Ibd from Robbins long question answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive long Q&A. Let me compile it.
Inflammatory Bowel Disease (IBD) - Long Question & Answer
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Q1. Define IBD. What are its two major subtypes and how do they differ fundamentally?
Answer:
Inflammatory bowel disease (IBD) is a chronic inflammatory condition triggered by the host immune response to intestinal microbiota in genetically predisposed individuals. It encompasses two distinct entities:
- Ulcerative Colitis (UC) - limited to the colon and rectum, involving only the mucosa and submucosa.
- Crohn Disease (CD) - may involve any part of the GI tract (from mouth to anus) and typically produces transmural inflammation.
The distinction between the two is based primarily on:
- Distribution of affected sites
- Morphologic expression of disease at those sites
(Robbins & Kumar Basic Pathology, p. 576; Robbins Pathologic Basis of Disease, p. 744)
Q2. Describe the epidemiology of IBD.
Answer:
- Both UC and Crohn disease most frequently present in adolescents and young adults (teenage years to early 20s), but can develop at any age.
- IBD is most common among people of European descent, and in the United States occurs 3-5 times more often in eastern European (Ashkenazi) Jewish people.
- Most common in North America, northern Europe, and Australia.
- Incidence is rising in Africa, South America, and Asia, where prevalence was historically low.
Hygiene Hypothesis: The increasing incidence may be related to improved hygiene, leading to:
- Improved food storage and decreased food contamination
- Changes in gut microbiome composition
- Inadequate development of regulatory immune processes that limit mucosal immune responses
- This allows mucosa-associated microbes to trigger persistent chronic inflammation in susceptible hosts.
Other proposed factors include preservatives and materials in processed foods that may induce low-grade mucosal damage.
(Robbins Pathologic Basis of Disease, p. 744)
Q3. Explain the pathogenesis of IBD in detail.
Answer:
IBD results from a combination of:
- Genetic susceptibility
