Crohn and ulcerative colitis in medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inflammatory bowel disease" AND "Crohn" AND "ulcerative colitis"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have a very comprehensive picture from multiple authoritative sources. Let me compile the full, well-structured answer.
Inflammatory Bowel Disease: Crohn's Disease and Ulcerative Colitis
These two conditions are the principal forms of idiopathic inflammatory bowel disease (IBD). Both are chronic, relapsing-remitting disorders driven by dysregulated mucosal immunity, but they differ fundamentally in location, depth of inflammation, and clinical behavior.
1. Epidemiology
IBD is most prevalent in North America, the United Kingdom, and northern Europe, but incidence is rising globally. In North America:
- Ulcerative colitis (UC): incidence ~19/100,000 person-years; prevalence ~280/100,000
- Crohn's disease (CD): incidence ~20/100,000 person-years; prevalence ~320/100,000
Both conditions peak in the 2nd to 4th decade, with a smaller second peak in the 7th decade. There is no clear gender predominance (F:M ~1:1 for UC; ~1.2:1 for CD). Incidence is highest in White and Ashkenazi Jewish populations, though African American incidence of CD is approaching that of White populations.
Notable risk factors:
-
Cigarette smoking: worsens CD but improves UC course
-
NSAIDs: associated with new onset and exacerbations of IBD
-
Appendectomy (for inflammatory indication): protective against UC
-
Western diet (high fat, high sugar, low fiber): ~2-fold increased IBD risk
-
Goldman-Cecil Medicine, p. 1480
2. Pathobiology
Three pathways interact to trigger IBD: genetic predisposition, immune dysregulation, and an environmental trigger. The current model holds that failure of the innate immune system to clear microbial antigens - combined with increased intestinal epithelial permeability - leads to an overactive adaptive immune response.
Genetics
- 5-20% of IBD patients have a first-degree relative with IBD; first-degree relatives have a 10-15-fold increased risk
- NOD2/CARD15 mutations (chromosome 16): strongest genetic association with CD; NOD2 senses bacterial muramyl dipeptide - mutations lead to impaired recognition and dysregulated NF-κB activation
- ATG16L1 and IRGM genes (autophagy pathway): also linked to CD
- IL-23 receptor gene polymorphisms: linked to UC and varied CD risk
- Toll-like receptor-4 gene polymorphisms: linked to both CD and UC
- ADCY7 missense mutation: leads to excessive inflammatory response predisposing to UC
- HLA class II polymorphisms (especially HLA-DR): increased risk for UC
Immunology
- Both CD and UC involve dysregulated innate immunity triggering T cells and humoral response
- Th17 cells are activated in both conditions, stimulated by IL-23 produced by antigen-presenting cells
