Epithelial and leukocyte cell in urine microscope
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the images and content needed for a thorough answer. Here is the complete guide:
Epithelial and Leukocyte Cells in Urine Microscopy
Cellular elements in urine sediment come from two sources: (1) desquamated epithelial lining cells of the kidney and lower urinary tract, and (2) cells of hematogenous origin (leukocytes and erythrocytes). Bright-field microscopy works best with a crystal-violet safranin stain to delineate formed elements; phase-contrast microscopy helps with translucent structures.
Leukocytes (White Blood Cells)
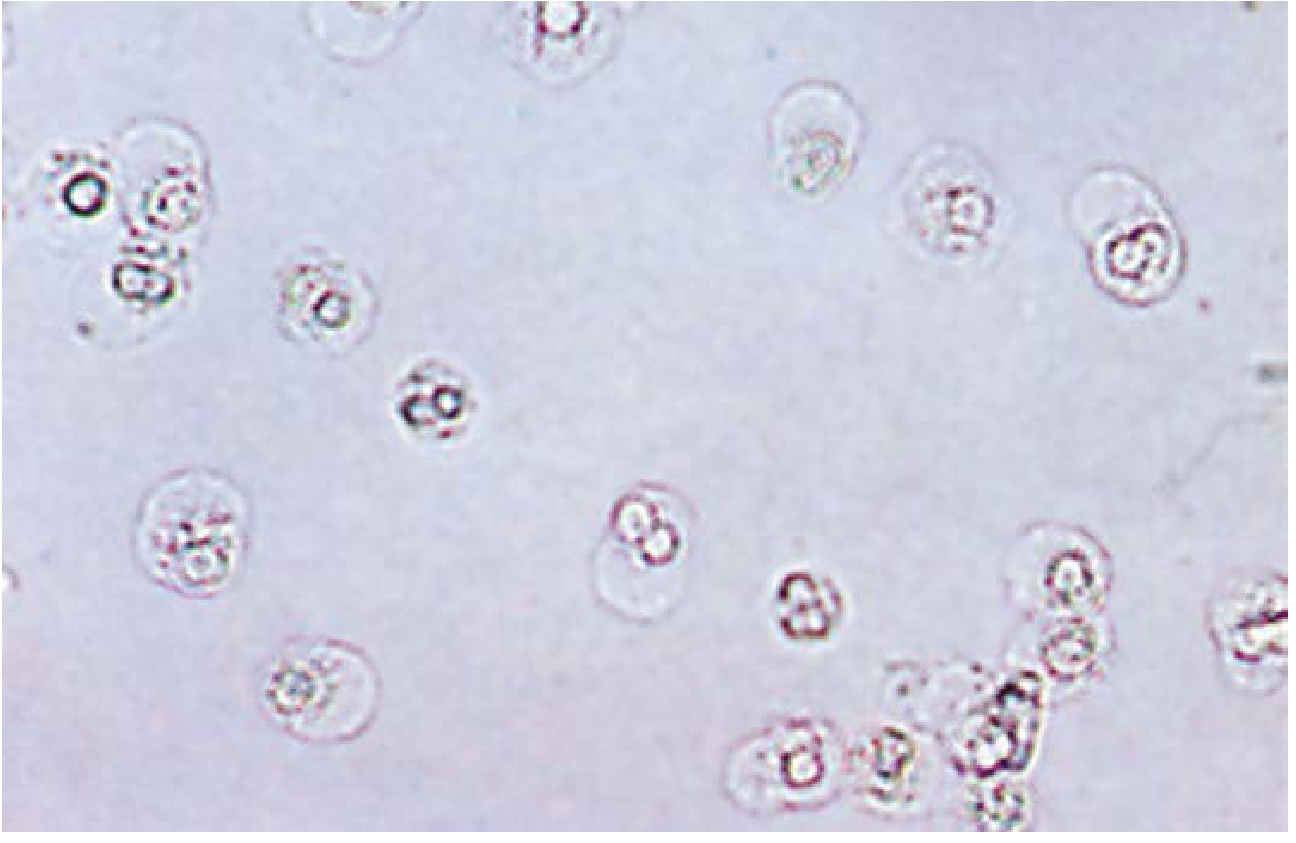
Neutrophils (PMNs)
The predominant WBC type in urine.
