explain me 10 common heart diseases with ecg changes and ecg images of those diseases.
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram myocardial infarction ST elevation
Finding Sources
Searching Images
ECG atrial fibrillation irregular rhythm absent P waves
Searching Images
ECG complete heart block third degree AV block
Searching Images
ECG left ventricular hypertrophy high voltage QRS
Searching Images
ECG Wolff-Parkinson-White syndrome delta wave pre-excitation
Searching Images
ECG hyperkalemia peaked T waves wide QRS
Searching Images
ECG pericarditis diffuse ST elevation saddle shape PR depression
Searching Images
ECG pulmonary embolism right heart strain S1Q3T3 pattern
Searching Images
ECG ventricular tachycardia wide complex tachycardia
Searching Images
ECG dilated cardiomyopathy left bundle branch block poor R wave progression
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings summary
Here is a comprehensive overview of 10 common heart diseases with their ECG changes and representative ECG images.
10 Common Heart Diseases: ECG Changes & Images
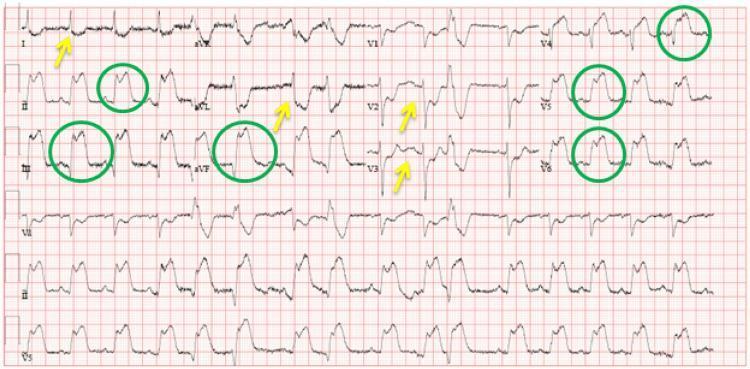
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes:
- Hyperacute T waves (earliest sign — tall, peaked, asymmetric)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Pathological Q waves (>40 ms wide, >25% of R wave height) — develop hours later
- Reciprocal ST depression in opposing leads
- T-wave inversion in evolving phase
- Lead localization: Anterior (V1–V4 = LAD), Inferior (II, III, aVF = RCA), Lateral (I, aVL, V5–V6 = LCx)

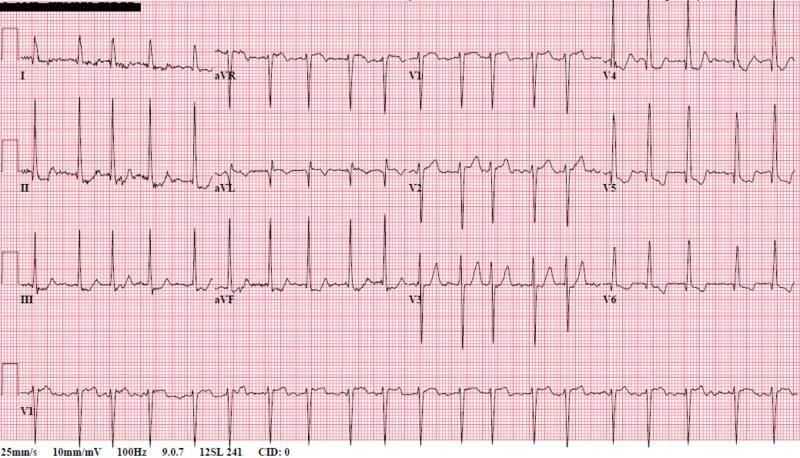
2. 💓 Atrial Fibrillation (AF)
ECG Changes:
- Absent P waves — replaced by chaotic fibrillatory baseline (f-waves), best seen in V1
- Irregularly irregular R-R intervals — hallmark finding
- QRS complexes are narrow (unless aberrant conduction or accessory pathway)
- Rate may be rapid (>100 bpm = AF with RVR) or controlled
- May show left ventricular hypertrophy voltage criteria in underlying hypertensive disease
3. 🔌 Third-Degree (Complete) Heart Block
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes are independent, with no relationship
- Atrial rate faster than ventricular rate
- Ventricular escape rhythm — rate 20–40 bpm (infra-Hisian) or 40–60 bpm (junctional)
- Wide QRS if ventricular escape; narrow QRS if junctional (nodal) escape
- P waves "march through" the QRS complexes and T waves

