Functional cast position
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough summary of the functional cast position (also called the "position of function" or "functional position") of the hand, as described across multiple authoritative orthopaedic and emergency medicine textbooks.
Functional Cast Position of the Hand
The functional position (also called the "position of function" or "intrinsic plus position") is the standard reference posture used when immobilizing the hand in a cast or splint to prevent contractures and preserve long-term hand function.
Joint Angles
| Joint | Position |
|---|---|
| Wrist | 20-40° of dorsiflexion (extension) |
| MCP joints | 70-90° of flexion |
| PIP joints | 0-10° of flexion (near full extension) |
| DIP joints | 0° (full extension) |
| Thumb | Abducted away from the palm |
| Forearm | Neutral position |
Different sources cite slightly varying wrist angles (10-20° per Roberts & Hedges, 30° per Rosen's, 40° per Rockwood & Green), but all agree the wrist should be in slight-to-moderate extension.
Illustrations
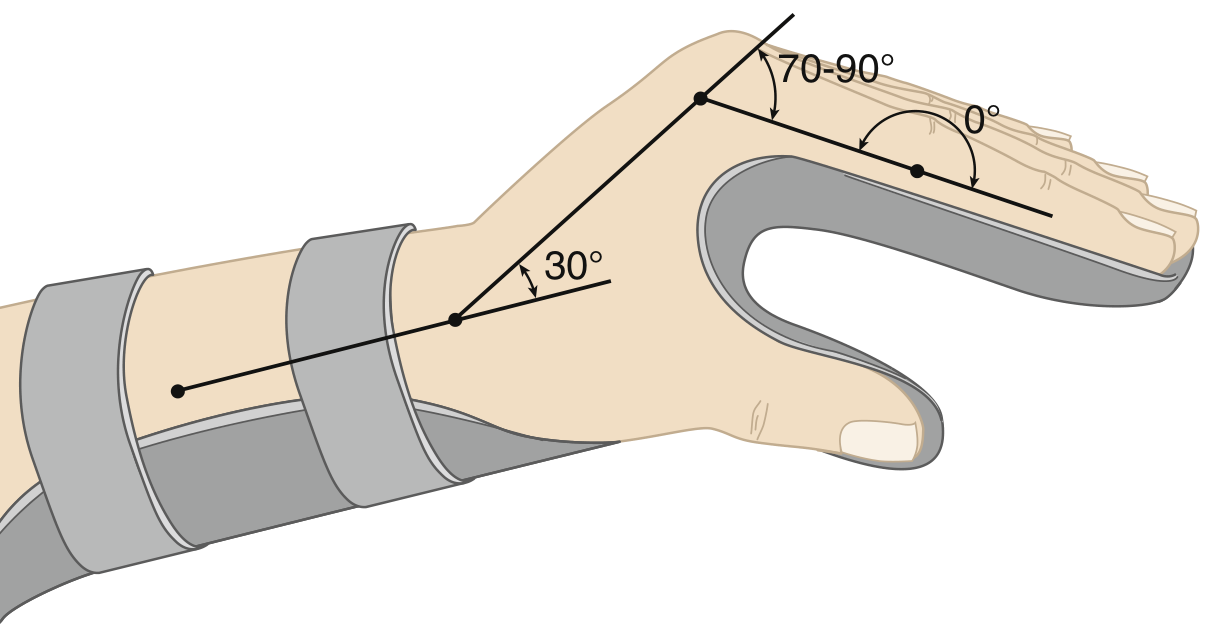
Fig. 42.5 from Rosen's Emergency Medicine - Functional position with wrist at 30° extension, MCP at 70-90° flexion, PIP/DIP at 0°:
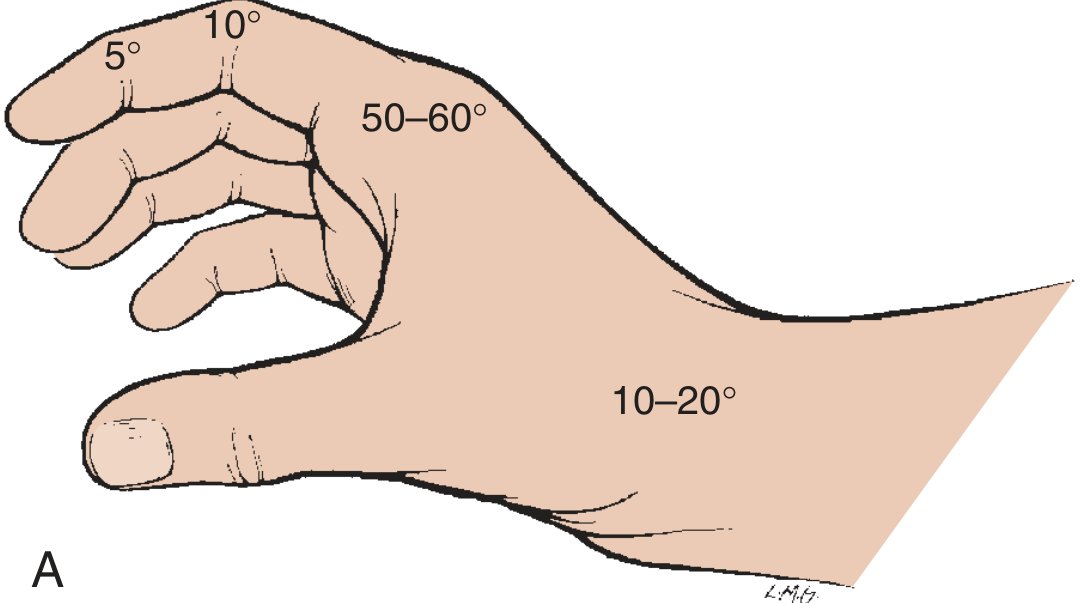
"Wineglass position" from Roberts & Hedges - showing wrist at 10-20°, MCP at 50-60°, IP joints in slight flexion (5-10°):
Rationale
The rationale is purely anatomical:
-
MCP collateral ligaments are lax in extension and taut in flexion. If the MCP is immobilized in extension, the collateral ligaments shorten and a flexion contracture develops. Splinting in 70-90° flexion keeps the ligaments stretched.
-
PIP/DIP volar plates are prone to shortening if the IP joints are held in flexion. Keeping them extended prevents flexion contractures.
-
