Gimme breif details about bioelectricity mbbs 1st year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Guyton & Hall. Let me compile the full answer.
Bioelectricity - MBBS 1st Year Physiology
(Source: Guyton and Hall Textbook of Medical Physiology)
1. What is Bioelectricity?
Bioelectricity refers to the electrical potentials and currents that exist across cell membranes in excitable tissues (nerves, muscles). It arises from the unequal distribution of ions across the cell membrane, maintained by ion pumps and selective ion permeability.
2. Resting Membrane Potential (RMP)
The resting membrane potential of a large nerve fiber is -70 mV (inside negative relative to outside). The membrane is said to be polarized at rest.
How is it established?
a) Na⁺-K⁺ ATPase Pump (Electrogenic Pump)
- Pumps 3 Na⁺ out for every 2 K⁺ in - creating a net deficit of positive ions inside.
- This pump is the primary driver of the RMP.
Ion concentrations maintained:
| Ion | Outside (mEq/L) | Inside (mEq/L) |
|---|---|---|
| Na⁺ | 142 | 14 |
| K⁺ | 4 | 140 |
b) K⁺ Leak Channels
- The resting membrane is ~100x more permeable to K⁺ than Na⁺.
- K⁺ continuously leaks out down its concentration gradient, carrying positive charges out and making the inside more negative.
c) Large Intracellular Anions
- Large negatively charged proteins inside the cell cannot cross the membrane, contributing to the negative interior.
Nernst Equation is used to calculate the equilibrium potential for individual ions. The Goldman-Hodgkin-Katz equation accounts for multiple ions and gives a more accurate RMP.
3. Action Potential (AP)
An action potential is a rapid, transient reversal of membrane potential that propagates along the nerve fiber to transmit signals.
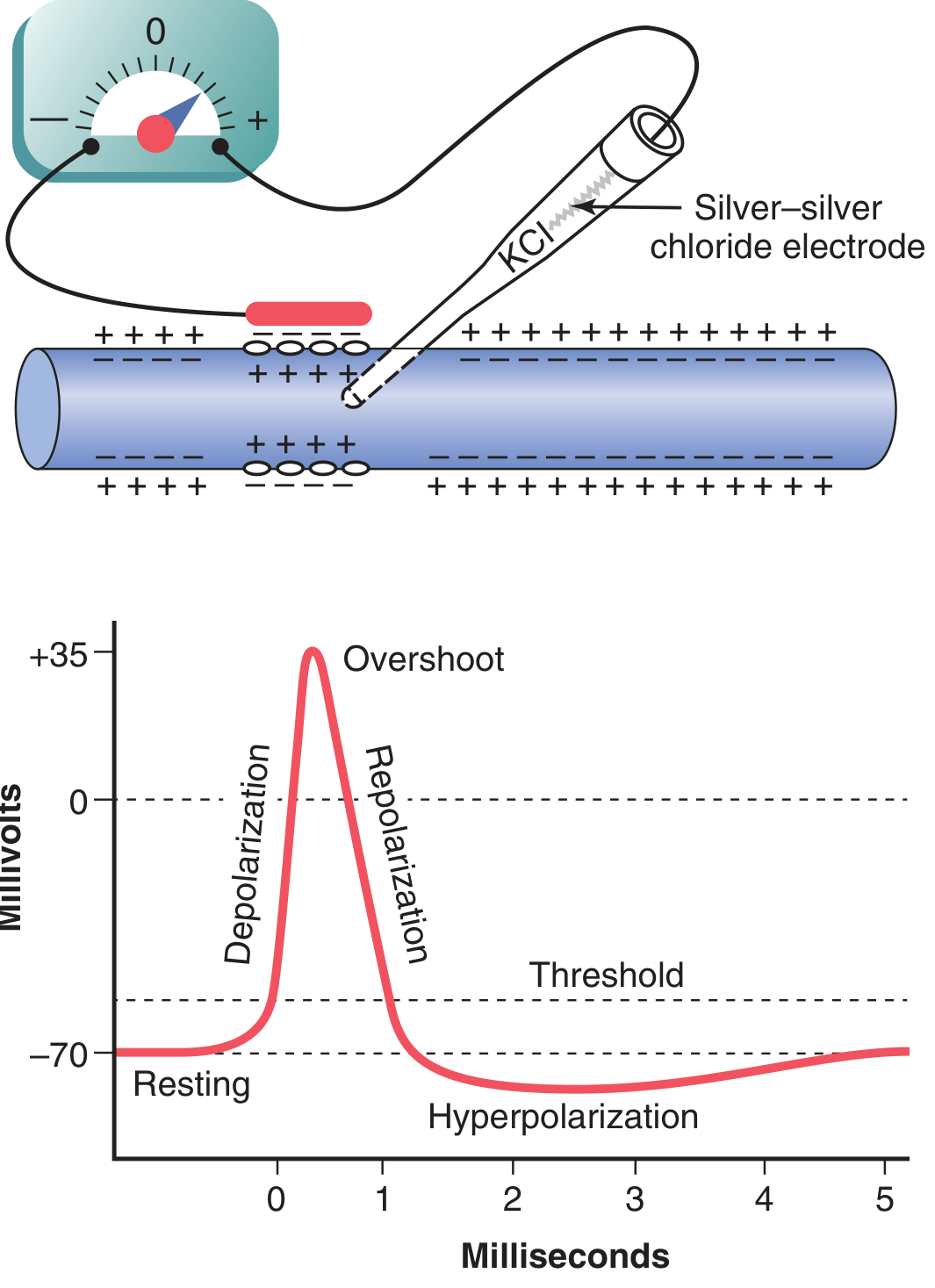
Phases of Action Potential:
a) Resting Stage (-70 mV)
