Explain me 10 heart diseases with their changes and explain images those changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
myocardial infarction gross pathology coagulative necrosis heart
Searching Images
dilated cardiomyopathy heart pathology gross specimen
Searching Images
hypertrophic cardiomyopathy asymmetric septal hypertrophy banana shaped ventricle
Searching Images
infective endocarditis vegetations mitral valve pathology
Searching Images
heart failure pulmonary edema congestion pathology
Searching Images
rheumatic heart disease mitral stenosis valve pathology
Searching Images
pericarditis fibrinous exudate bread butter pericardium
Searching Images
aortic stenosis calcified valve gross pathology
Searching Images
congenital heart disease ventricular septal defect tetralogy of Fallot
Searching Images
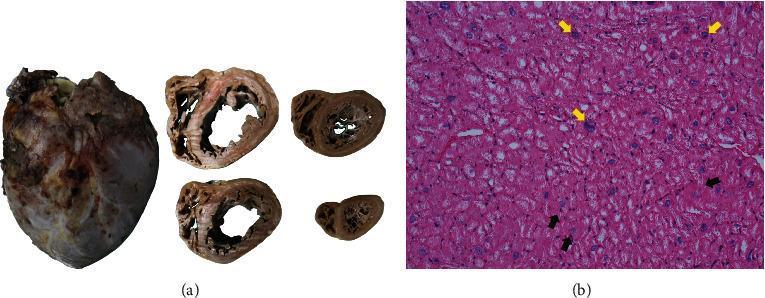
restrictive cardiomyopathy amyloidosis cardiac pathology
Reading File
I now have comprehensive content and images for all 10 diseases. Let me compile the full, well-illustrated answer.
10 Heart Diseases: Pathological Changes & Illustrated Guide
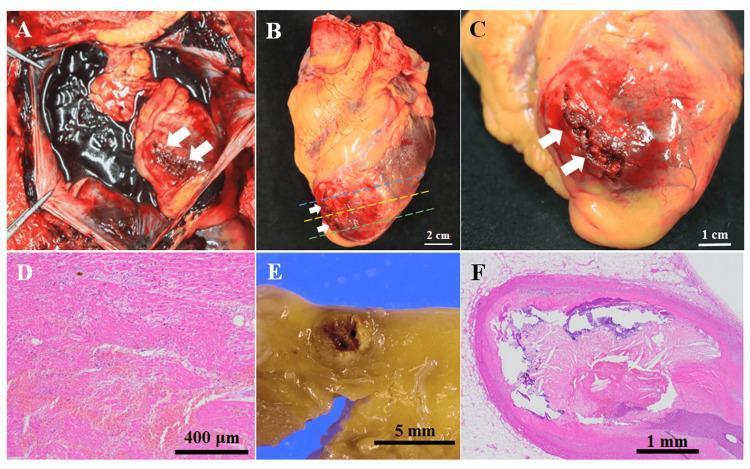
1. Myocardial Infarction (MI)
Definition: Necrosis of the heart muscle from ischemia, defined as acute myocardial injury with abnormal cardiac biomarkers plus evidence of acute myocardial ischemia.
Pathological Changes
- Mechanism: Atherosclerotic plaque rupture → platelet aggregation → thromboxane A2/ADP/serotonin release → coronary thrombosis → vessel occlusion
- Sequence: Within 20–40 minutes of sustained ischemia, irreversible coagulative necrosis begins in the subendocardial zone (most vulnerable, last to receive blood), then a "wavefront" of necrosis progresses outward over 3–6 hours
- Biochemical: Aerobic metabolism ceases within seconds → ATP drops → lactic acid accumulates → sarcolemmal membrane disruption → release of troponins, CK-MB into bloodstream
- Gross changes by time:
- 0–6 h: No gross change (only microscopic)
- 6–24 h: Dark mottling, pale area
- 1–3 days: Yellow-tan, softening
- 1–2 weeks: Hyperemic border, yellow-grey centre
- 4–8 weeks: White scar (collagen replacement)
- Coronary territories: LAD occlusion (40–50%) → anterior LV, anterior 2/3 septum; RCA (30–40%) → inferior/posterior LV; LCX (15–20%) → lateral LV
Complications: Arrhythmia (ventricular fibrillation in 80–90% of cardiac deaths), cardiac rupture, mural thrombus, cardiogenic shock, pericarditis, aneurysm.