- Abnormal mucosal immune responses
- Host-microbiome interactions
- Epithelial barrier dysfunction
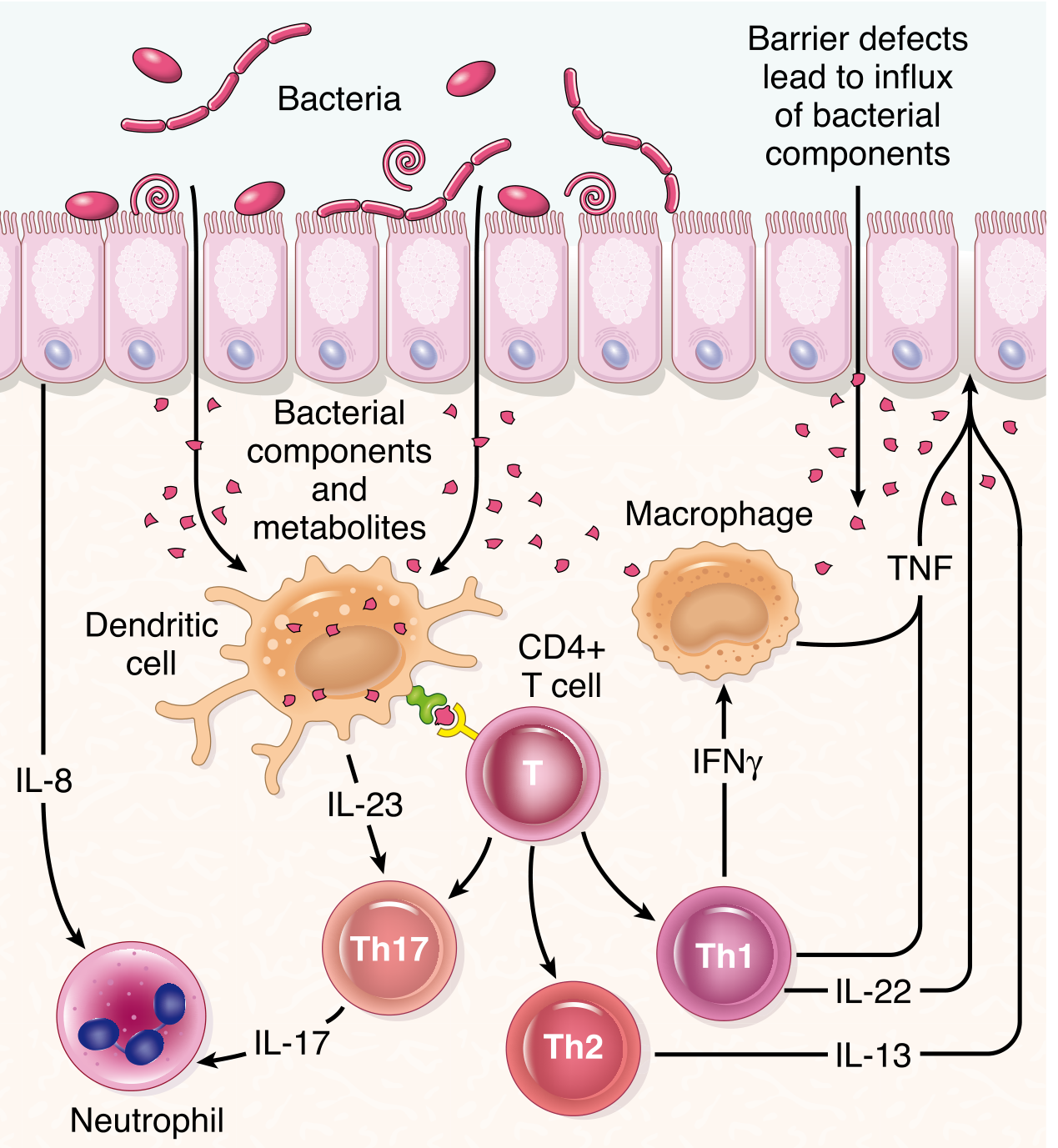
Fig. 17.36 - Pathogenesis of IBD showing bacterial components interacting with dendritic cells, CD4+ T cells, macrophages, and neutrophils via IL-23, IL-17, IL-13, IFN-γ, and TNF.
A. Genetic Factors
- Over 200 IBD-associated risk alleles have been identified; they account for less than 20% of disease risk in Crohn disease.
- NOD2 gene (nucleotide oligomerization binding domain 2):
- Most strongly associated with Crohn disease in European populations
- Encodes an intracellular sensor of muramyl dipeptide (a bacterial cell wall component)
- Disease-associated NOD2 variants are ineffective at defending against intestinal bacteria, allowing bacteria to penetrate the epithelium and trigger inflammatory reactions
- Three major NOD2 risk alleles present in only ~30% of CD patients vs. 5% of healthy individuals
- NOD2 variants are rare in Asian populations - so other factors are important
- NOD2 and PTPN22 variants: increase Crohn risk but are protective in ulcerative colitis
- Concordance rates: Monozygotic twins - ~50% for CD, ~20% for UC (genetic factors less dominant in UC)
- Additional IBD-associated genes involve autophagy-related pathways - involved in host cell responses to intracellular bacteria.
B. Abnormal Mucosal Immune Responses
- Microbial antigens are presented to CD4+ helper T cells, inducing differentiation into Th1 and Th17 cells (driven by IL-12 and IL-23).
- These activate macrophages, recruit neutrophils, and release proinflammatory cytokines (especially TNF).
- Defects in regulatory T cells (especially IL-10-producing subset) may fail to dampen the immune response - individuals with mutations in IL-10 or IL-10 receptor genes develop severe early-onset colitis.
- IL-13 (Th2 cytokine): mucosal production is increased in UC and, to a lesser degree, in CD.
- Effective treatments with anti-TNF antibodies and anti-IL-12/IL-23 antibodies support the role of these cytokines.
C. Intestinal Microbiota
- The intestinal lumen contains the largest reservoir of potential antigens in the body.