Microbiome
-
Colitis does not develop in animal models in a sterile environment
-
The terminal ileum and colon (highest bacterial density, ~10¹² organisms/g) are the preferentially affected sites
-
Debaryomyces hansenii (Candida famata) has been implicated in Crohn tissue
-
Goldman-Cecil Medicine, p. 1479-1480
3. Key Distinguishing Features
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| GI involvement | Esophagus to anus ("mouth to anus") | Colon only |
| Pattern | Skip lesions (discontinuous) | Continuous, starts in rectum |
| Depth of inflammation | Transmural | Mucosal/submucosal only |
| Ulceration type | Usually discrete | Continuous |
| Fistulae | Yes (20-40%) | No |
| Strictures | Yes | Rare |
| Perianal disease | Yes (up to 30%) | No |
| Granulomas (histology) | Noncaseating granulomas (up to 70% surgical specimens) | Absent |
| Peak age of onset | 15-30 yr (2nd peak 7th decade) | 20-40 yr (2nd smaller peak beyond 7th decade) |
| Sex (F:M) | 1.2:1 | 1:1 |
- Goldman-Cecil Medicine, p. 1481
4. Pathology
Crohn's Disease
- Early: acute inflammatory infiltrate in lamina propria, cryptitis, crypt abscesses
- Later: distorted crypt architecture with lymphocytic infiltrate, branching/shortening of crypts
- Pathognomonic (when present): noncaseating granulomas (found in ~15% endoscopic biopsies, up to 70% surgical specimens)
- Surgical specimens: transmural wall inflammation; fat creeping on serosal surface ("creeping fat")
Ulcerative Colitis
- Begins in the rectum, extends proximally in a continuous pattern
- Mild disease: granular, hyperemic, edematous mucosa
- Severe disease: mucosal ulceration extending into lamina propria
- Chronic disease: pseudopolyps (from epithelial regeneration), loss of normal fold pattern, colonic shortening and narrowing
- Histology: epithelial necrosis, acute inflammatory infiltrate, cryptitis/crypt abscesses; with chronicity - lymphocytic infiltrate and crypt architectural distortion
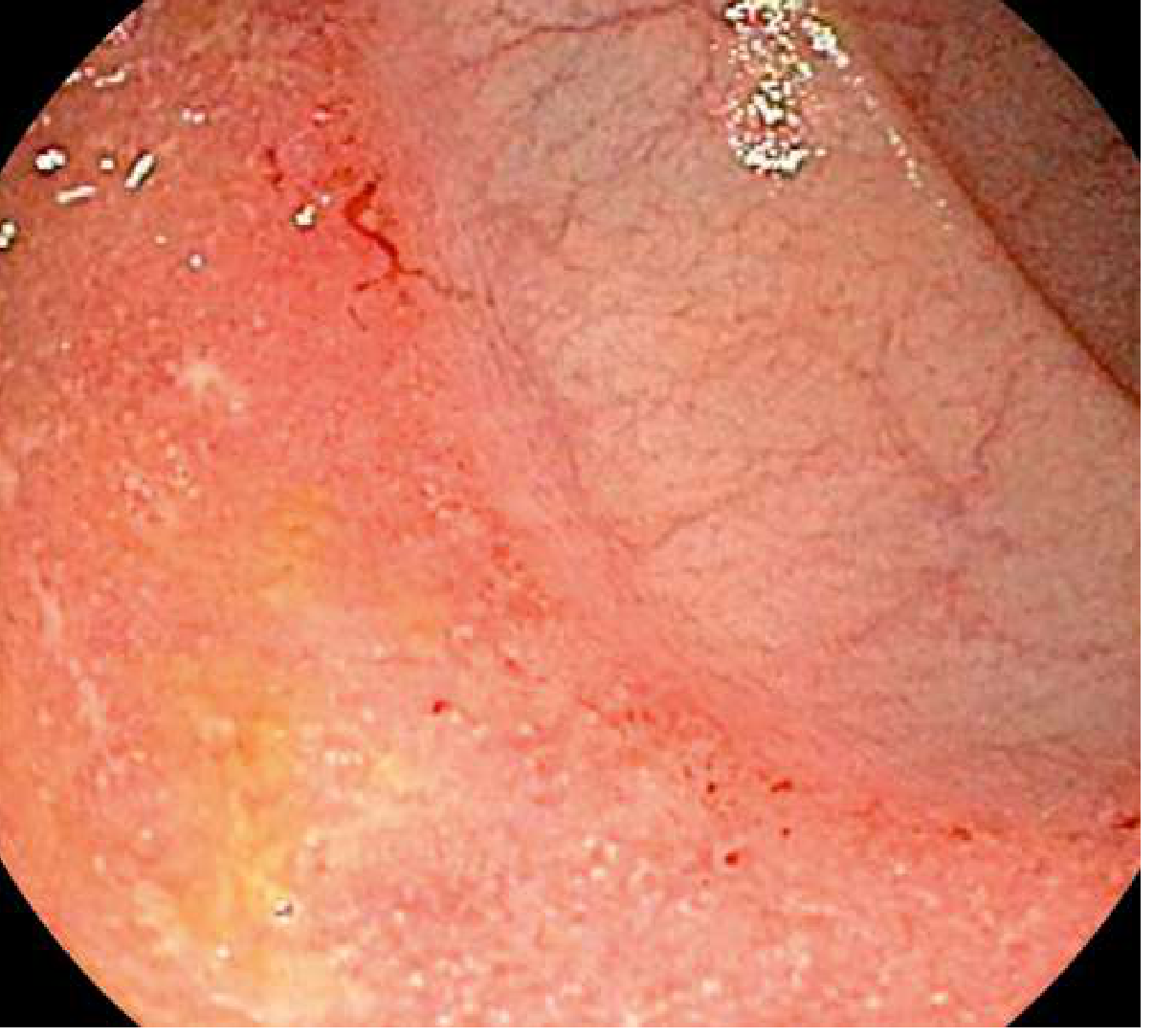
Endoscopic appearance of UC - diffuse mucosal erythema, friability, contact bleeding:
- Goldman-Cecil Medicine, p. 1481
5. Clinical Manifestations
Crohn's Disease
- Terminal ileum affected in ~70% (ileal disease 30%, ileocolonic 40%)
- Symptoms: right lower quadrant pain, diarrhea, hematochezia, fatigue; fever and weight loss with more severe disease
- Obstructive symptoms (pain, distention, nausea) when strictures develop
- Perianal disease (fissures, skin tags, fistulae, abscesses) in up to 30%
- Fistulae in 20-40%: enterocutaneous, rectovaginal, enterovesicular, enteroenteric
- Upper GI involvement in ~5% (esophageal in <2%); gastroduodenal in 0.5-4%
Ulcerative Colitis
- At diagnosis: 44-49% have proctosigmoiditis; 36-41% disease beyond rectum; 14-37% pancolitis
