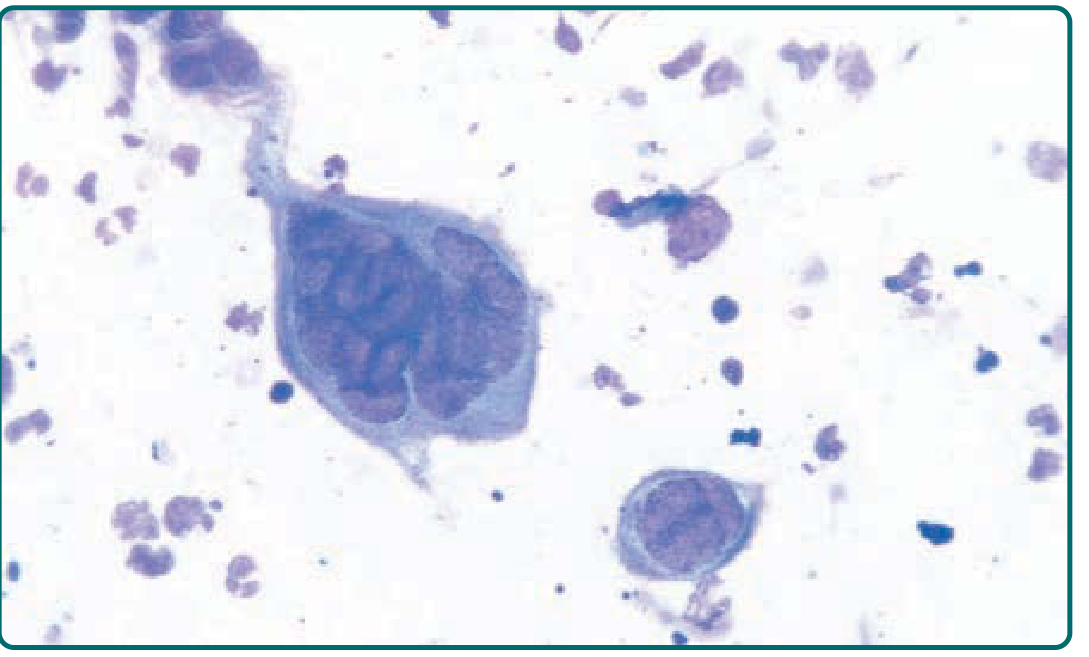
Giemsa-stained smear from a vesicle base showing a giant multinucleated keratinocyte (Tzanck cell). Compare its size with surrounding neutrophils.
- Fitzpatrick's Dermatology, 5e
Key Points to Remember
| Feature | Detail |
|---|---|
| Test name | Tzanck smear / Tzanck test |
| Stains used | Giemsa (most common), Wright's, Papanicolaou |
| Finding | Multinucleated giant cells (Tzanck cells) + intranuclear eosinophilic inclusions |
| Sensitivity | Low - positive in <40% of culture-proven cases; even lower (<30%) for mucosal swabs |
| Specificity problem | Cannot distinguish HSV from VZV - both cause identical Tzanck cell changes |
| Specimen | Scraping from base of freshly ruptured vesicle |
2. Direct Fluorescent Antibody (DFA) Staining
- Stains lesion scrapings with fluorescent-labeled antibodies
- More sensitive than Tzanck smear, but less sensitive than viral culture
- Can be used as an alternative rapid test
3. Skin Biopsy (Histopathology)
On H&E or special stains, biopsy shows:
- Enlarged, swollen epithelial cells that are often separated (ballooning degeneration)
- Multinucleated cells
- Intranuclear eosinophilic inclusion bodies (Cowdry type A inclusions)
4. Gold Standard: PCR + Viral Culture
| Method | Notes |
|---|---|
| PCR | Most sensitive; preferred for CNS/neonatal HSV; can type HSV-1 vs HSV-2 |
| Viral culture | Cytopathic effect visible in 48-96 hours; spin-amplified culture can give result in <24 hours; needed for antiviral sensitivity testing |
Summary Hierarchy (Sensitivity)
PCR > Viral culture > DFA staining > Tzanck smear
Exam pearl: The Tzanck smear is positive in HSV and VZV - it does NOT differentiate between the two. For HSV-1 vs HSV-2 typing, PCR or culture is required. - Harrison's Principles of Internal Medicine, 22e
This is a shared conversation. Sign in to Orris to start your own chat.