Write assignment on hemodialysis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hemodialysis"[MeSH Terms] AND "complications"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the content needed for a thorough assignment. Let me compile it:
Hemodialysis: A Comprehensive Assignment
1. Introduction
Hemodialysis (HD) is the most widely used form of renal replacement therapy (RRT) for patients with end-stage kidney disease (ESKD) and acute kidney injury (AKI). When conservative medical management - dietary restriction, medications for blood pressure, phosphate, and electrolyte control - can no longer adequately manage the consequences of kidney failure, RRT becomes the only life-sustaining option. In the United States alone, approximately 800,000 patients currently receive some form of RRT, with the majority on HD. The incidence of ESKD is increasing worldwide, driven by longer life expectancies and a rising burden of diabetes mellitus and hypertension, the two most common causes of ESKD globally.
2. Principles of Hemodialysis
Hemodialysis works by passing blood from the patient through an extracorporeal circuit to a device called a dialyzer, where harmful solutes are removed and electrolytes are corrected, before returning the cleaned blood to the patient.
The two fundamental transport mechanisms are:
2.1 Diffusion
Solutes move across a semipermeable membrane down their concentration gradient - from an area of high concentration (the blood) to low concentration (the dialysate). The rate of diffusive transport depends on:
- The magnitude of the concentration gradient
- The membrane surface area
- The mass transfer coefficient of the membrane (a function of membrane porosity, thickness, and solute size)
According to the laws of diffusion, smaller molecules are cleared more efficiently. Urea (molecular weight 60 Da) undergoes substantial clearance, while larger molecules like creatinine (113 Da) are cleared less efficiently.
2.2 Convection (Ultrafiltration)
In addition to diffusion, solutes are swept along with plasma water across the membrane - a process called solvent drag or convective clearance. This is driven by a hydrostatic pressure gradient applied across the dialysis membrane and is responsible for the removal of excess fluid (ultrafiltration). Convective clearance is particularly important for middle-molecule toxins that diffuse poorly.