- Symptoms: hematochezia, diarrhea, tenesmus, excess mucus, urgency
- Proctitis/proctosigmoiditis may cause constipation (paradoxically)
- Severe disease: weight loss, fever, nausea/vomiting, anemia, hypoalbuminemia, peripheral edema
Extraintestinal Manifestations
-
Crohn's is more frequently associated with: arthritis, aphthous stomatitis, uveitis, erythema nodosum, ankylosing spondyloarthropathy
-
UC is most associated with: inflammatory arthropathies and primary sclerosing cholangitis (PSC)
-
Both: skin lesions (pyoderma gangrenosum), eye disease, bone disease
-
Rosen's Emergency Medicine, p. 1334; Goldman-Cecil Medicine, p. 1481-1482
6. Diagnosis
Laboratory
- Anemia (iron deficiency from blood loss; B12/folate deficiency from terminal ileal disease or resection in CD)
- Elevated ESR, CRP (reflect inflammatory activity)
- Hypoalbuminemia, leukocytosis, thrombocytosis in active disease
- Fecal calprotectin: sensitive marker of gut mucosal inflammation, helpful for monitoring
- ANCA (perinuclear): associated with UC; ASCA (anti-Saccharomyces cerevisiae antibodies): associated with CD
Endoscopy and Biopsy
- Colonoscopy with biopsy is the cornerstone of diagnosis
- For UC: starts in rectum, continuous inflammation; biopsy shows crypt distortion, continuous mucosal inflammation, absence of granulomas, absence of small bowel disease
- For CD: skip pattern of ulceration, discrete ulcers, can involve small bowel or upper GI; noncaseating granulomas confirm CD if present
Radiology
- CT enterography / MRI enterography have replaced barium studies - best for assessing extent, severity, strictures, fistulae, abscesses, and perianal disease in CD
- CT/MRI also essential for detecting intra-abdominal and perianal abscesses
Disease Severity Scoring
The Crohn's Disease Activity Index (CDAI) weights:
-
Liquid/soft stools × 7 days (×2)
-
Abdominal pain severity × 7 days (×5)
-
General well-being × 7 days (×7)
-
Complications (×20), antidiarrheal use (×30), abdominal mass (×10), hematocrit deviation (×6), weight deviation (×1)
-
Goldman-Cecil Medicine, p. 1482-1485
7. Disease Severity Classification
Ulcerative Colitis
| Severity | Criteria |
|---|---|
| Mild | <4 stools/day, may have some blood, no systemic toxicity |
| Moderate | >4 stools/day, minimal signs of toxicity |
| Severe | >6 bloody stools/day, signs of systemic toxicity |
Crohn's Disease
| Severity | Criteria |
|---|---|
| Mild-Moderate | Ambulatory, eating, no dehydration, no toxicity, weight loss <10% |
| Moderate-Severe | Failed mild treatment; systemic toxicity, significant weight loss, anemia, fever, abdominal pain, intermittent N/V |
| Severe | Persistence despite steroids/biologics; high fever, persistent vomiting, obstruction, rebound tenderness, cachexia, abscess |
- Rosen's Emergency Medicine, p. 1334