- IBD is rare in germ-free animal models.
- Probiotic bacteria can be beneficial in IBD treatment.
- Dysbiosis - altered microbial composition is seen in IBD:
- Decrease in protective species such as Faecalibacterium prausnitzii (produces butyrate)
- Increase in mucosal-adherent/invasive bacteria
- It remains unclear if microbial changes are a cause or consequence of IBD.
D. Epithelial Defects
- Normally, intestinal epithelium forms a barrier that limits contact between luminal microbes and the mucosal immune system.
- ATG16L1 and IRGM (autophagy genes): IBD-associated polymorphisms affect autophagy in Paneth cells, impairing their antibacterial secretory function.
- IBD-associated barrier defects allow bacterial components to enter the lamina propria, triggering and sustaining the inflammatory cascade.
(Robbins & Kumar Basic Pathology, pp. 577-578; Robbins Pathologic Basis of Disease, pp. 744-747)
Q4. Compare and contrast the gross and microscopic morphology of Crohn disease and Ulcerative Colitis.
Answer:
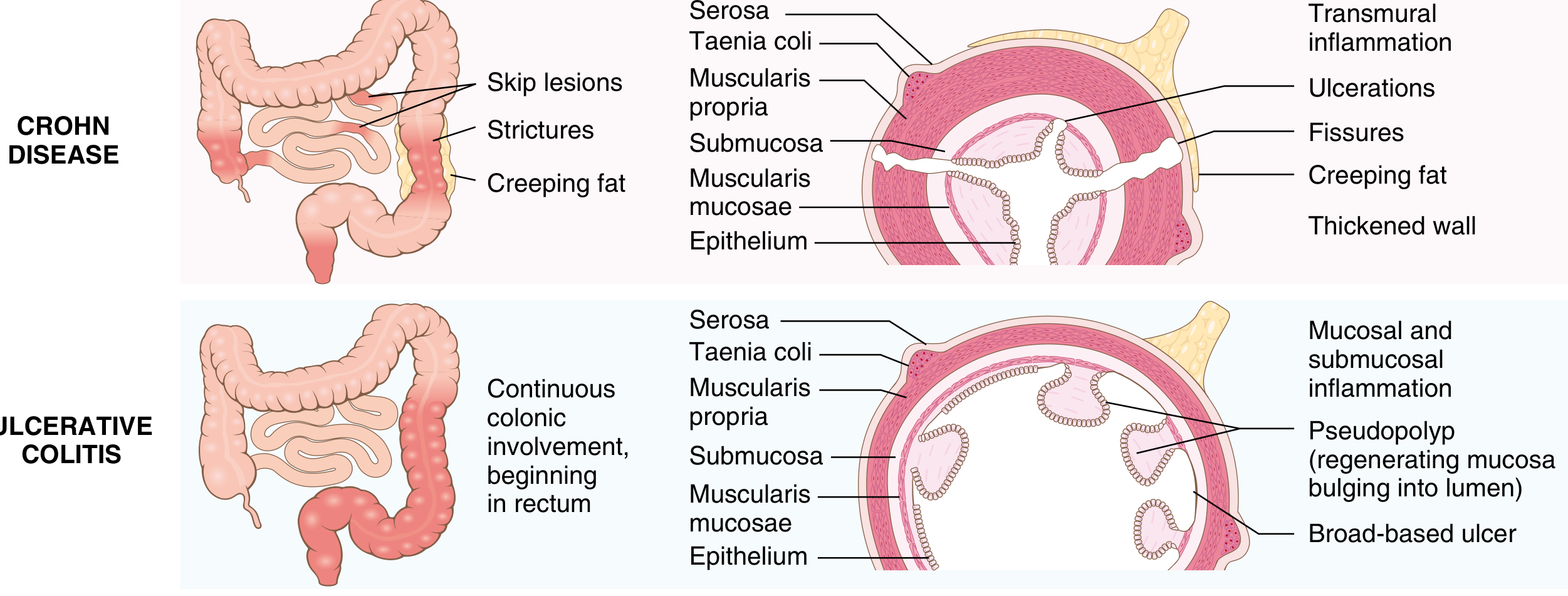
Fig. 17.35 - Distribution and cross-sectional morphology of Crohn disease vs. Ulcerative Colitis.