- Size: ~12 μm in diameter
- Appearance: Granular spheres with multilobated (segmented) nuclei
- Degenerating forms: Nuclear detail is lost; may be confused with renal tubular epithelial cells. Adding dilute acetic acid enhances nuclear detail.
- Glitter cells: In dilute/hypotonic urine, neutrophils swell and their granules show Brownian movement, giving a sparkling refractile appearance.
- Normal: < 5 leukocytes/hpf
- Pyuria: > 5 leukocytes/hpf - indicates infection or inflammation. > 30 cells/hpf suggests acute infection.
- Clinical significance: Pyelonephritis, cystitis, urethritis, prostatitis. Leukocyte casts + pyuria = renal origin.
Staining: With crystal-violet safranin - nuclei appear reddish-purple, cytoplasmic granules violet. Leukocyte esterase strip confirms pyuria in hypotonic specimens.
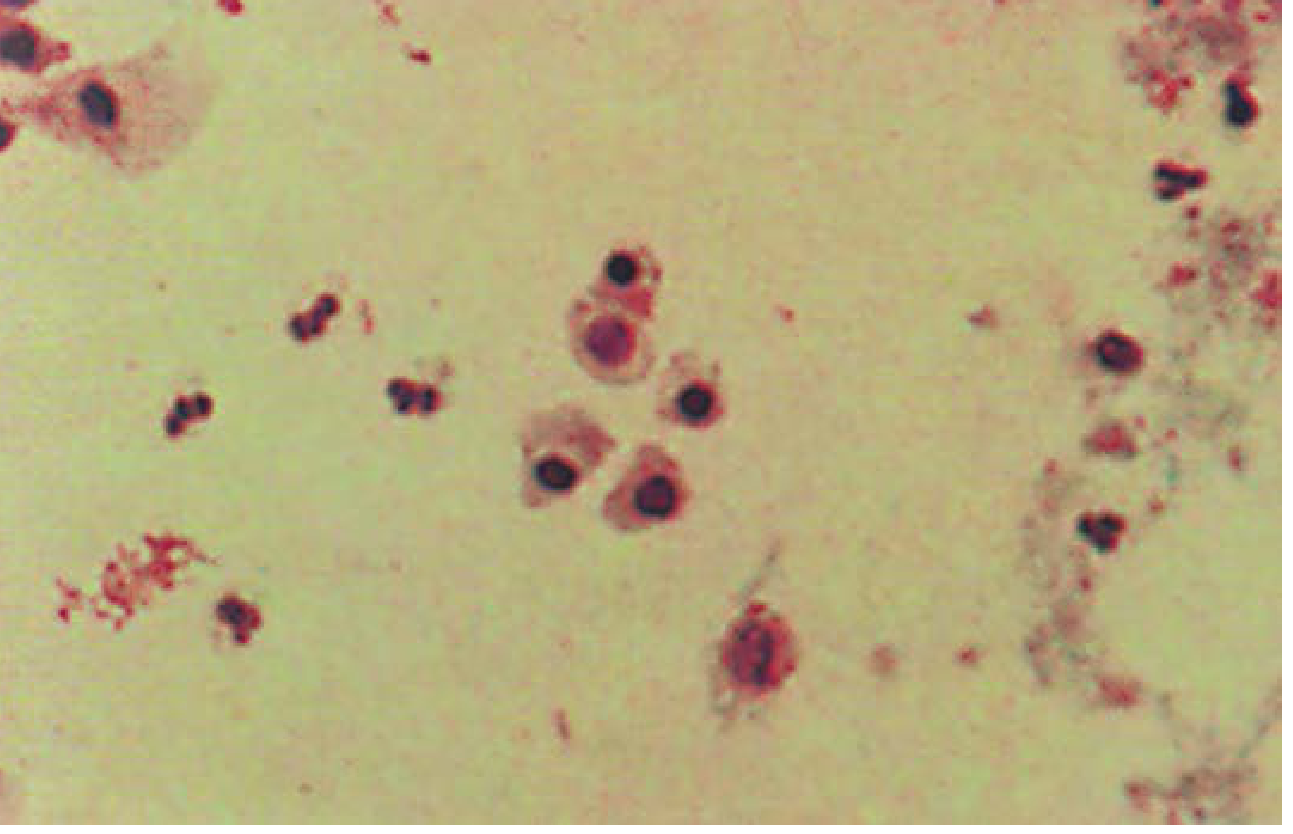
Fig. 29.6 - Neutrophils with dilute acetic acid (x100):
Eosinophils
- Not normally seen; > 1% of leukocyte population is significant
- Requires Hansel stain (methylene blue + eosin-Y in methanol), Wright, or Papanicolaou stain for identification
- Clinical significance: Allergic interstitial nephritis (drug hypersensitivity - penicillins), UTIs, renal transplant rejection
Lymphocytes and Mononuclear Leukocytes
- Small lymphocytes normally present in small numbers
- Mononuclear cells (histiocytes, lymphocytes, plasma cells) constituting ≥ 30% of differential = chronic inflammation
- Increased lymphocytes in renal transplant rejection
Epithelial Cells
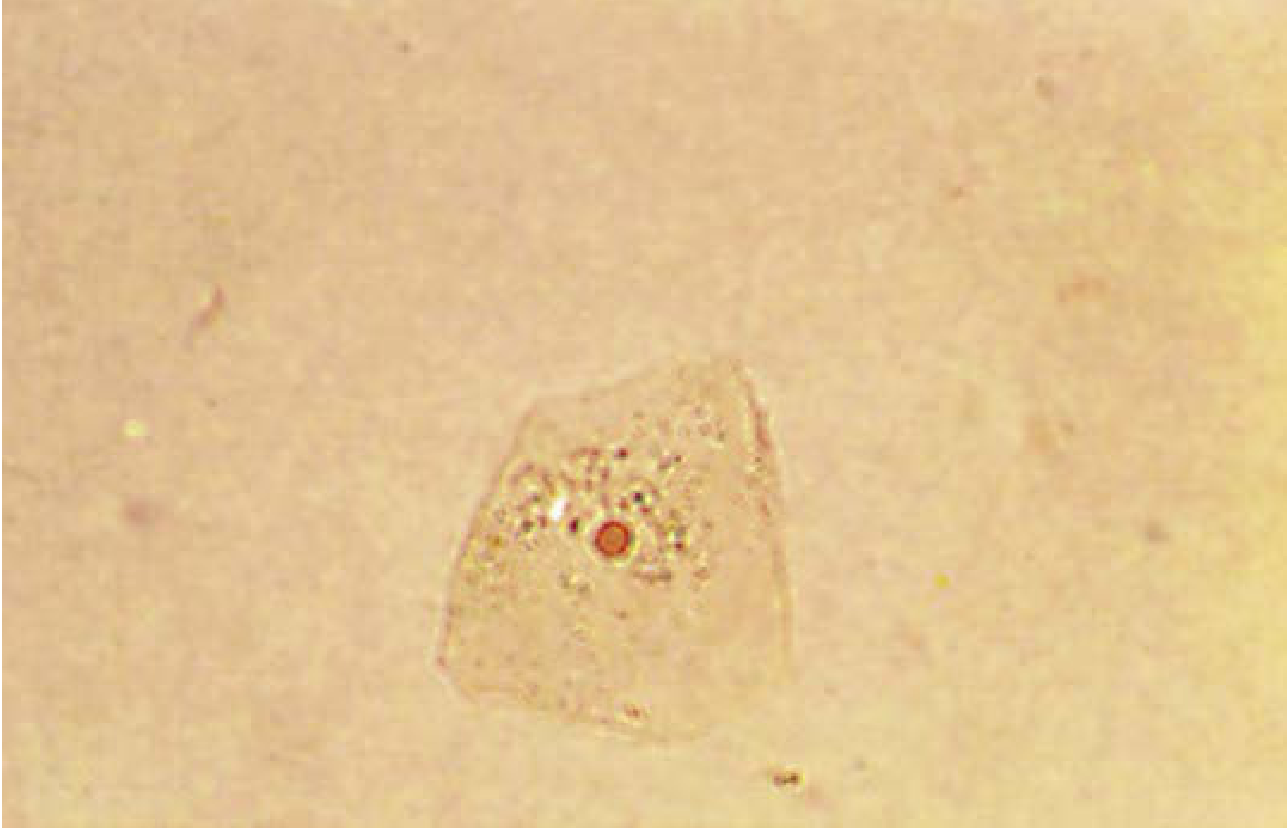
1. Squamous Epithelial Cells
The most common and least significant epithelial cells in urine.