Key Point: Hemodialysis relies on diffusion across a semipermeable artificial membrane, whereas peritoneal dialysis uses a natural biologic membrane (the peritoneum). - Goldman-Cecil Medicine International Edition, p. 1350
3. The Hemodialysis System
There are three essential components to hemodialysis:
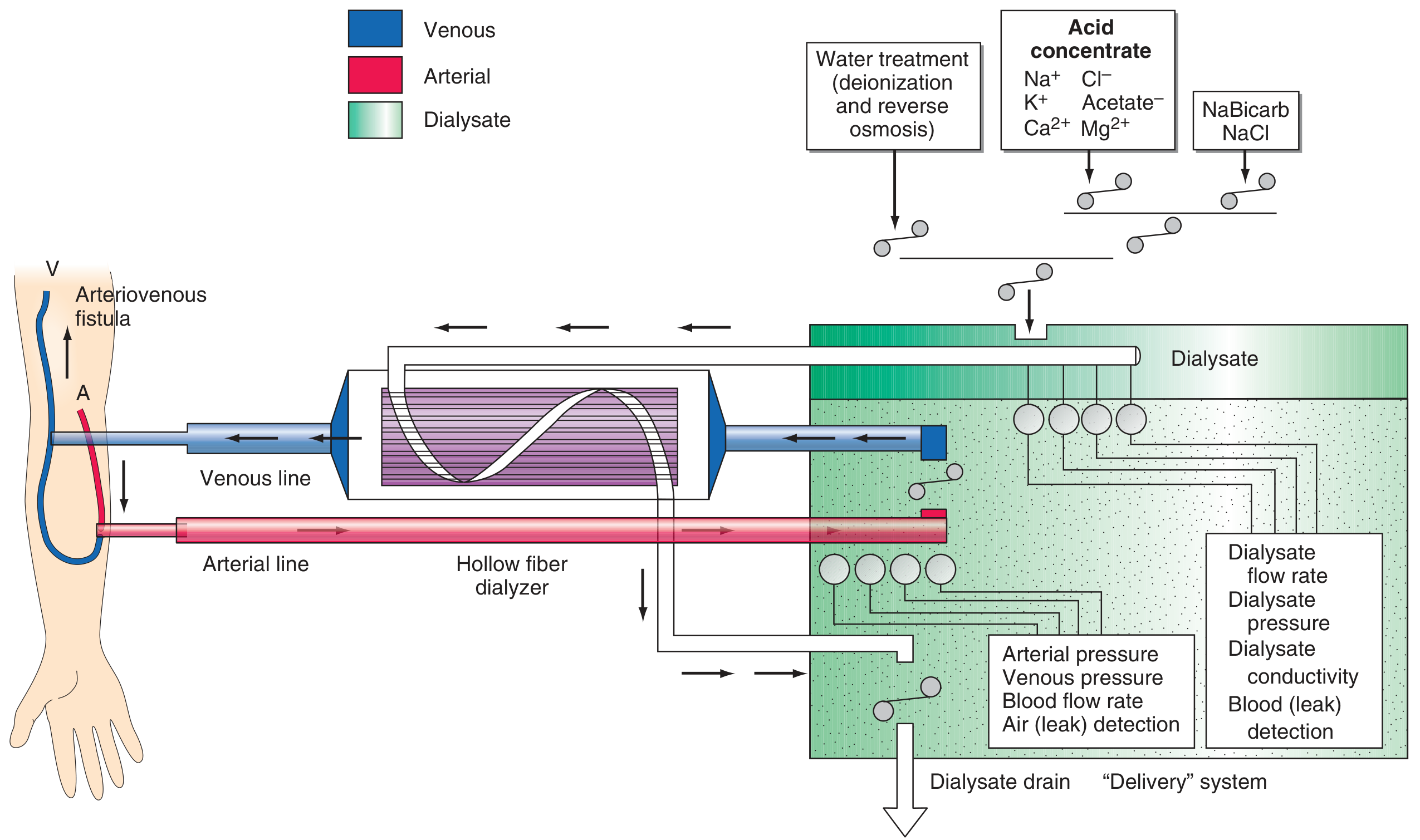
3.1 The Dialyzer
The dialyzer is a plastic chamber that simultaneously perfuses blood and dialysate compartments at high flow rates. The hollow-fiber dialyzer is the most common type in the United States. It consists of bundles of capillary tubes through which blood circulates while dialysate travels countercurrently on the outside of the fiber bundle. This countercurrent arrangement maximizes the concentration gradient and therefore the efficiency of solute removal.
Virtually all dialyzers manufactured today use biocompatible synthetic membranes derived from polysulfone or related compounds. Older cellulose membranes were "bioincompatible" - they activated the complement cascade, causing inflammatory reactions. Their use has largely been discontinued.
3.2 The Dialysate
The dialysate is a carefully composed electrolyte solution that drives diffusion by providing low concentrations of waste solutes. Key components:
| Constituent | Typical Dialysate Concentration | Purpose |
|---|---|---|
| Potassium | 2-4 mmol/L (variable) | Corrects hyperkalemia |
| Bicarbonate | ~35 mEq/L | Corrects uremic metabolic acidosis |
| Calcium | 1.25 mmol/L (2.5 mEq/L) | Corrects calcium balance |
| Sodium | 135-140 mmol/L | Osmotic balance |
The potassium concentration of dialysate can be varied from 0-4 mmol/L depending on the predialysis serum potassium concentration. Very low potassium dialysate (0 or 1 mmol/L) has been associated with an increased risk of sudden death, possibly due to cardiac arrhythmias from rapid potassium shifts.
Because patients are exposed to approximately 120 liters of water during each dialysis treatment, water used for the dialysate is subjected to filtration, softening, deionization, and reverse osmosis to remove microbiologic contaminants and dissolved ions.
Sodium Modeling: In patients who frequently develop hypotension during dialysis, the dialysate sodium concentration can be started high (145-155 mmol/L) and gradually lowered to isotonic levels (135-140 mmol/L) near the end of treatment. This counterbalances urea-related osmolar gradients. However, high dialysate sodium can cause positive sodium balance and excessive thirst.