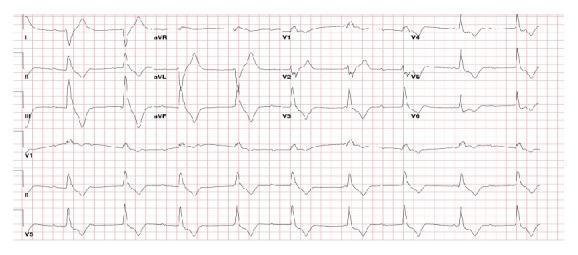
4. ❤️🔥 Acute Pericarditis
ECG Changes:
- Diffuse concave "saddle-shaped" ST elevation — in virtually all leads except aVR and V1
- PR-segment depression (atrial inflammation) — most evident in lead II; reciprocal PR elevation in aVR
- Spodick's sign — downward-sloping TP segment
- No reciprocal ST depression (unlike STEMI) — key differentiator
- Later: T-wave inversion after ST normalization, then return to baseline

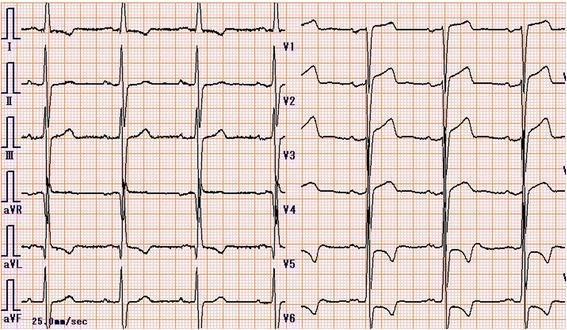
5. 🩺 Left Ventricular Hypertrophy (LVH)
Causes: Hypertension, aortic stenosis, hypertrophic cardiomyopathy
ECG Changes:
- High-voltage QRS: Sokolow-Lyon criteria — S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria — R in aVL + S in V3 >28 mm (men) / >20 mm (women)
- Left axis deviation
- Left atrial enlargement — broad notched P wave in II (P mitrale), biphasic in V1
- Strain pattern — ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- QRS complexes may overlap on adjacent leads ("Seamens sign")
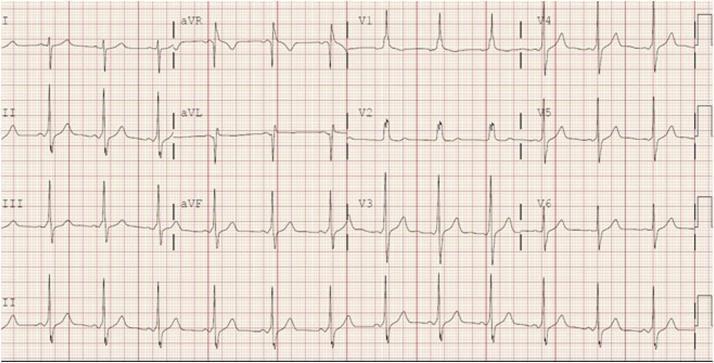
6. ⚡ Wolff-Parkinson-White (WPW) Syndrome
ECG Changes:
- Short PR interval (<120 ms) — due to bypass of AV node via accessory pathway (Bundle of Kent)
- Delta wave — slurred upstroke at the start of the QRS complex
- Wide QRS complex (>120 ms) — fusion of delta wave + normal conduction
- Secondary ST-T changes — discordant to QRS direction
- Pseudo-infarct Q waves — negative delta waves may mimic Q waves (esp. inferior leads)
- Risk of life-threatening tachycardia if AF develops with rapid pre-excited conduction

7. 🫁 Pulmonary Embolism (PE)
ECG Changes:
- Sinus tachycardia — most common finding
- S1Q3T3 pattern — deep S wave in I, Q wave in III, inverted T in III (McGinn-White sign)
- Right bundle branch block (RBBB) — complete or incomplete; rSR' in V1
- Right axis deviation
- T-wave inversions V1–V4 — right ventricular strain
- P pulmonale — tall peaked P wave in inferior leads
- Rarely: atrial fibrillation, RBBB with right heart strain


