Spaces of head and neck 20 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Excellent - I have a comprehensive parapharyngeal space diagram. Now I have all the information needed to write a thorough MS ENT exam answer. Let me compile the full answer:
Spaces of the Head and Neck
Introduction
The head and neck contain a series of potential fascial spaces defined by the layers of the deep cervical fascia. These spaces are clinically important because they act as pathways for the spread of infection, tumor, and hemorrhage. Understanding their boundaries, contents, and communications is essential for diagnosis and surgical management.
Fascial Layers - The Foundation
The cervical fascia is divided into:
Superficial cervical fascia - a thin subcutaneous layer containing platysma, fat, and cutaneous nerves.
Deep cervical fascia - has three layers:
- Investing (superficial) layer - encircles the entire neck; splits to enclose sternocleidomastoid, trapezius, parotid gland, and submandibular gland.
- Middle (pretracheal) layer - has a muscular portion (strap muscles) and a visceral portion (enclosing thyroid, trachea, esophagus).
- Deep (prevertebral) layer - encircles the vertebral column and paravertebral muscles; has an alar fascial subdivision anteriorly.
The carotid sheath is a condensation of all three layers of deep cervical fascia and forms the boundary of the carotid space.
Classification of Head and Neck Spaces
SUPRAHYOID SPACES
1. Parapharyngeal Space (PPS)
The "Central" or "Pivot" Space - the most important anatomical landmark for understanding suprahyoid neck anatomy.
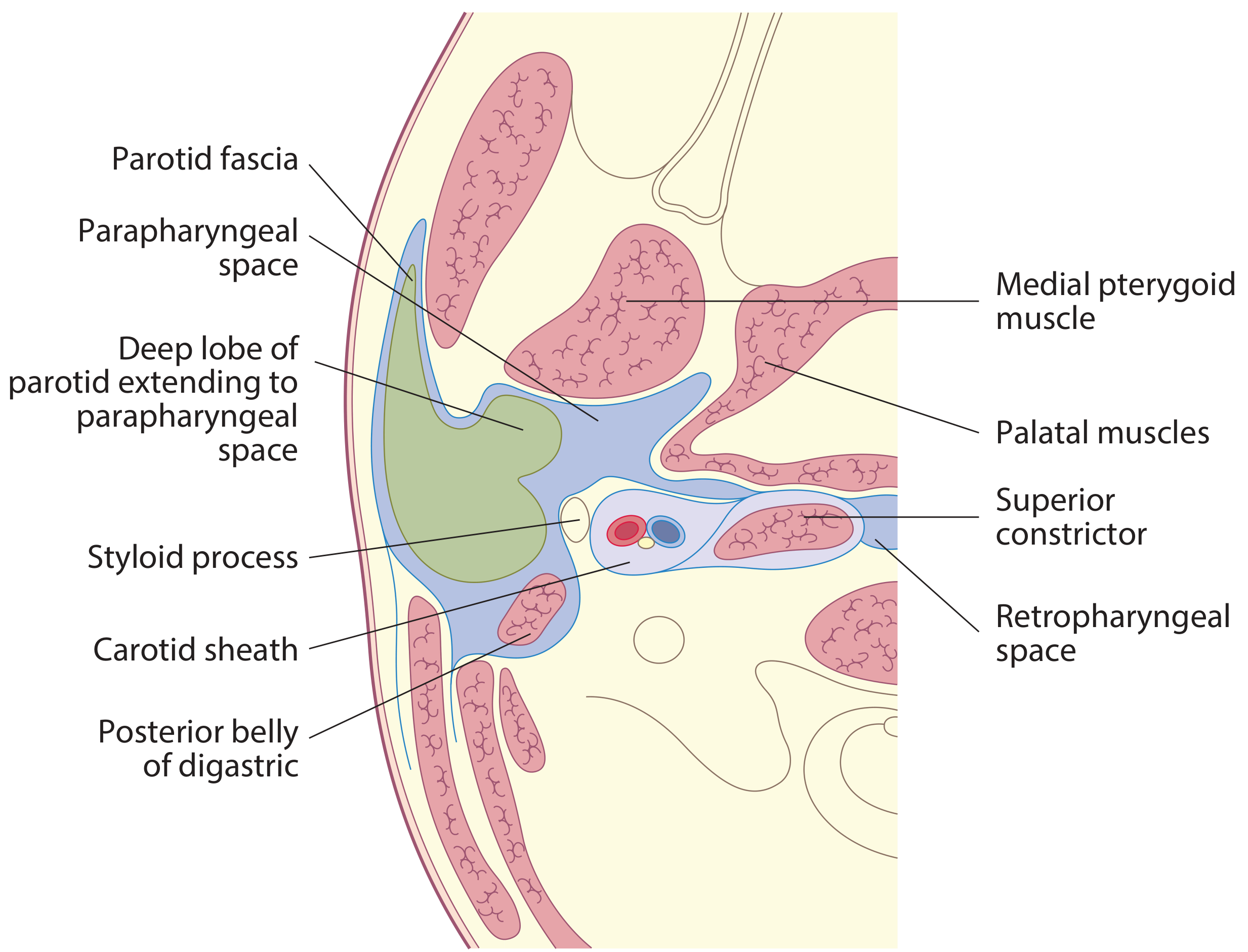
Shape: Inverted pyramid (on axial imaging: triangular; on coronal: hourglass shape, thicker at skull base and hyoid, narrower in the midportion).