Images
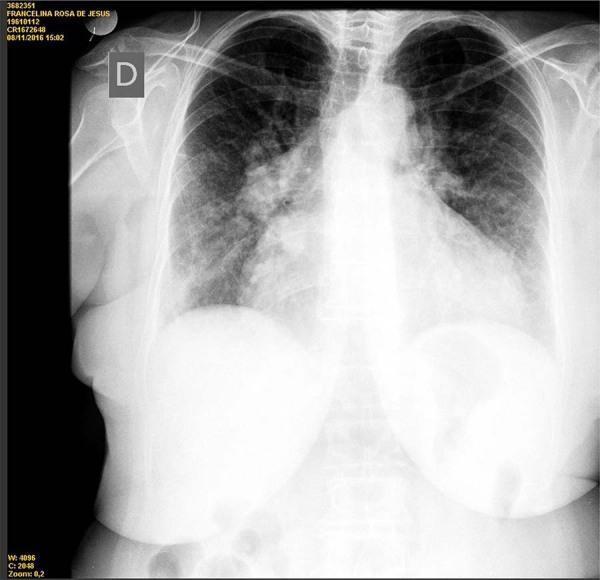
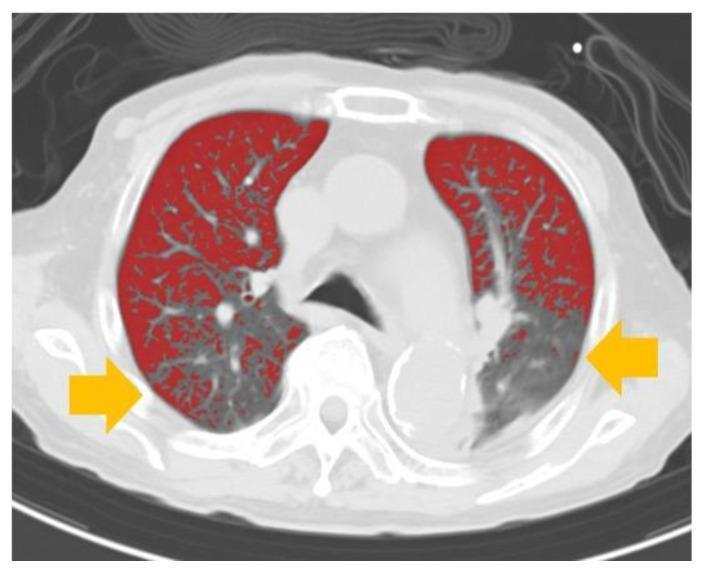
2. Heart Failure (Congestive Heart Failure)
Definition: Inability of the heart to pump sufficient blood to meet metabolic demands; classified as HFrEF (reduced EF, systolic) or HFpEF (preserved EF, diastolic).
