Cholecystectomy
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"cholecystectomy"[MeSH Terms] AND "laparoscopic"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile the full answer.
Cholecystectomy
Cholecystectomy is the surgical removal of the gallbladder. It is one of the most commonly performed abdominal operations worldwide - over 750,000 are done annually in the United States alone. - Schwartz's Principles of Surgery, 11e, p. 1438
1. Historical Background
- 1882: Carl Langenbuch performed the first successful open cholecystectomy
- 1985: Erich Muhe performed the first laparoscopic cholecystectomy using a direct scope
- 1987: Philippe Mouret (France) popularized the laparoscopic approach, which rapidly became the standard of care
Open cholecystectomy was the gold standard for over a century; laparoscopic technique supplanted it and effectively ended interest in non-surgical management options (lithotripsy, bile salt dissolution). - Sabiston Textbook of Surgery, p. 516
2. Indications
Cholecystectomy is indicated for:
| Condition | Notes |
|---|---|
| Symptomatic cholelithiasis (biliary colic) | Most common indication |
| Acute cholecystitis | Early surgery preferred within 72 hours |
| Chronic cholecystitis | Recurrent attacks |
| Choledocholithiasis | With or without ERCP |
| Gallstone pancreatitis | After resolution |
| Gallbladder polyps >10 mm | Cancer risk |
| Gallbladder carcinoma (early) | Curative intent |
| Empyema / gangrene of gallbladder | Urgent |
| Biliary dyskinesia (ejection fraction <35%) | Selected cases |
Early surgical intervention for acute cholecystitis has economic, social, and medical benefits and is the preferred approach for experienced surgeons. After 72 hours of symptoms, the conversion rate to open increases significantly. - Maingot's Abdominal Operations
3. Preoperative Workup
Routine investigations (from Bailey & Love's, 28e):
- Full blood count
- Renal and liver function tests (LFTs)
- Prothrombin time / coagulation screen
- Chest X-ray and ECG (if medically indicated)
- Abdominal ultrasound (primary imaging)
CBD stone risk stratification (Bailey & Love's, Table 71.4):
| Risk | History | LFTs | CBD diameter (USG) | Action |
|---|---|---|---|---|
| Low (2-3%) | No cholangitis/pancreatitis | Normal | ≤6 mm | None needed |
| Medium (20-40%) | Present | 2× normal | 8-10 mm | MRCP ± ERCP |
| High (50-80%) | Jaundice + cholangitis | 2× normal | ≥10 mm | MRCP + ERCP before surgery |
Prophylaxis:
- Antibiotic: second-generation cephalosporin at induction
- DVT prophylaxis: subcutaneous heparin + antiembolic stockings
4. Contraindications
Absolute:
- Inability to tolerate general anesthesia
- Refractory coagulopathy
- Hemodynamic instability / frank peritonitis
- Suspicion of gallbladder carcinoma (relative to laparoscopic approach)
- Severe COPD or CHF (ejection fraction <20%) - cannot tolerate CO₂ pneumoperitoneum
Relative:
- Previous upper abdominal surgery (adhesions)
- Cirrhosis / portal hypertension
- Morbid obesity
- Pregnancy (see below)
- Cholangitis
- Cholecystoenteric fistula
Pregnancy is a special relative contraindication. Laparoscopic cholecystectomy is safest in the second trimester. Key precautions: open port insertion technique, insufflation pressure <12 mmHg, maternal hyperventilation to prevent fetal CO₂ acidosis, laparoscopic ultrasound instead of cholangiogram to limit radiation exposure. - Maingot's
5. Surgical Technique - Laparoscopic Cholecystectomy
This is the gold standard approach.