Extent: Petrous temporal bone / skull base (superiorly) to the level of the hyoid bone (inferiorly).
Boundaries:
| Wall | Structure |
|---|---|
| Medial | Pharyngobasilar fascia superiorly; superior constrictor muscle |
| Lateral | Mandibular ramus, medial pterygoid muscle, deep lobe of parotid |
| Anterior | Pterygomandibular raphe |
| Posterior | Prevertebral fascia |
Division by the Styloid Process:
The styloid process and its associated muscles (stylopharyngeus, styloglossus, stylohyoid) and ligaments (stylomandibular and stylohyoid ligaments) divide the PPS into two compartments:
Pre-styloid compartment (muscular/anterior):
- Fat and loose connective tissue
- Internal maxillary artery
- Inferior alveolar nerve, lingual nerve, auriculotemporal nerve
- Lymph nodes
- Deep lobe of parotid tissue
Post-styloid compartment (neurovascular/posterior) = Carotid space:
- Internal carotid artery
- Internal jugular vein
- Cranial nerves IX (glossopharyngeal), X (vagus), XI (accessory), XII (hypoglossal)
- Sympathetic chain
- Lymph nodes
Communications: Communicates with the retropharyngeal space posteriorly (key route for infection spread), submandibular space inferiorly, and peritonsillar space anteromedially.
Clinical significance:
- Acts as the pivot space - displacement of PPS fat pad on imaging localizes adjacent space lesions
- Pre-styloid lesions (e.g., deep lobe parotid tumors) displace the carotid sheath and fat pad posteromedially
- Post-styloid lesions (e.g., glomus tumors, schwannomas) displace the fat pad anteriorly
- PPS infections can arise from adjacent submandibular or peritonsillar spaces
2. Pharyngeal Mucosal Space (PMS)
Boundaries: Mucosal surface of the pharynx to the pharyngobasilar fascia / buccopharyngeal fascia.
Contents: Mucosa, lymphoid tissue (Waldeyer's ring - nasopharyngeal tonsil, palatine tonsils, lingual tonsils), minor salivary glands, and the pharyngeal constrictor muscles.
Clinical significance: Primary site for squamous cell carcinoma of the pharynx, nasopharyngeal carcinoma, and lymphoma.
3. Masticator Space (MS)
Also known as the infratemporal fossa space.
Boundaries: Enclosed by the investing layer of deep cervical fascia which splits around the masseter and pterygoid muscles and inserts on the mandible. Extends superiorly to include the temporal fossa (suprazygomatic masticator space).
Contents:
- Masseter muscle
- Temporalis muscle
- Medial and lateral pterygoid muscles
- Motor branch of V3 (mandibular nerve)
- Inferior alveolar nerve
- Internal maxillary artery and branches
- Pterygoid venous plexus
- Ramus and posterior body of mandible
Relationship to PPS: A mass in the masticator space displaces the PPS posteriorly and medially.
Clinical significance:
- Odontogenic infections - abscesses, cellulitis, osteomyelitis (most common source: dental caries)
- Trismus (spasm of pterygoid muscles) is the hallmark symptom
- Juvenile nasopharyngeal angiofibroma characteristically extends from the pterygopalatine fossa into the masticator space
- Perineural spread of malignancy along V3
4. Parotid Space (PS)
Formation: The investing layer of deep cervical fascia splits to encompass the parotid gland.