Pathological Changes
- Left heart failure: Pulmonary venous hypertension → pulmonary edema → "nutmeg lung" (congestive hemosiderosis, "heart failure cells" = hemosiderin-laden macrophages in alveoli)
- Right heart failure (or biventricular): Systemic venous congestion → hepatomegaly (nutmeg liver), peripheral edema, ascites, splenomegaly
- Cardiac remodeling: Myocyte hypertrophy, interstitial fibrosis, ventricular dilation; increased wall stress activates neurohormonal pathways (RAAS, sympathetic nervous system, BNP)
- Compensatory mechanisms (that ultimately worsen failure): Frank–Starling mechanism, neurohormonal activation, ventricular hypertrophy/remodeling
- BNP/NT-proBNP: Released due to ventricular wall stress; key diagnostic biomarker
Images
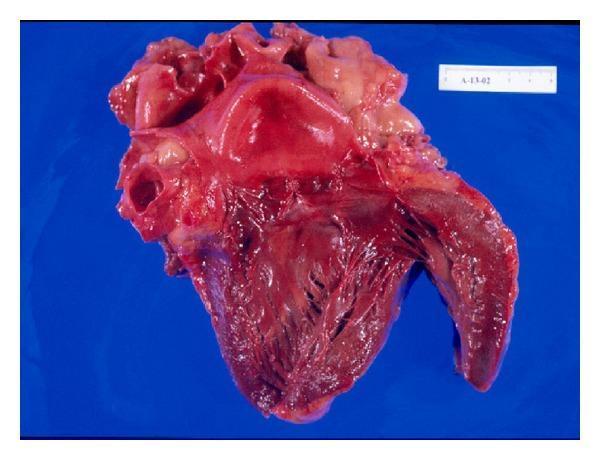
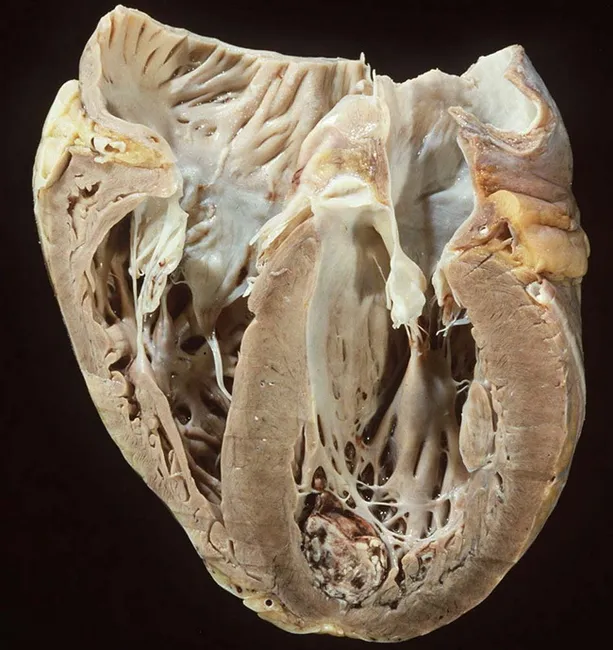
3. Dilated Cardiomyopathy (DCM)
Definition: Progressive cardiac dilation with contractile (systolic) dysfunction (EF < 40%), usually with concurrent hypertrophy.
Pathological Changes
- Causes: Genetic (20–50%; titin mutations most common, also β-myosin heavy chain, troponin T, dystrophin); viral myocarditis (coxsackievirus B, parvovirus B19); alcohol/toxins (acetaldehyde direct myocardial toxin); peripartum; hemochromatosis; sarcoidosis; doxorubicin
- Gross: Four-chamber dilation and hypertrophy; flabby, poorly contractile walls; mural thrombus at apex of LV (risk of systemic embolism)
- Microscopy: Myocyte hypertrophy (enlarged nuclei) + interstitial fibrosis (collagen blue on Masson trichrome); vacuolar degeneration; no specific cause identifiable in end-stage
- Mechanism of failure: Loss-of-function mutations in cytoskeletal/sarcomeric proteins → impaired contractility → systolic dysfunction → progressive dilation → further pump failure
Images
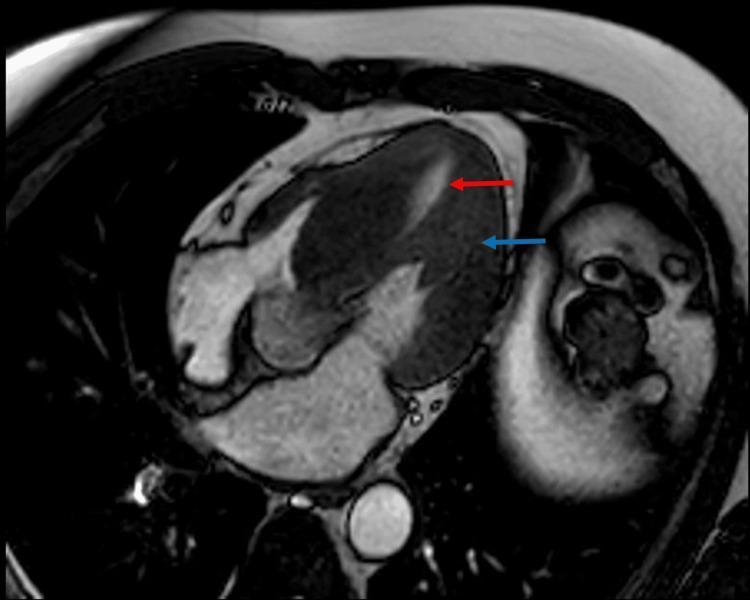
4. Hypertrophic Cardiomyopathy (HCM)
Definition: Myocardial hypertrophy with defective diastolic filling and — in 1/3 of cases — ventricular outflow obstruction; thick-walled, heavy, hypercontractile heart.