3.3 The Blood Delivery System
The blood delivery system consists of the extracorporeal circuit and the dialysis access. The blood pump moves blood from the access site through the dialyzer and back to the patient at a blood flow rate of 250-450 mL/min, depending on the type and integrity of vascular access and needle gauge. Negative hydrostatic pressure on the dialysate side is manipulated to control fluid removal (ultrafiltration). Dialysis membranes have different ultrafiltration coefficients (mL removed/min per mmHg).
4. Vascular Access
Reliable vascular access is the lifeline of hemodialysis. There are three main types:
4.1 Arteriovenous Fistula (AVF)
The AVF is the gold standard. It is created by surgically anastomosing an artery directly to a vein - the classic example is the Brescia-Cimino fistula, where the cephalic vein at the wrist is anastomosed end-to-side to the radial artery. This causes "arterialization" of the vein, allowing it to dilate and develop thicker walls, facilitating insertion of large needles (typically 15 or 16 gauge). AVFs have the highest long-term patency of all access types and the lowest infection rates. The "Fistula First" initiative in the United States has promoted AVF creation in a larger fraction of patients. However, AVFs may fail to mature or thrombose early.
4.2 Arteriovenous Graft (AVG)
When patients' vasculature does not allow successful AVF creation (poor arterial inflow or inadequate recipient veins), an AVG is placed - a prosthetic conduit (usually polytetrafluoroethylene, PTFE) is interposed between an artery and vein. The most important complication is thrombosis due to intimal hyperplasia at the graft-vein anastomosis. Catheter-guided angioplasty can dilate stenoses when grafts or fistulas fail.
4.3 Tunneled Central Venous Catheter (CVC)
Large-bore intravenous catheters are often used in patients with AKI or as a bridge in CKD patients. Tunneled catheters (single dual-lumen or two separate catheters placed in the internal jugular or subclavian veins) are used for maintenance HD when fistulas cannot be created or accessed. CVCs carry much higher rates of infection than fistulas or grafts and should be avoided for long-term use whenever possible.
"Failure to convert from central venous catheter access to non-catheter vascular access within 6 months of commencing HD was associated with a higher mortality rate." - Brenner and Rector's The Kidney, MONDO database data
5. Indications for Hemodialysis
RRT (including HD) is typically initiated when the eGFR falls below 10 mL/min/1.73 m², although it may be needed at 10-15 mL/min when comorbid conditions (particularly heart failure) complicate medical management.
Table 1: Indications for Dialysis in Chronic Kidney Disease (Goldman-Cecil Medicine)
| Category | Specific Indication |
|---|---|
| Neurological | Uremic encephalopathy or peripheral neuropathy |
| Cardiovascular | Pericarditis or uremic pleuritis |
| Haematological | Bleeding attributable to uremia |
| Fluid/Electrolyte | Fluid overload refractory to diuretics |
| Haemodynamic | Hypertension poorly responsive to medication |
| Metabolic | Persistent hyperkalemia, metabolic acidosis, hyperphosphatemia, or hypocalcemia refractory to medical therapy |
| Nutritional | Malnutrition or progressive weight loss |
| GI | Persistent nausea and vomiting |
In acute kidney injury (AKI), larger randomized trials have shown that early initiation of RRT offers no survival advantage over delayed initiation - and patients whose dialysis was delayed tended to have earlier spontaneous diuresis, fewer adverse events, and shorter duration of RRT. Routine early initiation (at serum creatinine 7.5 mg/dL) is no better than standard initiation (at ~10 mg/dL).
6. HD Prescription and Adequacy
6.1 Standard Schedule
Conventional HD is typically provided three times per week for 3-4 hours per session at an outpatient dialysis unit. Some patients in increased catabolic states (trauma, glucocorticoid therapy) may require more frequent sessions.
6.2 Measuring Adequacy
Adequacy of HD is measured by urea clearance as a surrogate marker for small-molecular-weight nitrogenous waste products (<500 Da):
-
Urea Reduction Ratio (URR): The percentage fall in blood urea nitrogen (BUN) per session. Target: ≥65%
-
Single-pool Kt/V (spKt/V): A dimensionless index from urea kinetic modeling where K = dialyzer urea clearance (mL/min), t = dialysis duration (min), and V = volume of urea distribution (mL). Target: ≥1.2 on a thrice-weekly schedule.