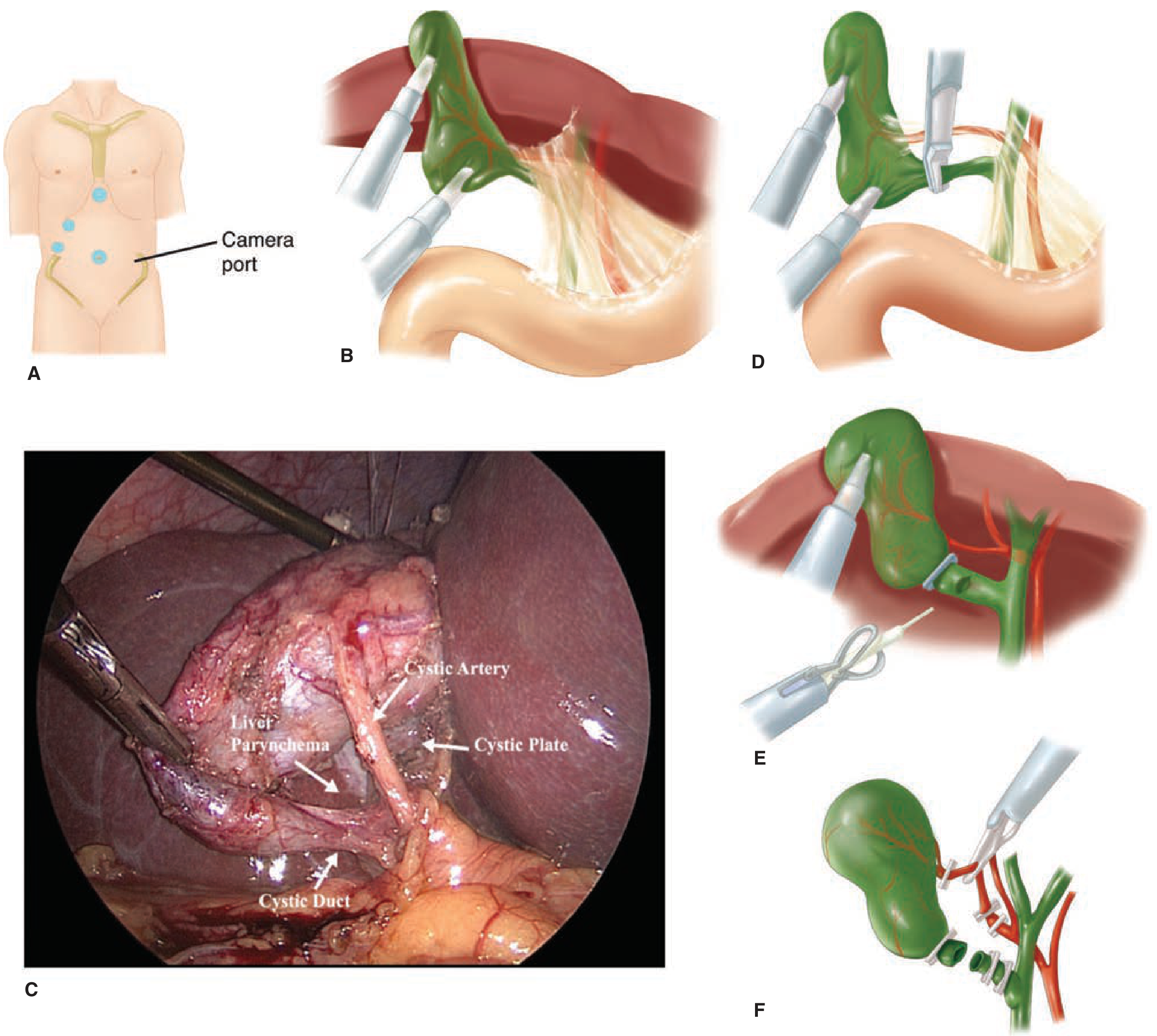
Fig: (A) Four-port trocar placement. (B) Fundus retracted cephalad exposing the hepatocystic triangle. (C) Intraoperative photo of critical view of safety showing cystic artery, cystic duct, and cystic plate. (D-F) Clipping and division of the cystic duct and artery. - Schwartz's Principles of Surgery
Patient Positioning:
- Supine; one arm tucked if intraoperative cholangiogram planned
- Orogastric tube to decompress the stomach
- Reverse Trendelenburg with slight left tilt intraoperatively
- Surgeon stands at the patient's left side
Port Placement (standard 4-port):
- 10-12 mm - periumbilical (camera port; also specimen extraction)
- 10-12 mm - epigastric/subxiphoid (main working port)
- 5 mm - right midclavicular line
- 5 mm - right anterior axillary line (fundus retraction)
Pneumoperitoneum:
- Established with CO₂ to 12-15 mmHg
- Either open (Hasson) technique (open subumbilical cutdown with direct peritoneal visualization - preferred by many to avoid blind trocar injuries) or closed (Veress needle) technique
Operative Steps:
- Fundus retraction - grasped and retracted cephalad over the liver toward the right shoulder
- Infundibulum retraction - pulled inferolaterally to open the Triangle of Calot (hepatocystic triangle)
- Dissection of Calot's triangle - peritoneum divided on both anterior and posterior aspects
- Critical View of Safety (CVS) - mandatory safety step:
- Only two structures seen entering the gallbladder (cystic duct + cystic artery)
- Lower third of gallbladder separated from the liver to expose the cystic plate
- Hepatocystic triangle cleared of fat and fibrous tissue
- Node of Calot (Calot's node) - a useful landmark lying directly over the cystic artery
- Clipping and division - cystic duct clipped proximally and distally, then divided; cystic artery similarly controlled
- Gallbladder dissection from liver bed using electrocautery
- Specimen retrieval through the umbilical port (endobag used if perforated)
- Sabiston Textbook of Surgery; Schwartz's Principles of Surgery; Bailey & Love's 28e
Intraoperative Cholangiogram (IOC):
- Optional but valuable for detecting CBD stones, confirming ductal anatomy, identifying injury
- Selective IOC is indicated when: abnormal LFTs, history of pancreatitis/jaundice, dilated CBD on ultrasound, small stones with large duct
- Routine IOC detects unexpected CBD stones in ~7% of patients
- Laparoscopic ultrasound is an equivalent alternative with no radiation
6. Open Cholecystectomy
Now uncommon; performed when:
- Converting from failed laparoscopic approach (~5% elective; 10-30% emergent/complicated cases)
- Concomitant laparotomy for another indication
Approach: right subcostal (Kocher) incision or midline laparotomy. Dissection typically proceeds fundus-to-cystic duct ("top-down") or from the hepatocystic triangle. In particularly difficult cases, partial cholecystectomy is acceptable - remove as much mucosa as possible, close the cystic duct stump, and drain widely. - Schwartz's
7. Risk Factors for Difficult Cholecystectomy (Bailey & Love's, Table 71.3)
| Category | Risk Factors |
|---|---|