Pathological Changes
- Genetics: Autosomal dominant; gain-of-function mutations in sarcomeric proteins: β-myosin heavy chain (most common), myosin-binding protein C, troponin T → account for 70–80% of all HCM
- Pathophysiology: Hypercontractility → increased energy consumption → negative energy balance → myocyte disarray and replacement fibrosis → diastolic dysfunction (impaired relaxation/compliance)
- Gross: Massive hypertrophy without dilation; asymmetric septal hypertrophy in 90% (septal > free wall); ventricular cavity compressed into "banana-like" shape; anterior mitral leaflet contacts septum during systole → left ventricular outflow tract (LVOT) obstruction (SAM - systolic anterior motion)
- Microscopy: Myocyte disarray (whorled pattern), hypertrophied myocytes, interstitial fibrosis
- Risk: #1 cause of sudden cardiac death in young athletes
Images

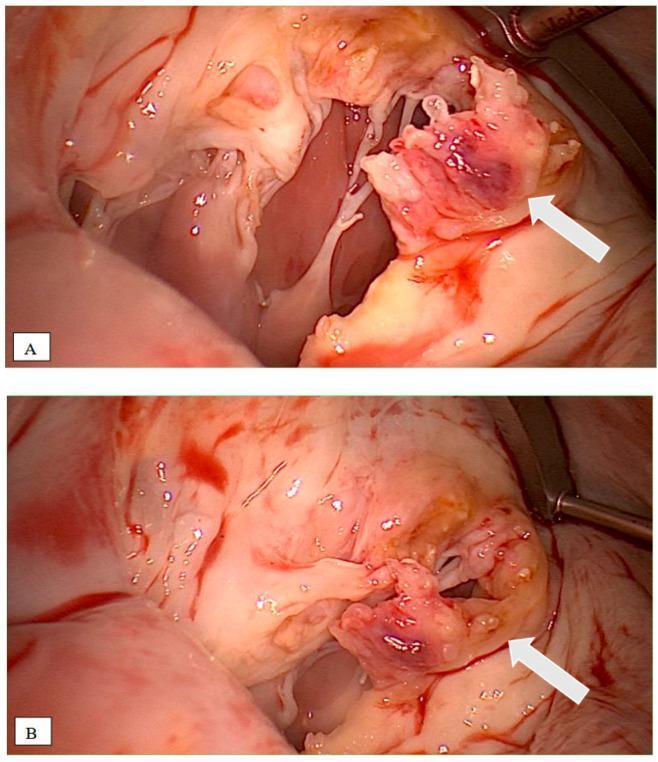
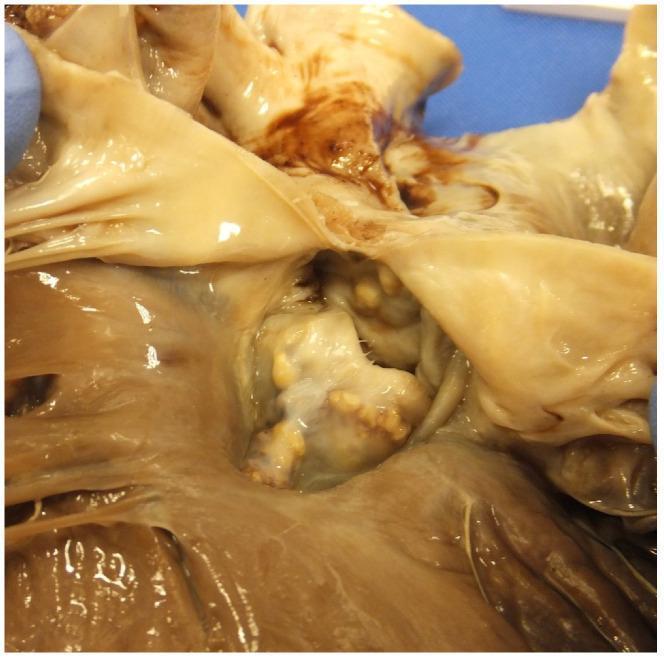
5. Infective Endocarditis (IE)
Definition: Infection of the cardiac endocardium, typically affecting valve leaflets, causing destructive vegetations.