Comparison Table (Table 17.8 / Table 13.5 from Robbins):
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Bowel region | Ileum ± colon | Colon only |
| Rectal involvement | Sometimes | Always |
| Distribution | Skip lesions | Diffuse/continuous |
| Stricture | Yes | Rare |
| Bowel wall | Thick (transmural) | Normal/thin |
| Inflammation | Transmural | Limited to mucosa & submucosa |
| Pseudopolyps | Moderate | Marked |
| Ulcers | Deep, knife-like | Superficial, broad-based |
| Lymphoid reaction | Marked | Moderate |
| Fibrosis | Marked | Mild to none |
| Serositis | Marked | Mild to none |
| Granulomas | Yes (~35%) | No |
| Fistulae/sinuses | Yes | No |
| Perianal fistula | Yes (in colonic disease) | No |
| Fat malabsorption | Yes | No |
| Malignant potential | Yes | Yes |
| Recurrence after surgery | Common | No (curative) |
| Toxic megacolon | No | Yes |
Crohn Disease - Morphology
Gross:
- Any part of GI tract affected; most commonly terminal ileum (ileocecal region in ~40-60% of cases)
- "Skip lesions" - alternating areas of disease and normal bowel separated by areas of normal mucosa ("skip areas")
- Cobblestone appearance - mucosal islands lift between deep ulcers and submucosal edema
- Deep, knife-like ulcers (fissures) that can penetrate the entire bowel wall
- Strictures - from transmural fibrosis; cause obstruction ("string sign" on barium)
- Creeping fat (fat wrapping) - mesothelial fat extends over the bowel surface
- Thick, rubbery bowel wall due to transmural edema and fibrosis
- Fistulas and sinuses - deep fissures may form internal fistulae (enterovesical, enterocutaneous, rectovaginal) or abscesses
Microscopic:
- Transmural inflammation with lymphoid aggregates through all layers
- Non-caseating granulomas (~35% of cases) - a hallmark; can be present in all layers including lymph nodes and distant organs
- Crypt abscesses and crypt distortion
- Haphazard crypt organization from repeated injury and regeneration
- Active disease shows ulceration with purulent exudate
- Submucosal and serosal granulomas
Ulcerative Colitis - Morphology
Gross:
- Always involves the rectum and extends proximally in a continuous (non-skip) fashion
- Pancolitis = disease of entire colon; left-sided UC, ulcerative proctitis, proctosigmoiditis based on extent
- Small intestine not affected - may have backwash ileitis (mild distal ileal inflammation in severe pancolitis)
- Focal appendiceal or cecal inflammation ("cecal red spot") may be present in left-sided UC
- Mucosa: ranges from slightly red and granular to extensive, broad-based ulcers
- Pseudopolyps (inflammatory polyps) - isolated islands of regenerating mucosa bulging into lumen; tips may fuse to form mucosal bridges
- No skip lesions, no thickening of wall, no strictures, serosal surface normal
- Chronic disease: mucosal atrophy with smooth surface, loss of normal folds
Microscopic:
- Mucosal and submucosal inflammation only (not transmural)
- Crypt abscesses (neutrophils within crypt lumens)
- Crypt distortion
- Pseudopyloric metaplasia and Paneth cell metaplasia in chronic disease
- No granulomas (a key distinguishing feature from Crohn disease)
- Basal plasmacytosis and increased lamina propria cellularity
(Robbins Pathologic Basis of Disease, pp. 747-752)
Q5. What are the clinical features of Crohn Disease and Ulcerative Colitis?