| History | Male gender, >65 years, symptom onset >72-96 hours before presentation, previous upper abdominal surgery, prior cholecystostomy |
| Physical | Morbid obesity, high ASA score |
| Labs | Abnormal LFTs |
| Imaging | Thick-walled GB (>4-5 mm), contracted/shrunken GB, pericholecystic fluid, large stones impacted in Hartmann's pouch |
8. Complications
General Surgical:
| Complication | Notes |
|---|---|
| Wound infection | Lower rate laparoscopic vs. open |
| Incisional hernia | Port sites, especially >10mm |
| Hemorrhage | Cystic artery injury |
Biliary (most serious):
| Complication | Notes |
|---|---|
| Bile duct injury | ~0.2% open; ~0.4% laparoscopic. Classic injury: CBD mistaken for cystic duct and clipped/divided. Risk factors: short cystic duct, stone in Hartmann's pouch, inflammation, excessive traction aligning CBD and cystic duct |
| Bile leak | Cystic duct stump leak, bile duct injury, duct of Luschka |
| Retained CBD stones | Presents post-op with jaundice/cholangitis |
Bile duct injury risk decreases significantly with experience: estimated at 1.7% for first case vs. 0.17% by the 50th case in one regression analysis. - Maingot's
Pneumoperitoneum-related:
- CO₂ embolism (rare but life-threatening)
- Vasovagal reflex
- Cardiac arrhythmias
- Hypercarbic acidosis
- Shoulder tip pain (referred from diaphragmatic irritation)
Trocar-related:
- Abdominal wall hemorrhage/hematoma
- Visceral injury (bowel, bladder)
- Vascular injury (aorta, iliac vessels, IVC) - if suspected, do NOT remove trocar; immediately open and control bleeding
Overall mortality: ~0.1% for laparoscopic cholecystectomy. - Sabiston
9. Postoperative Care & Recovery
- Diet: clear liquids same day, resume normal diet within 24 hours (laparoscopic)
- Discharge: typically same day or next day (laparoscopic)
- Activity: return to full activity within 1-2 weeks
- Open cholecystectomy: 3-5 day hospitalization; 4-6 weeks to full activity
- Follow-up: LFTs if any concern about bile duct injury; ERCP if retained stones suspected
Wound infection and cardiopulmonary complication rates are considerably lower with laparoscopic vs. open cholecystectomy. - Schwartz's
10. Special Situations
Common Bile Duct Exploration (CBDE):
For stones detected pre- or intraoperatively, options include:
- Preoperative ERCP (then cholecystectomy)
- Intraoperative laparoscopic CBDE via cystic duct or choledochotomy
- Flushing small stones with saline + IV glucagon (to relax sphincter of Oddi)
- Postoperative ERCP
Acute Cholecystitis:
- Early lap cholecystectomy is the gold standard when feasible
- After 72 hours: higher conversion rate; consider percutaneous cholecystostomy + delayed elective cholecystectomy 6-8 weeks later in high-risk patients
Single-Incision Laparoscopic Surgery (SILS):
Proposed cosmetic benefit, but systematic reviews show higher failure rate, longer operative time, and increased blood loss without substantive benefit. - Bailey & Love's
Sources:
- Schwartz's Principles of Surgery, 11e - Chapter 32 (p. 1438-1441)
- Sabiston Textbook of Surgery (Current edition) - Chapter 88
- Bailey & Love's Short Practice of Surgery, 28e - Chapter 71
- Maingot's Abdominal Operations - Chapter 48
This is a shared conversation. Sign in to Orris to start your own chat.