Pathological Changes
- Microbiology: Acute IE (rapid destruction): Staphylococcus aureus; Subacute IE (smoldering): viridans streptococci; HACEK organisms; fungi (Candida) in IV drug users/prosthetic valves
- Pathogenesis: Bacteremia → seeding of endothelium (especially abnormal/damaged valves) → platelet-fibrin-bacteria aggregates form vegetations
- Vegetations: Friable, irregular, cauliflower-like masses on valve leaflets (usually on mitral and aortic valves, left-sided); contain bacteria, fibrin, inflammatory cells, necrotic tissue
- Gross: Large, bulky, destructive vegetations; leaflet ulceration/perforation; chordae tendineae involvement; valve insufficiency
- Systemic effects (emboli): Osler nodes (fingertip tender nodules), Janeway lesions (painless palm/sole hemorrhages), Roth spots (retinal), splenic/renal infarcts, stroke (septic emboli)
- Duke Criteria: Used for diagnosis (major: positive blood cultures, echocardiographic evidence; minor: fever, predisposing condition, vascular/embolic phenomena)
Images

6. Rheumatic Heart Disease
Definition: Late valvular complication of acute rheumatic fever (immune response to Group A streptococcal pharyngitis, mediated by molecular mimicry against cardiac antigens).
Pathological Changes
- Acute phase (rheumatic carditis): Pancarditis (all layers); Aschoff bodies (pathognomonic) — granulomatous foci with Anitschkow cells (caterpillar cells = activated macrophages with characteristic chromatin pattern); MacCallum plaques on posterior LA wall
- Valves: Sterile vegetations (verrucae) along valve closure lines during acute phase; subsequent fibrosis and scarring
- Chronic/late changes:
- Mitral stenosis (most common, 70%): leaflet thickening, commissural fusion → "fish-mouth" or "buttonhole" orifice; chordal shortening/fusion; calcification
- Mitral valve area reduced from normal 4–6 cm² to < 1 cm² in severe stenosis
- Left atrial dilation → atrial fibrillation → mural thrombus → systemic embolism
- Other valves: aortic > tricuspid > pulmonary (in decreasing frequency)
- Microscopy: Fibrosis, neovascularization, calcification of leaflets
Images

7. Pericarditis
Definition: Inflammation of the pericardium (serous sac surrounding the heart), most commonly idiopathic/viral.