- Membrane is polarized. No signal being transmitted.
b) Depolarization (Rising Phase)
- Stimulus depolarizes membrane to threshold (~-55 mV).
- Voltage-gated Na⁺ channels rapidly open → massive Na⁺ influx.
- Membrane potential shoots from -70 mV to +35 mV (overshoot).
c) Repolarization (Falling Phase)
- Na⁺ channels inactivate (close) within <1 ms.
- Voltage-gated K⁺ channels open (slower) → K⁺ rushes out.
- Membrane potential returns to -70 mV.
d) Hyperpolarization (Undershoot / After-Potential)
- K⁺ channels stay open slightly longer than needed.
- Membrane goes below -70 mV transiently (e.g., -75 to -80 mV).
- Returns to resting potential when K⁺ channels close.
Ion Channel Events Summary:
| Phase | Na⁺ Channel | K⁺ Channel | Membrane Potential |
|---|---|---|---|
| Resting | Closed | Closed | -70 mV |
| Depolarization | Open (activated) | Closed | -70 → +35 mV |
| Repolarization | Inactivated | Open | +35 → -70 mV |
| Hyperpolarization | Closed | Slowly closing | Below -70 mV |
Na⁺ conductance increases ~5000-fold at onset; K⁺ conductance increases only ~30-fold and more slowly.
4. Threshold and All-or-None Law
- A stimulus must depolarize the membrane to threshold (~-55 mV) to trigger an AP.
- Once threshold is reached, the AP is all-or-none - it fires at full amplitude regardless of stimulus strength.
- Subthreshold stimuli produce only local, graded potentials that fade away.
5. Refractory Periods
| Type | Mechanism | Significance |
|---|---|---|
| Absolute Refractory Period (ARP) | Na⁺ channels inactivated - cannot be reopened | No second AP possible, regardless of stimulus strength |
| Relative Refractory Period (RRP) | Na⁺ channels recovering; K⁺ channels still open (hyperpolarized) | AP possible only with a stronger-than-normal stimulus |
The refractory period limits the maximum frequency of nerve impulse transmission.
