Systometrometrogrm
The term "Systometrometrogrm" doesn't match any recognized medical, scientific, or technical term I'm aware of. It may be a typo or misspelling.
Did you mean one of these?
- Hysterosalpingogram (HSG) - an X-ray procedure to examine the uterus and fallopian tubes
- Hysterogram - imaging of the uterine cavity
- Cystometrogram (CMG) - a urodynamic test measuring bladder pressure and function
- Salpingogram - imaging of the fallopian tubes
Could you clarify what you were looking for? If it's a specific medical test, procedure, or condition, feel free to rephrase and I'll give you a detailed answer.
Cmg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough explanation of the Cystometrogram (CMG):
Cystometrogram (CMG)
Definition
A cystometrogram is a graphical record of the relationship between intravesical (bladder) pressure (cm H₂O) and bladder volume (mL) during bladder filling. It is obtained by the procedure called cystometry: a catheter is inserted through the urethra, the bladder is emptied, and then filled with 50 mL increments of water or air while intravesical pressure is continuously recorded.
- Ganong's Review of Medical Physiology, 26th ed.
The Normal CMG Curve - Three Segments
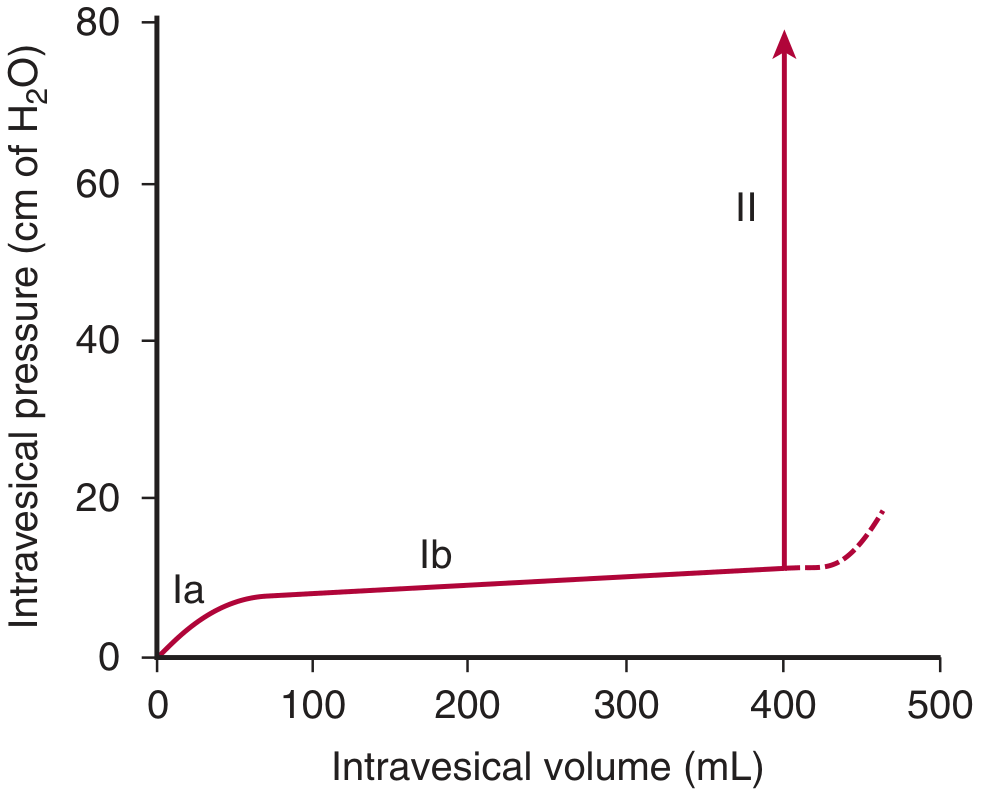
Normal cystometrogram (Ganong's Review of Medical Physiology, 26th ed.) showing the three segments.
| Segment | Description | Volume Range |
|---|---|---|
| Ia | Initial slight rise in pressure as first increments of urine enter the empty bladder | 0-50 mL |
| Ib | Long, nearly flat segment - bladder accommodates large volumes with minimal pressure rise ("tonic" compliance) | 50-400 mL |
| II | Sudden, sharp rise in pressure as the micturition reflex is triggered and voiding occurs | >400 mL |
The flatness of segment Ib is explained by the Law of Laplace: Pressure = 2T/r. As the bladder fills, both wall tension (T) and radius (r) increase together, so the net pressure change stays small.