Pathological Changes
- Causes: Viral (coxsackievirus A/B, echovirus, EBV, CMV, HIV); bacterial (TB — constrictive); post-MI (Dressler syndrome); uremia; autoimmune (SLE, RA); neoplastic; post-radiation
- Types by exudate:
- Fibrinous (most common): Fibrin deposition on pericardial surfaces → "bread and butter" appearance on gross inspection (shaggy, yellow-white, irregular surface replacing normal smooth glistening serosal surface)
- Serous: Clear fluid (viral, autoimmune)
- Serofibrinous/hemorrhagic: TB, malignancy
- Purulent: Bacterial (Staphylococci, gram-negatives)
- Pericardial effusion: Accumulation of fluid; if rapid → cardiac tamponade (Beck's triad: hypotension, raised JVP, muffled heart sounds)
- Constrictive pericarditis: Fibrosis + calcification → rigid pericardium → impaired cardiac filling → diastolic dysfunction; "pericardial knock," Kussmaul's sign
- ECG: Saddle-shaped diffuse ST elevation + PR depression (pathognomonic)
Images
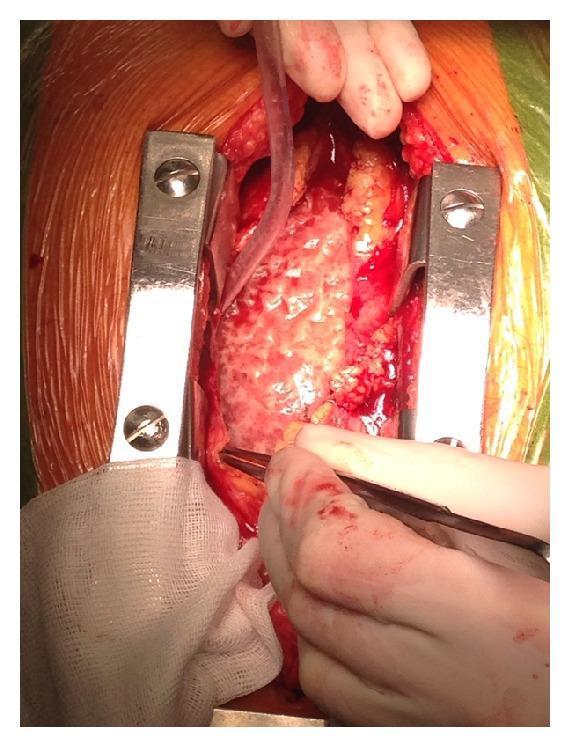

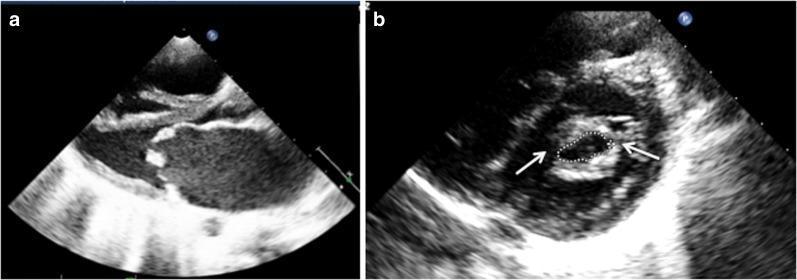
8. Aortic Stenosis (AS)
Definition: Obstruction of LV outflow due to narrowing of the aortic valve orifice; most common valvular heart disease in developed countries.
Pathological Changes
- Causes by age:
- Young < 60 y: Congenital bicuspid aortic valve (1–2% population) → accelerated calcification
- Elderly > 65 y: Calcific (senile/degenerative) AS — most common; active process similar to atherosclerosis (lipid deposition, inflammation, calcification)
- Any age (less common now): Rheumatic (usually combined MS + AS)
- Pathophysiology: Valve orifice narrows (normal 3–4 cm²; severe < 1 cm²) → LV pressure overload → concentric LV hypertrophy (wall thickness increases to normalize wall stress) → diastolic dysfunction → eventually systolic dysfunction and cardiac decompensation
- Gross: Thickened, irregular, heavily calcified leaflets; nodular calcium deposits; fused commissures (rheumatic) vs. calcified but mobile cusps (degenerative)