6. Propagation of Action Potential
- At the site of depolarization, local currents flow from the active (+ve inside) region to the adjacent resting (-ve inside) region.
- This depolarizes the adjacent membrane to threshold, triggering a new AP there.
- The AP thus travels along the fiber in one direction (the refractory period behind prevents backward conduction).
Saltatory Conduction (Myelinated Fibers)
- In myelinated nerves, the AP "jumps" from one node of Ranvier to the next.
- This is much faster and energy-efficient than continuous conduction in unmyelinated fibers.
- Conduction velocity: up to 120 m/s in large myelinated fibers vs. ~0.5 m/s in small unmyelinated C fibers.
7. Importance / Clinical Relevance
- Local anesthetics (e.g., lidocaine) block voltage-gated Na⁺ channels → prevent AP generation → pain relief.
- Cardiac arrhythmias involve abnormal membrane potentials in cardiac muscle.
- Nerve conduction studies (NCS) measure AP velocity to diagnose neuropathies.
- EEG / ECG / EMG all record bioelectric potentials from brain, heart, and muscle respectively.
Key Numbers to Remember:
| Parameter | Value |
|---|---|
| Resting Membrane Potential | -70 mV |
| Threshold | ~ -55 mV |
| Peak overshoot | +35 mV |
| Duration of AP (nerve) | ~1 ms |
- Guyton and Hall Textbook of Medical Physiology, Ch. 5
Brief me about all or none law
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Excellent content from multiple authoritative sources. Here is your brief:
All-or-None Law
Definition
The All-or-None Law states that an excitable cell (nerve fiber or muscle fiber) either responds to a stimulus with a full-amplitude action potential or does not respond at all. There is no partial or graded action potential - the response is either complete or absent.
"No action potential occurs if the stimulus is subthreshold in magnitude, and the action potential has a constant amplitude and form at any stimulus strength above the threshold intensity."
- Ganong's Review of Medical Physiology, 26th Ed.
The Core Concept: Threshold
- Every excitable membrane has a threshold potential (approximately -55 mV in nerve fibers).
- If a stimulus depolarizes the membrane to or beyond threshold → action potential fires fully.
- If the stimulus is subthreshold → no action potential; only a local, decaying electrotonic potential occurs.
| Stimulus Strength | Response |
|---|---|
| Below threshold | No AP - only graded electrotonic potential (decays with distance) |
| At threshold | AP fires (full amplitude) |
| Above threshold | AP fires - same amplitude, NOT bigger |
| During ARP | No AP, regardless of stimulus strength |
| During RRP | AP fires only with a stronger-than-normal stimulus |
Why is it "All-or-None"? - The Ionic Basis
Once threshold is reached, a positive feedback (regenerative) cycle takes over:
- Membrane depolarizes to threshold (-55 mV)
- Voltage-gated Na⁺ channels open → Na⁺ rushes in
- This further depolarizes the membrane → more Na⁺ channels open
- The process becomes self-sustaining and explosive - it cannot be "half-done"
- The AP always peaks at the same level (~+35 mV) because it is limited by the Na⁺ equilibrium potential
"The firing of an action potential is a binary, all-or-none event; that is, the spike has a constant, nongraded voltage peak that occurs only if the depolarizing stimulus exceeds the threshold."
- Medical Physiology (Boron & Boulpaep)
All-or-None vs. Graded Potentials
| Feature | Action Potential (All-or-None) | Graded Potential |
|---|---|---|
| Amplitude | Fixed, constant | Proportional to stimulus size |
| Propagation | Non-decremental (travels full distance) | Decremental (decays with distance) |
| Threshold | Required | Not required |
| Duration | Fixed (~1 ms) | Variable |
| Examples | Nerve impulse, muscle AP | Receptor potential, EPSP, IPSP |
Applies to Individual Fibers - Not Whole Nerves
A key point often asked in exams:
- The all-or-none law applies to a single nerve fiber or muscle fiber.