Contents:
- Parotid gland (superficial and deep lobes)
- Facial nerve (CN VII) and its branches
- Retromandibular vein
- Terminal branches of external carotid artery (superficial temporal and maxillary arteries)
- Parotid lymph nodes (intraparotid lymph nodes)
Clinical significance:
- Parotid gland tumors (pleomorphic adenoma most common benign; mucoepidermoid carcinoma most common malignant)
- Deep lobe tumors extend into the pre-styloid PPS through the stylomandibular tunnel, presenting as a parapharyngeal mass with the classic "dumbbell" appearance on imaging
5. Submandibular Space
Boundaries:
- Superior: mucosa of the floor of mouth
- Inferior: investing layer of deep cervical fascia
- Lateral/anterior: mandible
- Medial: mylohyoid, hyoglossus, genioglossus muscles
- The mylohyoid muscle divides this region into:
- Sublingual space (above mylohyoid)
- Submandibular space proper (below mylohyoid)
Contents (submandibular space):
- Submandibular salivary gland (superficial lobe)
- Lymph nodes (levels IA, IB)
- Facial artery and vein
Contents (sublingual space):
- Sublingual salivary gland
- Deep lobe of submandibular gland and Wharton's duct
- Lingual nerve and artery
- Hypoglossal nerve (CN XII)
- Genioglossus and geniohyoid muscles
Communication: Freely communicates bilaterally around the posterior edge of mylohyoid - this is why Ludwig's angina is a bilateral infection. The sublingual and submandibular spaces communicate posteriorly around the free edge of mylohyoid.
Ludwig's Angina:
- Rapidly spreading cellulitis of the submandibular and sublingual spaces bilaterally
- 70-80% odontogenic origin (lower 2nd/3rd molar infections)
- Can also arise from submandibular sialadenitis, lymphadenitis, or trauma
- Life-threatening - elevated floor of mouth, posterior displacement of tongue, airway compromise
- Management: Airway first (awake fiber-optic intubation/tracheostomy), IV broad-spectrum antibiotics, surgical drainage
6. Peritonsillar Space
Boundaries: The potential space between the palatine tonsil capsule and the superior constrictor muscle.
Contents: Loose areolar tissue only (potential space).
Clinical significance:
- Peritonsillar abscess (Quinsy) - most common deep space infection of the head and neck
- Occurs when tonsillitis breaches the tonsillar capsule
- Presents with unilateral throat pain, muffled "hot potato" voice, uvular deviation, trismus
- Treatment: Needle aspiration or incision and drainage + antibiotics
- Untreated: spreads to the parapharyngeal space
INFRAHYOID AND MIDLINE SPACES
7. Retropharyngeal Space (RPS)
One of the most important spaces due to its route for infection spread.
Boundaries:
| Anterior | Middle layer of deep cervical fascia (buccopharyngeal fascia) encasing pharyngeal constrictors |
| Posterior | Alar fascia (anterior layer of prevertebral fascia) |
| Superior | Skull base |
| Inferior | T3 vertebral level (upper mediastinum) |
| Lateral | Carotid sheaths bilaterally |
Contents:
- Fat
- Retropharyngeal lymph nodes:
- Nodes of Rouviere (lateral retropharyngeal nodes) - the most clinically important; prominent in children, normally involute in adults; >5 mm is suspicious in adults
- Medial retropharyngeal nodes
Communications: Lies between the two parapharyngeal spaces and communicates with both; extends inferiorly to the posterior mediastinum.
Retropharyngeal abscess:
- More common in children (age 1-6 years) - secondary to lymph node suppuration from upper respiratory/dental infections
- Presents with fever, stiff neck, dysphagia, muffled voice, torticollis, stridor
- Lateral neck X-ray: widened prevertebral soft tissue shadow (>7 mm at C2, >14 mm at C6 in children; >22 mm at C6 in adults)
- CT scan: confirms diagnosis, gas indicates anaerobic infection
- Treatment: Airway management, IV antibiotics, transoral or transcervical drainage
- Complications: Airway obstruction, aspiration, mediastinitis via danger space
8. "Danger Space" (Alar Space)
Boundaries:
- Anterior: Alar fascia
- Posterior: Prevertebral fascia proper
Extent: From skull base to the diaphragm (T12) - the longest of all neck spaces.
Clinical significance: This is why it is called the "danger space" - infections in this space can spread unimpeded from the neck into the posterior mediastinum all the way to the diaphragm, causing:
- Descending necrotizing mediastinitis (30-40% mortality)
- Empyema
- Pericarditis
9. Prevertebral Space (PVS)
Boundaries:
- Anterior: Prevertebral fascia (deep layer of deep cervical fascia)
- Posterior: Vertebral column and paraspinal musculature
Extent: Skull base to coccyx.