Wrist extension optimizes the length-tension relationship of the extrinsic flexor and extensor tendons, allowing balanced resting tension.
"The functional anatomy of the MCP joint also illustrates the importance of splinting the joint in flexion to avoid shortening and subsequent stiffening of the collateral ligaments."
- Rosen's Emergency Medicine
Named Casts Using This Position
- James Cast (from Rockwood & Green's, 10th ed.): Wrist at 40° dorsiflexion, MCP at 70-90° flexion, IP joints in full extension. Applied as a volar slab + forearm cast. Designed so collateral ligaments are maximally stretched, preventing contracture.
- Burkhalter Cast: Similar principle; another named hand cast used in fracture management.
Functional vs. Intrinsic Plus Position
These two terms are sometimes used interchangeably but can be distinguished:
| Feature | Position of Function ("wineglass") | Intrinsic Plus |
|---|---|---|
| Wrist extension | 10-20° | 20-30° |
| MCP flexion | 50-60° | 70-90° |
| IP flexion | 5-10° | 0° (full extension) |
| Best for | Short-term splinting (7-14 days) | Longer immobilization, metacarpal neck fractures |
Both are acceptable for initial ED splinting; neither has been proven superior for the first few weeks.
Clinical Application
- Used for general hand/finger fractures, tendon repairs, hand infections, and burns.
- Incorrect splinting is one of the most common causes of chronic hand stiffness after injury.
- The operated area in skin grafts should also be held in a functional position with maximal stretching of the graft site.
Sources: Rosen's Emergency Medicine (9th ed.), Roberts & Hedges' Clinical Procedures in Emergency Medicine, Rockwood & Green's Fractures in Adults (10th ed. 2025), Campbell's Operative Orthopaedics (15th ed. 2026), THIEME Atlas of Anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.