- A whole nerve trunk contains thousands of fibers with different thresholds, so a stronger stimulus recruits more fibers, giving a graded compound response - this is called recruitment or the size principle.
- This is why squeezing harder gives a stronger muscle contraction - more motor units are recruited, not bigger APs per fiber.
Exceptions / Where It Does NOT Apply
- Rods and cones of the retina: Their output signal is graded (hyperpolarizing), not all-or-none. The strength of the signal is proportional to light intensity. (Guyton & Hall)
- Receptor potentials (e.g., in mechanoreceptors): These are graded.
- Synaptic potentials (EPSPs/IPSPs): Graded responses.
- These graded signals eventually summate at the trigger zone (axon hillock) to decide whether to fire an all-or-none AP.
Clinical Significance
- Local anesthetics (lidocaine, bupivacaine): Block Na⁺ channels → prevent threshold from being reached → no AP → no pain signal.
- Cardiac muscle: Follows the all-or-none law per cell - the heart contracts fully or not at all (important in understanding arrhythmias).
- Nerve conduction studies: Measure the all-or-none AP response to assess nerve integrity.
Key Point to Remember for Exams:
- Stronger stimulus = more fibers recruited, NOT a bigger AP per fiber.
- The all-or-none law ensures reliable, consistent signal transmission over long distances without decay.
Sources: Ganong's Review of Medical Physiology 26th Ed. | Costanzo Physiology 7th Ed. | Medical Physiology (Boron & Boulpaep) | Guyton & Hall Textbook of Medical Physiology
Brief me about hla gene
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Excellent content gathered. Here is your comprehensive brief:
HLA (Human Leukocyte Antigen) Genes
1. What are HLA Genes?
HLA genes encode the Major Histocompatibility Complex (MHC) proteins in humans. They are responsible for presenting peptide antigens to T lymphocytes, allowing the immune system to distinguish self from non-self. The HLA system is the most polymorphic gene system in the entire human genome.
2. Chromosomal Location
- Located on the short arm of chromosome 6 (6p21.3)
- Spans approximately 4000 kilobases (kb) of DNA
- Contains over 224 identified gene loci
- Map order (distal → centromere): HLA-A → HLA-C → HLA-B → HLA-DR → HLA-DQ → HLA-DP
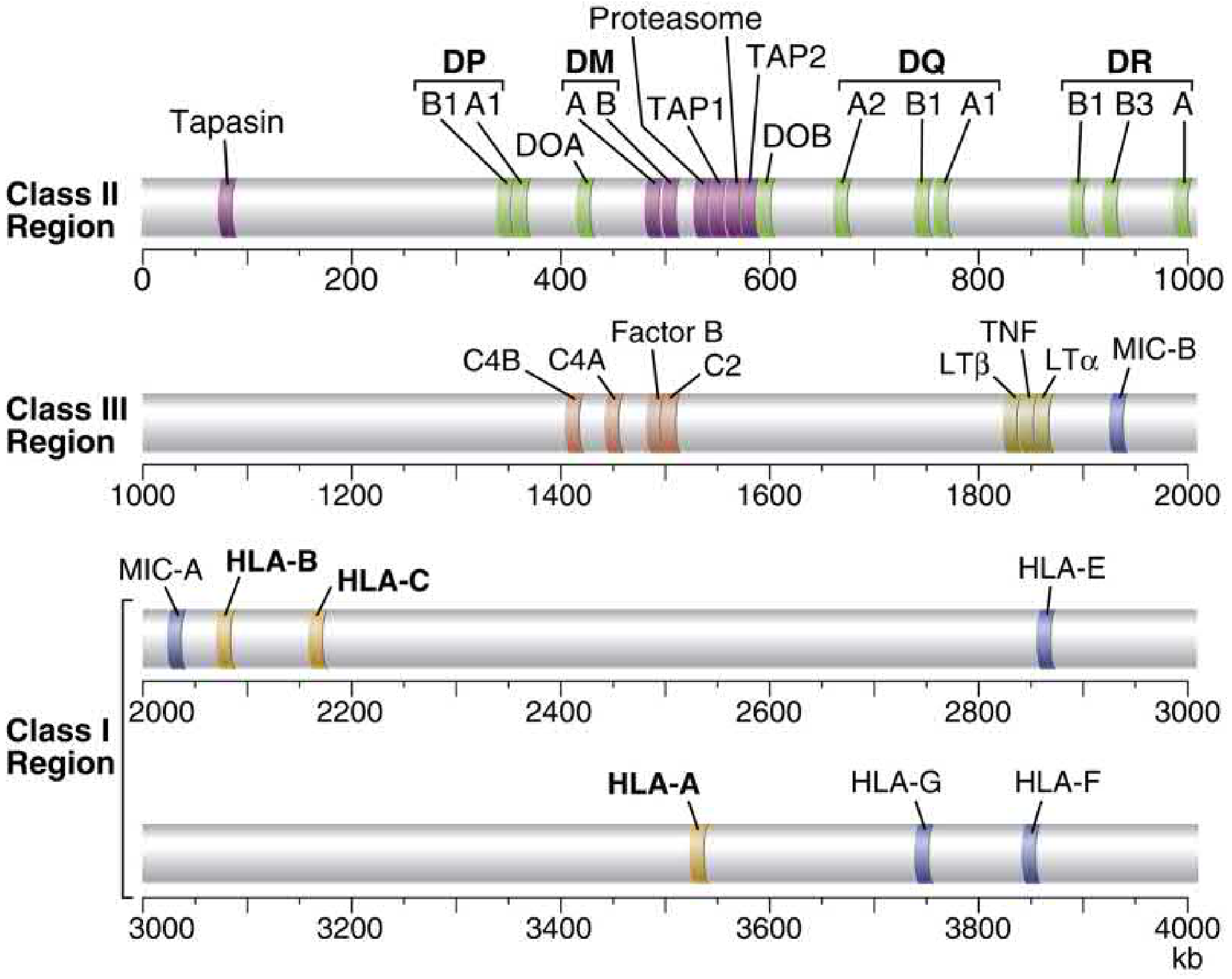