- Classic symptom triad (SAD): Syncope, Angina, Dyspnea — with each symptom, prognosis worsens (2–5 years if untreated once symptoms appear)
- Auscultation: Harsh systolic ejection murmur at RUSB radiating to carotids; paradoxical splitting of S2; slow-rising pulse (pulsus parvus et tardus)
Images

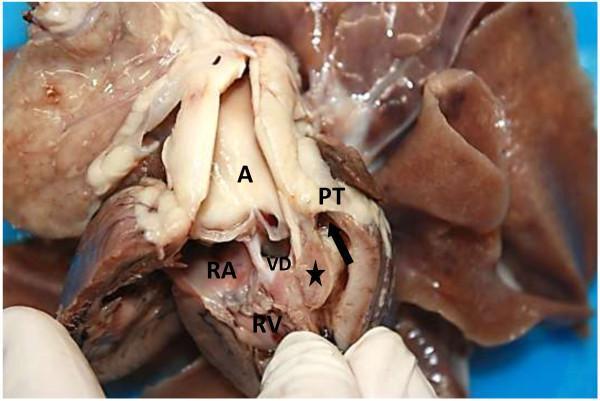
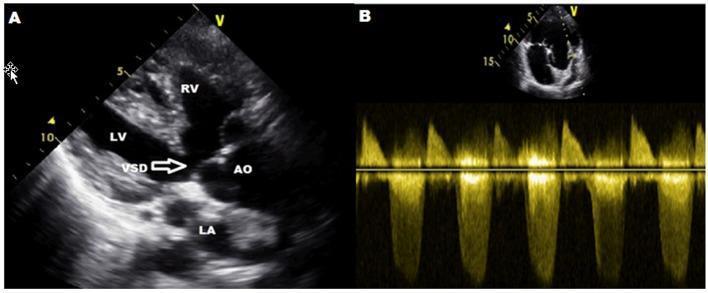
9. Congenital Heart Disease — Tetralogy of Fallot (TOF)
Definition: Most common cyanotic congenital heart defect; comprises four anatomical abnormalities arising from a single developmental defect (anterosuperior displacement of the infundibular septum).
The Four Components
- Ventricular Septal Defect (VSD) — large perimembranous defect
- Pulmonary stenosis/infundibular stenosis — RVOT obstruction
- Overriding aorta — aortic root displaced rightward over VSD
- Right ventricular hypertrophy (RVH) — secondary to outflow obstruction
Pathological Changes
- Embryology: Abnormal rotation/migration of conotruncal septum → malalignment of great vessels
- Hemodynamics: RVOT obstruction → RV pressure rises → right-to-left shunting through VSD → deoxygenated blood enters systemic circulation → central cyanosis ("blue baby")
- Degree of shunt: Depends on severity of RVOT obstruction; mild (pink TOF = left-to-right shunt) vs. severe (marked cyanosis)
- "Tet spells": Episodes of sudden hypercyanosis from muscular RVOT spasm; treated by knee-chest position (increases SVR) or morphine/propranolol
- Polycythemia: Compensatory; risk of cerebral thrombosis and abscess
- Gross: RV hypertrophy, hypoplastic pulmonary trunk, overriding aorta, large perimembranous VSD
- Treatment: Complete surgical repair (VSD patch + RVOT reconstruction)
Images
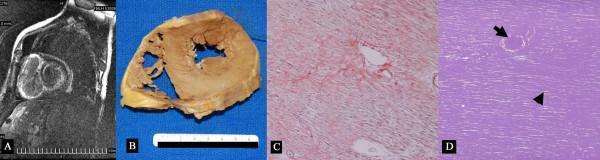
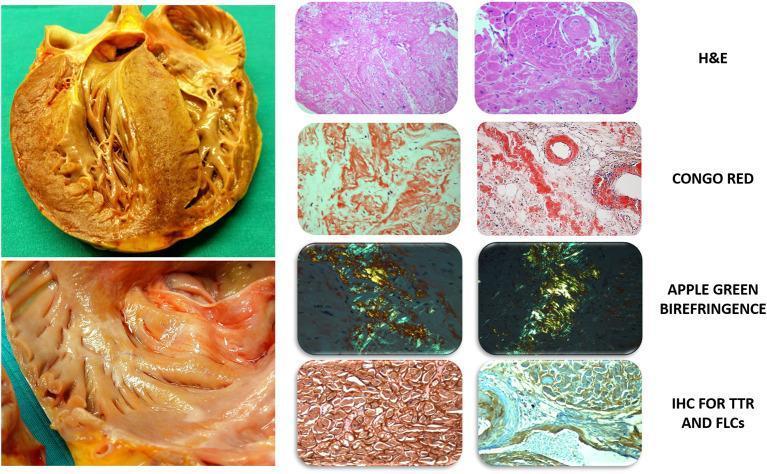
10. Restrictive Cardiomyopathy (Cardiac Amyloidosis)
Definition: Stiffened, non-compliant ventricles with markedly impaired diastolic filling but relatively preserved systolic function; most common causes are amyloidosis, radiation fibrosis, sarcoidosis.