Answer:
Crohn Disease - Clinical Features
- Intermittent bouts of diarrhea, fever, and abdominal pain separated by asymptomatic intervals
- Abdominal right lower quadrant pain and tenderness (due to terminal ileal involvement)
- Malabsorption - fat and fat-soluble vitamins (A, D, E, K), vitamin B12 (terminal ileum)
- Weight loss, anemia, hypoproteinemia
- Fistulas and abscesses
- Perianal disease - fistulas, skin tags, abscesses
- Strictures leading to bowel obstruction
- Up to 75% have disease recurrence after surgical resection
Ulcerative Colitis - Clinical Features
- Bloody diarrhea - most common presenting symptom
- Colicky abdominal pain relieved by defecation
- Tenesmus (rectal urgency)
- Disease follows a relapsing and remitting course
- Factors triggering onset: smoking cessation can precede or worsen UC; some cases follow infectious enteritis
- Smoking is actually partially protective in UC (opposite of Crohn disease)
- p-ANCA (perinuclear antineutrophil cytoplasmic antibodies): present in up to 75% of UC patients, only ~10% of Crohn patients - a useful serology
- ASCA (anti-Saccharomyces cerevisiae antibodies): more common in Crohn disease
Q6. What are the extraintestinal (systemic) manifestations of IBD?
Answer:
Extraintestinal manifestations overlap between UC and Crohn disease and include:
| System | Manifestation |
|---|---|
| Joints | Migratory polyarthritis, sacroiliitis, ankylosing spondylitis |
| Eyes | Uveitis (iritis), episcleritis |
| Skin | Erythema nodosum, pyoderma gangrenosum |
| Liver/Biliary | Primary sclerosing cholangitis (PSC) - markedly increased in UC (~5% of UC patients); conversely, majority of PSC patients also have UC |
| Mouth | Aphthous stomatitis |
- No granulomas are found in extraintestinal sites in UC (unlike Crohn disease, where granulomas can be found in lymph nodes and other distant organs).
Q7. Discuss the risk of colorectal cancer in IBD.
Answer:
Colitis-associated neoplasia is one of the most serious long-term complications of both UC and colonic Crohn disease.
Risk factors:
- Duration of disease - risk increases beginning 8-10 years after disease initiation
- Extent of involvement - pancolitis carries greater risk than partial involvement
- Severity and frequency of active inflammation - more neutrophilic activity = greater carcinogenic risk
Important exception: In primary sclerosing cholangitis, the risk for dysplasia is markedly greater - surveillance begins at the time of PSC diagnosis, not 8 years after IBD onset.
Progression: Follows the sequence: Chronic inflammation → Dysplasia (flat mucosa, often endoscopically invisible) → Adenocarcinoma
- Risk in UC is confined to the colon
- In Crohn disease, patients are also at increased risk of small intestinal adenocarcinoma
Surveillance: Colonoscopic surveillance with extensive mucosal biopsy approximately 8 years after IBD diagnosis. Advanced endoscopic imaging techniques (chromoendoscopy) are being developed to improve detection of flat dysplastic lesions.
(Robbins & Kumar Basic Pathology, pp. 579-580)
Q8. What are the serologic markers and lab findings in IBD?
Answer:
| Marker | UC | Crohn Disease |
|---|---|---|
| p-ANCA | Positive in ~75% | Positive in ~10% |
| ASCA (anti-Saccharomyces) | Low | More common |
| CRP/ESR | Elevated in active disease | Elevated in active disease |
| Fecal calprotectin | Elevated | Elevated |
| Anemia | Iron deficiency (blood loss) | Multifactorial (iron + B12 + folate) |
| Hypoalbuminemia | In severe disease | Common (malabsorption) |
Q9. What is toxic megacolon and when does it occur?
Answer:
Toxic megacolon is a serious, life-threatening complication seen almost exclusively in Ulcerative Colitis (not Crohn disease).