3. Classes of HLA Genes
Class I (HLA-A, HLA-B, HLA-C)
- Encode single α-chain proteins that pair with β2-microglobulin (encoded on chromosome 15)
- Present endogenous (intracellular) antigens - e.g., viral peptides, tumor antigens
- Expressed on virtually all nucleated cells
- Recognized by CD8+ cytotoxic T lymphocytes (CTLs)
Class II (HLA-DP, HLA-DQ, HLA-DR)
- Encode heterodimers (α + β chains) - each locus has separate A gene (α) and B gene (β)
- Present exogenous (extracellular) antigens - e.g., bacteria, phagocytosed microbes
- Expressed only on antigen-presenting cells (APCs): Dendritic cells, B lymphocytes, Macrophages, Thymic epithelial cells
- Recognized by CD4+ helper T lymphocytes
Class III
- Encoded between Class I and II regions
- Encode complement proteins: C2, C4A, C4B, Factor B
- Encode cytokines: TNF-α, Lymphotoxin-α (LTα), Lymphotoxin-β (LTβ)
- Also encode proteins involved in antigen processing: TAP1, TAP2, Tapasin, Proteasome subunits
| Feature | Class I | Class II | Class III |
|---|---|---|---|
| Genes | HLA-A, B, C | HLA-DP, DQ, DR | C2, C4, Factor B, TNF |
| Structure | α-chain + β2-microglobulin | α-chain + β-chain | Various |
| Expression | All nucleated cells | APCs only | Secreted |
| Presents to | CD8+ T cells | CD4+ T cells | - |
| Antigen type | Endogenous | Exogenous | - |
4. Non-Classical HLA Genes
- HLA-E, HLA-F, HLA-G: Class I-like molecules; important for NK cell regulation
- HLA-G: Expressed at the maternal-fetal interface; protects the fetus from maternal immune attack
- MIC-A, MIC-B: Stress-induced molecules; recognized by NK cells
5. Inheritance
- HLA genes are tightly linked - they segregate en bloc as a haplotype
- Each individual inherits one haplotype from each parent (two total)
- Alleles show codominant expression - both alleles are expressed
- Follow Mendelian inheritance - 4 possible combinations among siblings
- Probability of two siblings being HLA-identical = 25%
- Crossing over within the MHC occurs in ~4% of meioses
6. Polymorphism
- HLA genes are the most polymorphic in the human genome
- Hundreds to thousands of alleles exist at each locus
- Alleles are named systematically:
- e.g., HLA-A*0201 = HLA-A gene, allele group 02, subtype 01
- e.g., HLA-DRB1*0401 = DR beta-1 gene, allele 04, subtype 01
- This polymorphism ensures that populations can respond to a wide variety of pathogens