Divided into:
- Anterior compartment: Prevertebral and scalene muscles, vertebral bodies, phrenic nerve, brachial plexus, vertebral artery and vein
- Posterior compartment: Posterior spinal elements, paraspinous musculature
Clinical significance:
- Infections reach here via direct pharyngeal/esophageal perforation or breach of alar fascia
- Causes: spinal osteomyelitis (Pott's spine - TB most common), epidural abscess
- In head and neck malignancy: prevertebral space invasion = inoperable disease (cannot be cleared surgically)
- Anterior PVS mass thickens prevertebral muscles and displaces PPS anteriorly
10. Carotid Space (CS)
Formation: Condensation of all three layers of deep cervical fascia forming the carotid sheath. Essentially corresponds to the post-styloid compartment of PPS in the suprahyoid neck; extends into the infrahyoid neck.
Contents:
- Common carotid artery (bifurcates at C4 into ICA and ECA)
- Internal jugular vein
- Vagus nerve (CN X)
- Deep cervical lymph nodes (levels II, III, IV)
- Sympathetic chain (runs within/adjacent to sheath)
Clinical significance:
- Carotid body tumors (chemodectoma / paraganglioma) - at carotid bifurcation; splays ICA and ECA ("lyre sign" on angiography); pulsatile neck mass
- Glomus vagale tumors (vagal paraganglioma)
- Jugular foramen tumors
- Carotid artery aneurysm
- Internal jugular vein thrombosis (Lemierre's syndrome - septic thrombophlebitis following peritonsillar or parapharyngeal infection)
11. Visceral Space (Infrahyoid)
Boundaries: Middle layer of deep cervical fascia (pretracheal fascia) anteriorly and posteriorly.
Contents:
- Larynx
- Hypopharynx
- Cervical trachea
- Cervical esophagus
- Thyroid and parathyroid glands
- Level VI lymph nodes
Clinical significance: Infections can arise from esophageal perforation or thyroid abscess. Thyroid malignancy can invade the prevertebral space.
Summary Table of Key Spaces
| Space | Extent | Key Contents | Key Clinical Feature |
|---|---|---|---|
| Parapharyngeal | Skull base to hyoid | Fat, V3 branches, internal maxillary A | Central pivot space; pre/post styloid division |
| Masticator | Temporal fossa to mandible | Pterygoids, masseter, mandible, V3 | Odontogenic infection; trismus |
| Parotid | Around parotid gland | Parotid gland, CN VII, retromandibular V | Parotid tumors, dumbbell extension |
| Peritonsillar | Tonsil to superior constrictor | Loose areolar tissue | Quinsy - most common deep neck abscess |
| Submandibular | Floor of mouth | Submandibular gland, nodes | Ludwig's angina - bilateral, airway danger |
| Retropharyngeal | Skull base to T3 | Fat, nodes of Rouviere | Retropharyngeal abscess; route to mediastinum |
| Danger space | Skull base to diaphragm | Areolar tissue | Descending mediastinitis - 30-40% mortality |
| Prevertebral | Skull base to coccyx | Prevertebral muscles, vertebrae, brachial plexus | PVS invasion = inoperable malignancy |
| Carotid | Skull base to aortic arch | ICA, IJV, CN X | Carotid body tumor, Lemierre's syndrome |
| Visceral | Hyoid to superior mediastinum | Thyroid, larynx, trachea, esophagus | Esophageal perforation, thyroid malignancy |
Spread of Infection Between Spaces
Understanding the interconnections between spaces is critical for MS ENT exams:
Dental/Tonsillar infection
↓
Peritonsillar space → Parapharyngeal space → Retropharyngeal space
Submandibular space → Parapharyngeal space → Retropharyngeal space
↓
Danger space (alar space)
↓
Posterior mediastinum (to diaphragm)
→ Descending necrotizing mediastinitis
- Lemierre's syndrome: Peritonsillar infection → parapharyngeal space → IJV thrombophlebitis → septic emboli to lungs
- Prevertebral space can be reached from retropharyngeal space if the alar fascia is breached, causing vertebral osteomyelitis
Imaging of Head and Neck Spaces
- CT with contrast is the investigation of choice for deep neck space infections - delineates abscess from cellulitis (rim enhancement + central low density = abscess)
- MRI is superior for soft tissue delineation and perineural spread, and for evaluating PPS tumors
- On CT: PPS appears as a low-density fat space; its displacement guides the origin of adjacent pathology
- Lateral neck X-ray: widened prevertebral shadow in retropharyngeal abscess
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.