- Characterized by massive colonic dilation (>6 cm on X-ray) with systemic toxicity (fever, leukocytosis, tachycardia, hemodynamic instability)
- Results from severe transmural inflammation (when inflammation extends beyond the mucosa) impairing neuromuscular function of the colon
- Risk of perforation is high
- Requires emergent management - if unresponsive to medical therapy, emergency colectomy is needed
Q10. What is the treatment approach for IBD?
Answer:
Treatment is aimed at controlling inflammation, inducing and maintaining remission, and preventing complications.
Medical Therapy:
| Severity | Agents |
|---|---|
| Mild disease | Glucocorticoids, aminosalicylates (5-ASA - mesalamine, sulfasalazine) |
| Moderate-severe | Biologic agents - anti-TNF antibodies (infliximab, adalimumab); anti-IL-12/IL-23 antibodies (ustekinumab); anti-integrin antibodies (vedolizumab) |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate |
- Therapies effective in Crohn disease (especially anti-TNF) are also effective in UC.
- Smoking cessation may worsen UC - nicotine trials have been disappointing.
Surgery:
| Crohn Disease | Ulcerative Colitis | |
|---|---|---|
| Role | Reserved for complications (obstruction, fistulas, abscess) | Colectomy is curative |
| Recurrence | Common post-surgery | No recurrence after total colectomy |
| Common procedure | Resection with re-anastomosis | Total proctocolectomy with ileal pouch-anal anastomosis (IPAA) |
(Robbins & Kumar Basic Pathology, p. 580; Robbins Pathologic Basis of Disease, p. 752)
Q11. Write a short note on Granulomas in Crohn Disease.
Answer:
- Non-caseating (sarcoid-like) granulomas are found in approximately 35% of Crohn disease cases - they are a hallmark but not universal.
- Unlike tuberculosis, they do NOT undergo central caseous necrosis.
- They can be found in:
- Any layer of the bowel wall (mucosa, submucosa, muscularis, serosa)
- Mesenteric lymph nodes
- Extraintestinal sites (liver, lungs, skin, eyes) in Crohn disease
- Ulcerative colitis does NOT produce granulomas - this is a key distinguishing histologic feature.
- The presence of granulomas in surgical biopsy specimens helps confirm the diagnosis of Crohn disease when the clinical picture is ambiguous.
Q12. What is meant by "skip lesions" and "cobblestone appearance" in Crohn disease?
Answer:
Skip lesions:
- Alternating segments of diseased and grossly normal bowel, typically separated by several centimeters to several centimeters of uninvolved mucosa.
- This discontinuous pattern distinguishes Crohn disease from UC, which shows continuous mucosal involvement.
- Skip lesions can involve multiple bowel segments simultaneously (e.g., terminal ileum and sigmoid colon, with normal intervening bowel).
Cobblestone appearance:
- Deep, knife-like ulcers (fissures) run along and between the mucosal folds of the bowel.
- The remaining edematous but intact mucosa is elevated by submucosal edema and fibrosis.
- The result is a surface that resembles cobblestones - irregular nodular mucosal islands interspersed with linear ulcer furrows.
- Seen endoscopically and on barium studies.
Summary: Key "Buzzwords" to Remember
| Crohn Disease | Ulcerative Colitis |
|---|---|
| Skip lesions | Continuous/diffuse |
| Transmural | Mucosal only |
| Any GI tract | Colon + rectum only |
| Deep, knife-like ulcers | Superficial, broad-based ulcers |
| Non-caseating granulomas | NO granulomas |
| Cobblestone mucosa | Pseudopolyps, mucosal bridges |
| Creeping fat, fistulas, strictures | Toxic megacolon |
| Thick rubbery wall | Normal wall thickness |
| Recurs after surgery | Curative with colectomy |
| ASCA positive, p-ANCA negative | p-ANCA positive (~75%) |
| NOD2 mutation | IL-10/IL-13 pathway |
| Fat/B12 malabsorption | Blood/mucus in stool |
Sources: Robbins & Kumar Basic Pathology (10th ed.), pp. 576-580 | Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 744-752
This is a shared conversation. Sign in to Orris to start your own chat.