A more intensive protocol increasing spKt/V from 1.32 to 1.53 does not improve survival and increases the risk of intradialytic hypotension.
6.3 Frequent and Nocturnal Hemodialysis
In-center HD six times per week or nocturnal home HD six times per week improves:
- Kidney-specific quality of life
- Blood pressure control
- Regression of left ventricular hypertrophy
- Serum phosphorus levels
However, it did not reduce mortality at 12 months in randomized trials, although longer follow-up (median 3.6 years) showed a mortality benefit.
7. Complications of Hemodialysis
7.1 Intradialytic Complications
Hypotension is the most common acute complication. Excessive fluid removal is the most frequent cause, but persistent hypotension may signal sepsis or myocardial dysfunction. Management includes:
- Discontinuing ultrafiltration
- Administration of 100-250 mL isotonic saline (or salt-poor albumin in inpatient settings)
- Ultrafiltration modeling (removing more fluid early in the session)
- Dialysate cooling
- Avoiding heavy meals during dialysis
- Excessively rapid fluid removal (>13 mL/kg per hour) must be avoided - it is associated with cardiovascular deaths
Muscle cramps are also common, caused by excessively rapid volume removal or targeting below the patient's dry weight. Prevention: reducing ultrafiltration rate, ultrafiltration profiling, sodium modeling.
Dialyzer reactions occur particularly on first use of a new dialyzer:
- Type A reactions: IgE-mediated hypersensitivity to ethylene oxide (sterilization agent). Occurs within the first few minutes of treatment; can progress to anaphylaxis.
- Type B reactions: Nonspecific chest and back pain from complement activation and cytokine release. Occurs several minutes into the run; typically resolves with continued dialysis.
Other intradialytic symptoms include nausea, vomiting, headache, and chest pain.
7.2 Chronic Complications
Cardiovascular disease is the leading cause of death in ESKD patients. Cardiovascular mortality is higher in patients on dialysis than post-transplant. Contributing factors include:
- Shared risk factors (diabetes, hypertension, dyslipidemia, atherosclerosis)
- Chronic inflammation
- Massive extracellular volume changes (especially with high interdialytic weight gains)
- Inadequate blood pressure control
- Anemia
- Dystrophic (vascular) calcification
- Alterations in cardiovascular dynamics during dialysis
Statins reduce LDL cholesterol in HD patients but clinical trials (4D and AURORA studies) showed no significant reduction in death or cardiovascular events. The SHARP study showed a 17% reduction in major cardiovascular events with simvastatin-ezetimibe in a mixed CKD/dialysis population. Conventional cardioprotective strategies (lipid-lowering agents, aspirin, ACE inhibitors/ARBs, and beta-blockers) are recommended based on individual cardiovascular risk profiles.
Other chronic complications:
- Vascular access problems (thrombosis, infection, steal syndrome)
- High incidence of systemic infections
- Progressive debility and frailty
- Protein-energy malnutrition
- Anemia (treated with erythropoiesis-stimulating agents and IV iron)
- Secondary hyperparathyroidism and renal osteodystrophy
- Impaired cognitive function
- Amyloidosis from beta-2 microglobulin deposition (with long-term HD)
8. Special Modalities
8.1 Hemodiafiltration (HDF)
HDF combines hemodialysis with hemofiltration, providing both diffusive and large-volume convective clearance. It is better at removing middle-molecule toxins (500-60,000 Da, e.g., beta-2 microglobulin) that standard HD clears poorly.
8.2 Continuous Renal Replacement Therapy (CRRT)
In the intensive care setting, CRRT is used for hemodynamically unstable patients with AKI. It provides gentle, continuous fluid and solute removal over 24 hours, avoiding the hemodynamic instability of intermittent HD. Randomized trials have shown that CRRT and intermittent HD lead to similar clinical outcomes in acute renal failure, and intensive dialytic support is not better than standard therapy.