- Origin: Distal one-third of urethra; in females, also from vagina/vulva
- Size: Large (largest epithelial cells in urine)
- Appearance: Flat, abundant cytoplasm, small round central nucleus, edges often folded
- Staining: Nuclei purple, cytoplasm pink to violet (crystal-violet safranin)
- Significance: Contamination marker; large numbers in female urine suggest vaginal contamination
Fig. 29.8 - Squamous epithelial cell, Pyridium stained (x200):
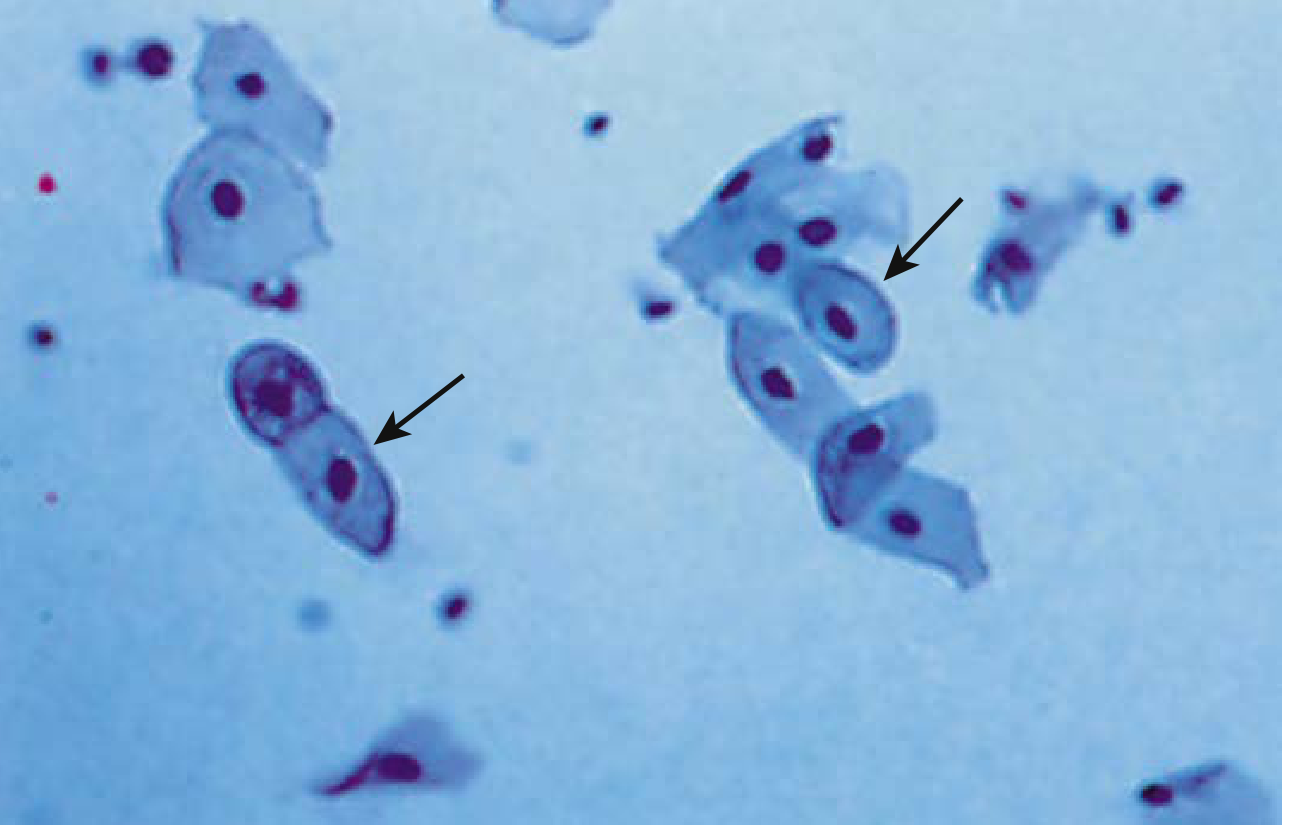
2. Transitional (Urothelial) Epithelial Cells
- Origin: Renal pelvis to lower third of urethra
- Size: 40-200 μm; smaller than squamous cells
- Appearance: Round or pear-shaped, round centrally located nucleus; occasional binucleate forms; characteristic endo-ecto cytoplasmic rim
- Staining: Dark-blue nuclei, pale-blue cytoplasm
- Significance: A few are normal (desquamation). Large clumps or sheets without instrumentation - requires cytology to rule out transitional cell carcinoma
Fig. 29.9 - Transitional epithelial cells, Papanicolaou stained (x430):
(Arrows point to characteristic pear-shaped cells with prominent nuclei)
3. Renal Tubular Epithelial Cells (RTECs)
The most clinically significant epithelial cells - increased numbers indicate tubular damage.