8. Treatment
Medical Therapies Overview
| Drug Class | Examples | Dosing Notes |
|---|---|---|
| 5-Aminosalicylates (5-ASA) | Sulfasalazine, mesalamine, olsalazine, balsalazide | 2-6 g/day; various release formulations; backbone of UC treatment, NOT effective in CD |
| Corticosteroids | Prednisone, methylprednisolone, budesonide | Induction only; avoid for maintenance |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate | Slow onset; steroid-sparing; adjunctive |
| Anti-TNF biologics | Infliximab (IV), adalimumab (SC), certolizumab pegol | Remission in ~50%; increased risk of infection/malignancy |
| Anti-integrin | Vedolizumab (IV), natalizumab | Inhibit T-lymphocyte gut migration; alternative to anti-TNF |
| Anti-IL-12/23 | Ustekinumab | Refractory CD and UC |
| JAK inhibitors | Tofacitinib, upadacitinib | Moderate-severe UC |
| Antibiotics | Ciprofloxacin 500 mg BD, metronidazole 500 mg TDS | Only for complications (abscess, fistula) in CD; not for UC |
Crohn's Disease Treatment by Severity
- Mild-moderate ileocecal CD: ileal-release budesonide 9 mg PO once daily for 8 weeks (minimal systemic effects due to first-pass metabolism)
- Mild-moderate CD colitis / ileocolonic: 8-week systemic corticosteroid course; prednisone 0.5-0.75 mg/kg/day (typically 40-60 mg/day)
- Esophageal/gastroduodenal CD: proton pump inhibitor only for mild disease
- Extensive small bowel CD: systemic corticosteroids + biologic (anti-TNF)
- Moderate-severe CD responsive to steroids: add azathioprine 1.5-2.5 mg/kg/day PO or 6-mercaptopurine 0.75-1.5 mg/kg/day; methotrexate 25 mg/week SC/IM
- Refractory CD: anti-TNF (infliximab, adalimumab, certolizumab) - equivalent efficacy; vedolizumab for anti-TNF failures
- Aminosalicylates are NOT recommended for CD (meta-analyses show no benefit over placebo)
- Hospitalized patients: methylprednisolone 1 mg/kg/day IV; avoid steroids for long-term maintenance (risk of osteopenia, osteonecrosis, GI mucosal injury)
Ulcerative Colitis Treatment
-
5-ASA drugs are the mainstay (effective in UC but not CD)
-
Mesalamine enema (4 g/day) or suppository (1 g/day) for distal/rectal disease
-
Oral 5-ASA for more proximal disease
-
Corticosteroids for moderate-severe flares
-
Immunomodulators and anti-TNF (infliximab) for steroid-refractory/dependent disease
-
Tofacitinib and upadacitinib (JAK inhibitors) for moderate-severe UC
-
Surgery (colectomy) is curative for UC - unlike CD where surgery does not cure
-
Rosen's Emergency Medicine, p. 1334-1335; Goldman-Cecil Medicine, p. 1484
9. Complications
Life-Threatening
- Toxic megacolon: pathologic colonic dilation from transmural inflammation causing smooth muscle paralysis, dilation, and eventual perforation. The hallmark is colonic dilation in a systemically toxic patient. Can occur in both CD and UC.