9. Hemodialysis vs. Peritoneal Dialysis
| Feature | Hemodialysis | Peritoneal Dialysis |
|---|---|---|
| Membrane | Synthetic (polysulfone) | Natural (peritoneum) |
| Setting | Mostly in-center (3x/week) | Home-based (daily) |
| Vascular access | Required (AVF/AVG/catheter) | Not required |
| Clearance | High, intermittent | Lower, continuous |
| Preferred in... | Patients near dialysis centers | Remote areas, poorer countries |
| Key complication | Access thrombosis/infection | Peritonitis |
Peritoneal dialysis is more commonly performed in lower-resource settings owing to its lower cost and the high expense of establishing in-center HD units.
10. Global Perspectives
The management of ESKD varies widely by country and region. Notable patterns:
- Japan: >85% in-center HD, high use of AVF (>90%), treatment sessions >4 hours in ~80% of patients, with favorable unadjusted 5-year survival rates of 60% vs. 39% in the USA (2004-2008)
- China: Twice-weekly HD in approximately 20% of patients due to resource constraints
- Middle East: Practice patterns vary widely; quality guidelines have been established in Saudi Arabia, Egypt, and Turkey
- Developing nations: Limited resources may restrict HD to once or twice weekly, and water purification remains a challenge
- Global trend: The dialysis population is expanding, especially among elderly patients and those with diabetes
11. Nursing Considerations in Hemodialysis
Nurses play a central role in the delivery of safe, effective HD care:
- Pre-dialysis assessment: Weight (to calculate fluid to remove), blood pressure, heart rate, temperature, and review of laboratory values (K+, BUN, creatinine, hemoglobin)
- Vascular access care: Inspection for infection, thrombosis, and adequate flow; use of aseptic technique for cannulation
- Patient monitoring during HD: Continuous BP monitoring, pulse, and symptoms of hypotension, cramps, or dialyzer reactions
- Fluid management: Calculate and monitor ultrafiltration rate; target dry weight; avoid rapid fluid removal (>13 mL/kg/hr)
- Anticoagulation management: Heparin is used to prevent clotting in the extracorporeal circuit; monitor for bleeding
- Patient education: Diet (low potassium, phosphate, sodium, fluid restriction), medication adherence, fistula/graft care at home, recognizing danger signs
- Post-dialysis care: Assess for rebound hypertension or hypotension, ensure hemostasis at needle sites, document treatment parameters
12. Conclusion
Hemodialysis is a life-sustaining renal replacement therapy that relies on the principles of diffusion and convection across a semipermeable membrane to remove uremic toxins and correct fluid and electrolyte imbalances in patients with kidney failure. Its three essential components - the dialyzer, dialysate, and blood delivery system - each require careful prescription and monitoring to ensure therapeutic adequacy (spKt/V ≥1.2; URR ≥65%). Vascular access, preferably an arteriovenous fistula, is the cornerstone of durable HD delivery. Common acute complications include intradialytic hypotension and muscle cramps, while cardiovascular disease dominates long-term morbidity and mortality. Global practice patterns vary substantially based on healthcare infrastructure and economic resources, but the overarching goal remains consistent: to optimize patient survival, quality of life, and minimize uremic complications.
References
- Jameson JL, et al. Harrison's Principles of Internal Medicine, 22nd ed. McGraw Hill Medical, 2025. Chapter 323: Dialysis.
- Goldman L, Schafer AJ. Goldman-Cecil Medicine International Edition, 2-Volume Set. Chapter 117: Treatment of Irreversible Renal Failure.
- Taal MW, et al. Brenner and Rector's The Kidney, 2-Volume Set. Elsevier. Chapters on Hemodialysis and Dialysis Outcomes.
- Johnson RJ, et al. Comprehensive Clinical Nephrology, 7th ed. Elsevier.
- National Kidney Foundation. KDOQI Clinical Practice Guidelines for Hemodialysis Adequacy. Available at: www.kidney.org
- Frequent Hemodialysis Network Trial Group. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363:2287.
- Flythe JE, et al. Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality. Kidney Int. 2011;79:250.
This assignment covers hemodialysis from its physiological principles and technical components through clinical indications, prescription, adequacy measurement, complications, and nursing care - drawing from Harrison's (22nd ed.), Goldman-Cecil Medicine, and Brenner and Rector's The Kidney.
This is a shared conversation. Sign in to Orris to start your own chat.