Pathological Changes (Cardiac Amyloidosis as Paradigm)
- Types: AL amyloidosis (immunoglobulin light chains, plasma cell dyscrasias/multiple myeloma) and ATTR amyloidosis (transthyretin; wild-type = senile, or hereditary TTR mutations)
- Gross: Concentric LV and RV wall thickening (hypertrophy); waxy, pale yellowish appearance; nodular deposits on endocardium; biatrial enlargement; thickened interatrial septum; thickened AV valves
- Microscopy:
- H&E: Pale pink amorphous material infiltrating myocardial interstitium between myocytes
- Congo red stain: Salmon-pink deposits → diagnostic
- Polarized light: Pathognomonic apple-green birefringence
- Immunohistochemistry: TTR-positive (ATTR) vs. κ/λ light chain (AL)
- Cardiac MRI: Diffuse subendocardial late gadolinium enhancement (LGE) with base-to-apex gradient; "inability to null" the myocardium; biventricular wall thickening; atrial dilation
- ECG paradox: Despite massive hypertrophy, shows low-voltage QRS (amyloid replaces conducting myocardium) + pseudo-infarct pattern
- Echo: Restrictive filling (E/A > 2, short deceleration time); "sparkling" granular myocardium on older echo; tissue Doppler shows severe diastolic dysfunction
Images
Summary Table
| # | Disease | Primary Change | Key Gross Finding | Key Micro Finding |
|---|---|---|---|---|
| 1 | Myocardial Infarction | Coagulative necrosis | Pale → yellow → white scar | Loss of nuclei, neutrophil infiltrate → fibrosis |
| 2 | Heart Failure | Remodeling + congestion | Four-chamber dilation, nutmeg lung/liver | Myocyte hypertrophy, fibrosis; hemosiderin macrophages |
| 3 | Dilated Cardiomyopathy | Systolic dysfunction | Flabby, dilated all 4 chambers, apical thrombus | Hypertrophy, vacuolar degeneration, interstitial fibrosis |
| 4 | Hypertrophic Cardiomyopathy | Diastolic dysfunction | Asymmetric septal hypertrophy, banana-shaped LV | Myocyte disarray, interstitial fibrosis |
| 5 | Infective Endocarditis | Valve destruction | Friable, bulky vegetations on leaflets | Bacteria + fibrin + necrosis in vegetations |
| 6 | Rheumatic Heart Disease | Immune-mediated valve fibrosis | Fish-mouth mitral stenosis, commissural fusion | Aschoff bodies, Anitschkow cells |
| 7 | Pericarditis | Pericardial inflammation | "Bread and butter" fibrinous exudate | Fibrin + inflammatory cells |
| 8 | Aortic Stenosis | LV pressure overload | Calcified, thickened aortic valve leaflets | Concentric LV hypertrophy |
| 9 | Tetralogy of Fallot | R→L shunt, RVOT obstruction | VSD, overriding aorta, RVH, small PA | Malalignment VSD, muscular RV hypertrophy |
| 10 | Restrictive Cardiomyopathy (Amyloid) | Diastolic dysfunction | Waxy, stiff, hypertrophied ventricles | Congo red positivity, apple-green birefringence |
Sources: Robbins & Kumar Basic Pathology (9780323790185); Braunwald's Heart Disease (9780323722193); Goldman-Cecil Medicine (9780323930345); Textbook of Family Medicine (9780323239905)
This is a shared conversation. Sign in to Orris to start your own chat.