- Intestinal perforation: from deep ulceration or toxic megacolon
- Fulminant colitis: severe colitis with systemic toxicity, >10 bloody stools/day, requiring urgent hospitalization
CD-Specific
- Intestinal strictures (from chronic fibrosis) leading to small bowel obstruction (SBO)
- Fistulae (enterocutaneous, rectovaginal, enterovesicular, enteroenteric)
- Abscesses (perianal and intra-abdominal)
- Short bowel syndrome (from multiple resections)
- Up to 75% of CD patients will undergo at least one abdominal surgery in their lifetime; 50% require surgery within 10 years, 80% within 20 years; surgery is not curative
Shared
-
Colorectal cancer risk is elevated in both - increases with disease duration and extent; ongoing endoscopic surveillance is required
-
Thromboembolic disease (DVT/PE) - DVT/PE prophylaxis important in hospitalized patients
-
Malabsorption and nutritional deficiencies (iron, B12, folate, fat-soluble vitamins)
-
Rosen's Emergency Medicine, p. 1332-1335; Goldman-Cecil Medicine, p. 1482-1484; Sleisenger and Fordtran's GI and Liver Disease, p. 2498
10. Surveillance and Cancer Risk
- Long-standing IBD (especially UC with pancolitis) significantly increases colorectal cancer risk
- Regular colonoscopic surveillance with multiple biopsies is mandated - frequency depends on duration, extent, and activity of disease
- Primary sclerosing cholangitis (common in UC) adds an independent risk for cholangiocarcinoma
Recent Evidence (2024-2025)
A 2024 AGA network meta-analysis in Gastroenterology synthesized comparative efficacy of advanced therapies for moderate-to-severe UC, confirming that newer biologics and JAK inhibitors differ in their benefit-risk profiles and guiding updated treatment sequencing. A meta-analysis in UEGJ (2024) found probiotics have modest but statistically significant effects in IBD remission maintenance. A 2025 systematic review in Gut also highlights emerging evidence linking environmental pollutants to increased IBD risk and worse outcomes.
Sources:
- Goldman-Cecil Medicine (26th ed.), Chapter 127 - Inflammatory Bowel Disease, p. 1479-1485
- Rosen's Emergency Medicine (10th ed.), Chapter 81 - Inflammatory Bowel Disease, p. 1332-1336
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (11th ed.), p. 2498
Refer from manipal manual book
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have checked the complete library catalog. Unfortunately, the Manipal Manual of Medicine (also known as the "Manipal Manual" or "Manual of Medical Diagnosis") is not available in the textbook library. The library contains 130+ titles across all medical specialties, but the Manipal Manual is not among them.
Here is the full list of internal medicine / gastroenterology titles available that cover Crohn's and UC in depth:
| Book | Speciality |
|---|---|
| Goldman-Cecil Medicine (International Ed., 2 Vol Set) | Internal Medicine |
| Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Gastroenterology |
| Yamada's Textbook of Gastroenterology (7th ed, 3 Vol) | Gastroenterology |
| Harrison's Principles of Internal Medicine (22nd ed, 2025) | Internal Medicine |
| Rosen's Emergency Medicine | Emergency Medicine |
| The Washington Manual of Medical Therapeutics | Internal Medicine |
| Swanson's Family Medicine Review | Family Medicine |
The answer I already gave you on Crohn's and UC was drawn from Goldman-Cecil Medicine and Sleisenger & Fordtran's - two of the most authoritative and comprehensive internal medicine and GI textbooks available. These are actually considered more detailed references than the Manipal Manual for the topics covered.
Would you like me to:
- Pull the same topic from Harrison's (22nd ed, 2025) which is the closest equivalent to Manipal in exam-oriented internal medicine content?
- Check The Washington Manual for a concise clinical summary format (similar to Manipal's style)?
- Look in Yamada's Gastroenterology for more detailed GI-specific content?
This is a shared conversation. Sign in to Orris to start your own chat.