Proximal/Distal Convoluted Tubular Cells:
- Size: 14-60 μm (large, oblong)
- Coarsely granular eosinophilic cytoplasm
- Small nuclei with dense chromatin, rare nucleoli; may be multiple
Collecting Duct Cells:
- Size: 12-20 μm
- Cuboidal or polygonal shape
- Large, slightly eccentric nucleus
- Basophilic endo-ecto cytoplasmic rim
Clinical significance of RTECs:
| Condition | Finding |
|---|---|
| Acute tubular necrosis (ATN) | Increased RTECs + granular casts + "muddy brown" casts |
| Drug/heavy metal toxicity | Increased proximal/distal tubular cells |
| Renal transplant rejection | Collecting duct cells + eosinophils + lymphocytes |
| Ischemic necrosis | Renal epithelial fragments (≥3 collecting duct cells = basement membrane disruption) |
Fig. 29.10 - Renal tubular epithelial cells (x200):
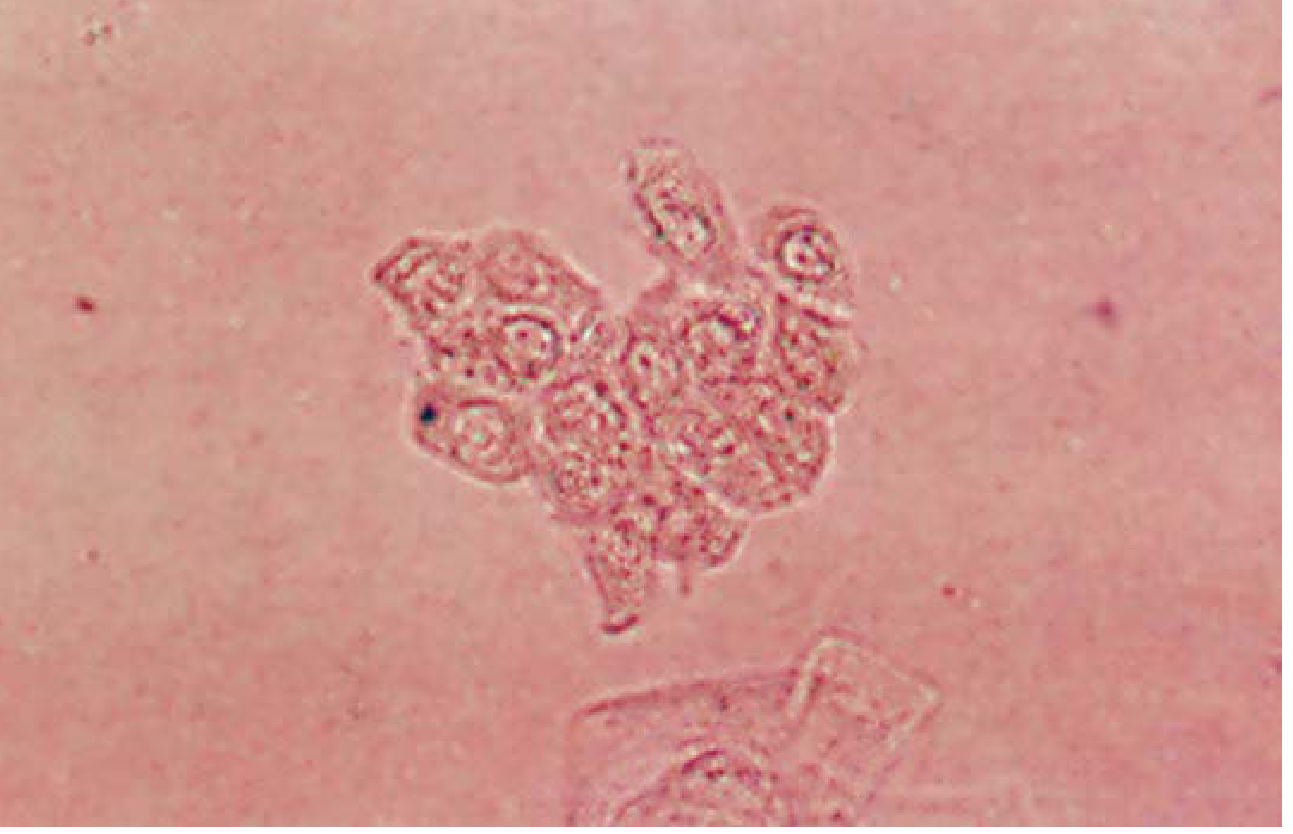
Fig. 29.11 - Renal tubular epithelial cells and neutrophils, Papanicolaou stained:
(Larger epithelial cells with prominent nuclei alongside smaller neutrophils)
Quick Comparison Table
| Cell Type | Size | Key Feature | Normal Limit | Significance |
|---|---|---|---|---|
| Neutrophil | ~12 μm | Multilobed nucleus, granular | < 5/hpf | Infection, inflammation |
| Eosinophil | ~12-15 μm | Bilobed, requires special stain | Absent | Drug hypersensitivity nephritis |
| Lymphocyte | ~8-10 μm | Small, dark round nucleus | Few | Chronic inflammation, rejection |
| Squamous epithelial | Large (40+ μm) | Flat, abundant cytoplasm, small nucleus | Few | Contamination marker |
| Transitional epithelial | 40-200 μm | Pear-shaped, endo-ecto rim | Few | Sheets = r/o malignancy |
| Renal tubular epithelial | 12-60 μm | Granular cytoplasm, eccentric nucleus | Rare | Tubular injury (ATN) |
Practical Tips
- Examine urine fresh - cells lyse within 2 hours at room temperature
- Refrigerate (2-8°C) to preserve cells if delay is unavoidable
- Acetic acid helps differentiate degenerating neutrophils from tubular cells (enhances nuclear lobulation)
- Phase-contrast microscopy improves detection of hyaline casts and translucent structures
- Pyuria in hypotonic urine - use leukocyte esterase strip to confirm (cells lyse rapidly)
- Distinguishing neutrophils from RTECs in degenerating specimens can be aided by the peroxidase cytochemical reaction (neutrophils are peroxidase-positive)
Source: Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapter 29 - Examination of Urine Sediment



IMG-20260712-WA0002.jpg
+2 more
Possible differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have enough information to provide a thorough differential diagnosis. Here is the full analysis:
Differential Diagnosis - Silochna, 26F
Summary of Lab Findings
| Report | Finding | Value | Interpretation |
|---|---|---|---|
| Hb | 11.1 g/dL | Normal 12-18 | Mild anemia |
| BT/CT | Normal | Within range | Normal hemostasis |
| Blood group | O Positive | - | - |
| Blood sugar | 88.29 mg/dL | < 140 (random) | Normal |
| TSH | 2.07 µIU/mL | 0.35-5.60 | Normal (pregnancy ranges also printed - likely pregnant or peripartum) |
| Urine - Leukocytes | 2-3/HPF | < 5 normal | High normal / borderline |
| Urine - Epithelial cells | 2-3/HPF | < 5 normal | Present |
| Urine - everything else | NIL | - | No casts, no bacteria, no crystals |
Key Clinical Observations
Two important contextual clues:
- The referring doctor is Dr. Suman Budania (MS) - an MS surgeon, likely a gynecologist/obstetrician in the Bikaner context
- The TSH report includes pregnancy trimester reference ranges - strongly suggesting this patient is pregnant or recently postpartum
Differential Diagnoses
PRIMARY - Most Likely
1. Pregnancy with Physiological Changes
- TSH of 2.07 fits 2nd/3rd trimester normal range (0.20-3.00)
- Mild anemia (Hb 11.1) is very common in pregnancy - WHO defines anemia in pregnancy as Hb < 11 g/dL (she is borderline)
- Epithelial cells (2-3/HPF) and leukocytes (2-3/HPF) in urine are within normal limits and commonly seen in pregnancy due to increased vaginal secretions and urinary tract changes
- Blood sugar 88 mg/dL - normal, rules out gestational diabetes at this level
2. Urinary Tract Infection (UTI) / Asymptomatic Bacteriuria
- Leukocytes 2-3/HPF with epithelial cells is at the borderline of significance
- No bacteria, no casts, no RBCs = sterile pyuria pattern
- In pregnant women, asymptomatic bacteriuria occurs in 2-7% and can present with low-grade pyuria before frank infection
- Important: In female urine, epithelial cells at this level may represent contamination from vaginal/vulvar secretions rather than true pathology
- Culture and sensitivity should be done to confirm or rule out
3. Vulvovaginal Contamination (Specimen Collection Artifact)
- 2-3 squamous epithelial cells/HPF is the classic finding when midstream urine collection is inadequate, especially in women
- No bacteria, no casts, clear urine, no albumin - all favor contamination rather than true infection
- Very common in young females; repeat midstream clean-catch recommended
SECONDARY - Consider If Symptomatic
4. Iron Deficiency Anemia
- Hb 11.1 g/dL in a 26-year-old female - most common cause is iron deficiency (menstrual loss, dietary)