7. Linkage Disequilibrium
- Certain HLA alleles occur together on the same haplotype more frequently than expected by chance - this is called linkage disequilibrium (LD)
- Classic example: A1-Cw7-B8-DR17(3)-DQ2 haplotype in Caucasians - seen ~4x more often than expected
- Extends from HLA-A through HLA-DP
8. HLA and Disease Associations (High-Yield for Exams)
| Disease | HLA Association | Relative Risk |
|---|---|---|
| Ankylosing Spondylitis | HLA-B27 | >150x; 95% of AS patients are B27+ |
| Rheumatoid Arthritis | HLA-DR4 (DRB1*0401) | ~4x |
| Type 1 Diabetes Mellitus | HLA-DR3, DR4, DQ2, DQ8 | High |
| Celiac Disease | HLA-DQ2, DQ8 | Very high |
| Narcolepsy | HLA-DR2 (DQ1) | ~100x |
| Psoriasis | HLA-Cw6 | ~10x |
| Hemochromatosis | HLA-A3 (via linkage with HFE gene) | Due to LD, not direct |
| Goodpasture syndrome | HLA-DR2 | ~16x |
| Multiple Sclerosis | HLA-DR2 | ~4x |
| SLE | HLA-DR2, DR3 | ~3x |
Mechanism: HLA-B27 in ankylosing spondylitis causes heavy chain misfolding → inefficient antigen presentation → triggers autoimmune inflammation. (Thompson & Thompson Genetics, 9th Ed.)
9. HLA in Transplantation
- HLA matching between donor and recipient is critical for preventing graft rejection
- Standard matching involves at least 3 loci: HLA-A, HLA-B, HLA-DR
- Better HLA match → lower risk of rejection → longer graft survival
- Panel Reactive Antibody (PRA) test: measures pre-formed antibodies against ~80% of HLA antigens in the donor panel
- A crossmatch test is done before transplant to detect pre-formed donor-specific antibodies
10. HLA and Immune Function - Key Points
- MHC/HLA expression is upregulated by cytokines:
- Class I: increased by IFN-α, IFN-β, IFN-γ (especially during viral infection)
- Class II: increased by IFN-γ (e.g., during inflammatory states)
- This ensures that during an infection, more antigen is presented to T cells, amplifying the immune response
Summary Mnemonics:
- Class I = One chain = One cell (all nucleated) = CD8 (cytotoxic)
- Class II = Two chains = Two types of APCs = CD4 (helper)
- B27 = Back pain (Ankylosing Spondylitis)
- HLA-DR4 = RA (4 letters)
Sources: Cellular and Molecular Immunology (Abbas & Lichtman) | Henry's Clinical Diagnosis | Thompson & Thompson Genetics 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.