Key Sensory Thresholds (Normal)
- First urge to void: ~150 mL
- Marked sense of fullness: ~400 mL
- Bladder capacity before micturition reflex triggers: 300-400 mL (Guyton & Hall)
Micturition Waves (Superimposed Spikes)
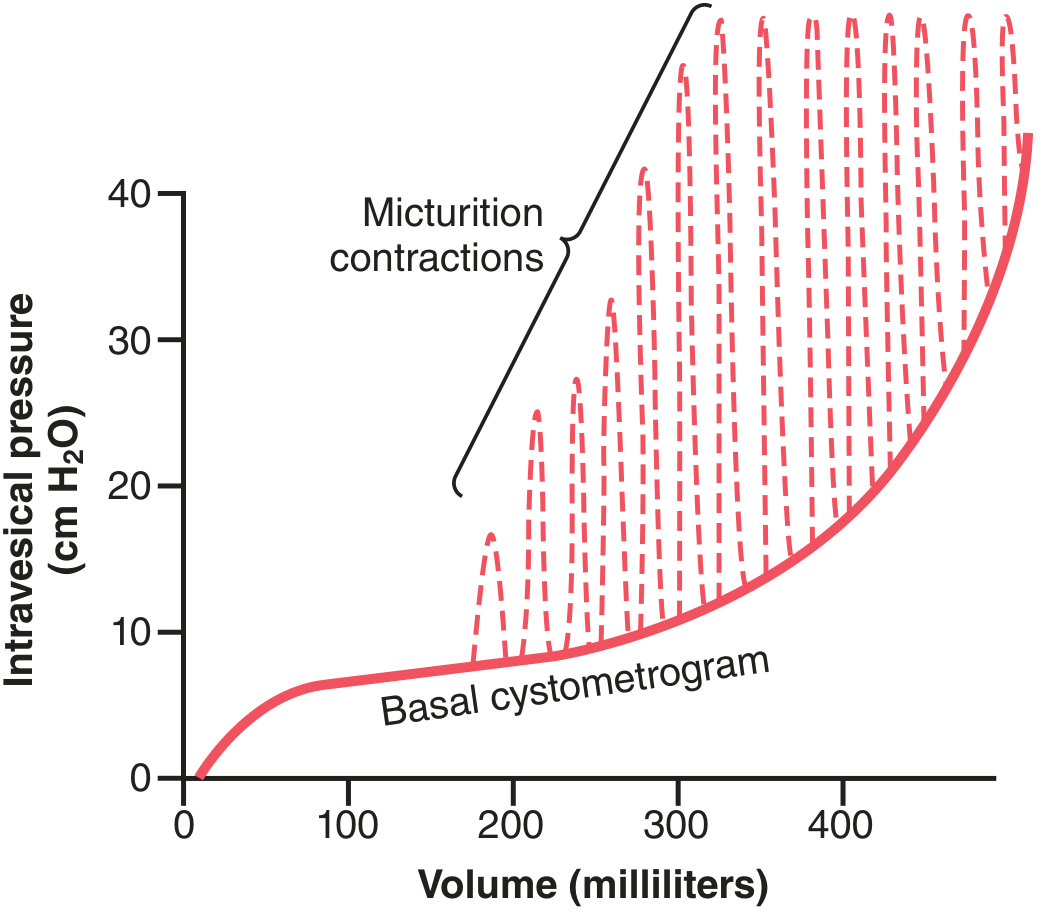
Normal CMG with superimposed micturition contractions (dashed spikes) - Guyton & Hall Textbook of Medical Physiology.
Superimposed on the basal CMG curve are periodic acute pressure spikes (micturition waves) caused by the micturition reflex:
- These arise from stretch receptors in the bladder wall and posterior urethra
- They last seconds to >1 minute
- Pressure may rise only a few cm H₂O, or >100 cm H₂O
- They become more frequent and forceful as the bladder fills
- If voiding is suppressed, the reflex self-regenerates briefly then fatigues, with pressure returning to baseline until the next stretch stimulus
Micturition Reflex (Underlying Physiology)
- Bladder filling activates stretch receptors in the detrusor wall and posterior urethra
- Afferent signals travel via pelvic nerves to the sacral spinal cord (S2-S4)
- The Pontine Micturition Center (PMC) coordinates voiding; higher cortical centers normally inhibit it until voiding is socially appropriate
- When voiding is initiated: external urethral sphincter relaxes first → internal sphincter relaxes → parasympathetic activation contracts the detrusor muscle → urine expelled
- The micturition reflex is self-regenerating (initial contraction activates more stretch receptors → stronger contraction), until the bladder empties
- Medical Physiology (Boron & Boulpaep)
Types of CMG Studies
| Type | What is Measured |
|---|---|
| Filling CMG | Pressure/volume relationship during bladder filling (storage phase) |
| Voiding CMG (VCMG) | Total bladder, detrusor, and abdominal pressures during voiding |
| Complex urodynamics | CMG + urethral pressure profilometry + EMG + fluoroscopy |
- Campbell-Walsh-Wein Urology
Clinical Applications
| Condition | CMG Finding |
|---|---|
| Detrusor overactivity (OAB) | Involuntary pressure spikes during filling at low volumes |
| Neurogenic bladder (upper motor neuron lesion) | Hyperreflexic, high-pressure contractions |
| Flaccid/decentralized bladder (lower motor neuron) | Flat, low-pressure curve; no reflex contractions |
| Reduced compliance | Steep rise in pressure during filling (e.g., radiation cystitis, fibrosis) |
| Obstruction (BPH) | Differentiates obstructive vs. functional cause of voiding dysfunction |
- Comprehensive Clinical Nephrology, 7th ed.
CPT Billing Codes (USA)
-
51725 - Simple CMG (e.g., spinal manometer)
-
51726 - Complex CMG (calibrated electronic equipment)
-
Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.
Summary: The CMG is a fundamental urodynamic tool that plots bladder pressure against volume. The normal curve has three characteristic segments (Ia, Ib, II), with the key feature being the flat "tonic" Ib segment reflecting bladder compliance. It is used clinically to diagnose detrusor overactivity, neurogenic bladder, and other voiding disorders.
This is a shared conversation. Sign in to Orris to start your own chat.