- If pregnant: increased iron demand is the most common cause
- Next step: serum ferritin, TIBC, peripheral smear
5. Anemia of Pregnancy (Dilutional)
- Plasma volume expands 40-50% in pregnancy while RBC mass expands only 20-30%
- Results in physiological dilutional anemia - Hb commonly falls to 10.5-11.5 g/dL
- Hb 11.1 fits perfectly with this pattern
6. Subclinical Hypothyroidism / Hashimoto's Thyroiditis (LOW probability)
- TSH 2.07 is normal - this diagnosis is unlikely
- However, the fact that TSH was ordered suggests clinical suspicion (fatigue, weight gain, hair loss)
- If symptoms persist, re-check TSH with Free T4
7. Chronic Pelvic Inflammatory Disease (PID) / Cervicitis
- Can cause sterile pyuria with epithelial cells without overt bacteriuria
- Referred by a surgeon/gynecologist supports this workup
- Would need pelvic exam, cervical swab for Chlamydia/gonorrhea
LOWER PROBABILITY (Rule Out)
| Condition | Why considered | Why less likely |
|---|---|---|
| Interstitial nephritis | Sterile pyuria | No RBCs, no casts, no proteinuria |
| Renal tuberculosis | Sterile pyuria in young adults | No RBCs, no systemic features noted |
| Urolithiasis | Can cause pyuria | No crystals, no hematuria |
| Cystitis (bacterial) | Pyuria | No bacteria on microscopy |
Recommended Next Steps
- Urine C&S (culture and sensitivity) - to confirm/exclude bacterial UTI
- Peripheral blood smear + serum ferritin - to characterize the anemia (iron deficiency vs. dilutional)
- Repeat urine R/M with proper midstream clean-catch - if epithelial cells disappear, it was contamination
- Confirm pregnancy status (if not already confirmed via clinical history)
- Obstetric ultrasound - if pregnant, for dating and fetal assessment
- If symptomatic for thyroid: Free T4
Bottom Line
The most likely overall picture in this 26-year-old female is pregnancy with:
- Physiological/iron deficiency anemia (Hb 11.1)
- Normal TSH
- Borderline pyuria + epithelial cells likely representing contamination OR early/asymptomatic UTI - urine culture is the key next step
The urine findings (2-3 leukocytes, 2-3 epithelial cells/HPF, no bacteria, no casts) are not diagnostic of active infection on microscopy alone and a culture is needed before treating.
⚠️ Note: This analysis is for educational/clinical support purposes. Final diagnosis must be made by the treating physician with full clinical history, examination findings, and symptom correlation.
This is a shared conversation. Sign in to Orris to start your own chat.