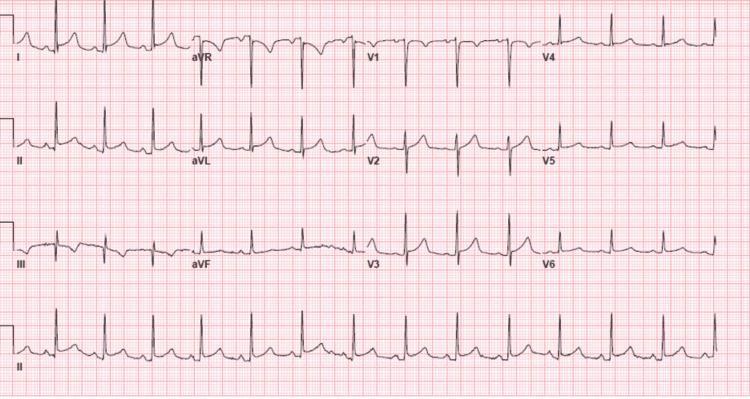
8. 💊 Hyperkalemia
Seen in: Renal failure, Addison's disease, ACE inhibitor/potassium-sparing diuretic use
ECG Changes (progressive with rising K⁺):
| K⁺ Level | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, narrow, peaked "tent" T waves |
| 6.5–7.5 mEq/L | PR prolongation, P wave flattening/disappearance |
| 7.0–8.0 mEq/L | QRS widening (>120 ms) |
| >8.0 mEq/L | Sine-wave pattern, ventricular fibrillation, asystole |
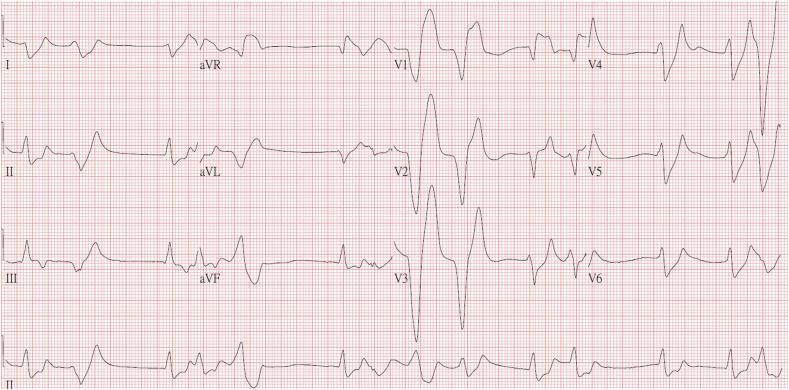
9. 🫀 Dilated Cardiomyopathy (DCM)
ECG Changes:
- Left bundle branch block (LBBB) — QRS >120 ms, broad notched R in I/aVL/V5–V6, deep S in V1–V3
- Poor R-wave progression across precordial leads
- Left ventricular hypertrophy voltage criteria
- Non-specific ST-T changes — secondary to conduction abnormality
- Atrial fibrillation — common in advanced DCM
- Ventricular ectopy / ventricular tachycardia — due to myocardial scarring
- Prolonged QRS is associated with worse prognosis and may indicate need for CRT


10. ⚡ Ventricular Tachycardia (VT)
ECG Changes:
- Wide QRS complex tachycardia (QRS ≥120 ms) at rate >100 bpm
- AV dissociation — P waves marching independently through wide QRS (pathognomonic)
- Fusion beats and capture beats (confirm VT vs SVT with aberrancy)
- Concordance — all precordial leads either all positive or all negative (positive concordance = VT)
- Northwest axis (extreme axis deviation)
- Monomorphic VT — identical QRS morphology; Polymorphic VT/Torsades — twisting QRS axis
Brugada criteria and Vereckei algorithm help differentiate VT from SVT with aberrancy.

Summary Table
| # | Disease | Key ECG Findings |
|---|---|---|
| 1 | STEMI | ST elevation (convex), Q waves, reciprocal depression |
| 2 | Atrial Fibrillation | No P waves, irregularly irregular RR |
| 3 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 4 | Acute Pericarditis | Diffuse saddle ST ↑, PR depression, Spodick's sign |
| 5 | LVH | High voltage, lateral strain pattern, left axis |
| 6 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 7 | Pulmonary Embolism | Sinus tach, S1Q3T3, RBBB, T inversions V1–V4 |
| 8 | Hyperkalemia | Peaked T waves → wide QRS → sine wave |
| 9 | Dilated Cardiomyopathy | LBBB, poor R progression, AF, ventricular ectopy |
| 10 | Ventricular Tachycardia | Wide complex tach, AV dissociation, concordance |
Clinical pearl: Always interpret the ECG in the context of the clinical presentation. Many ECG changes overlap between conditions (e.g., diffuse ST elevation in STEMI vs pericarditis), and the history, physical exam, and troponin levels are essential for correct diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.