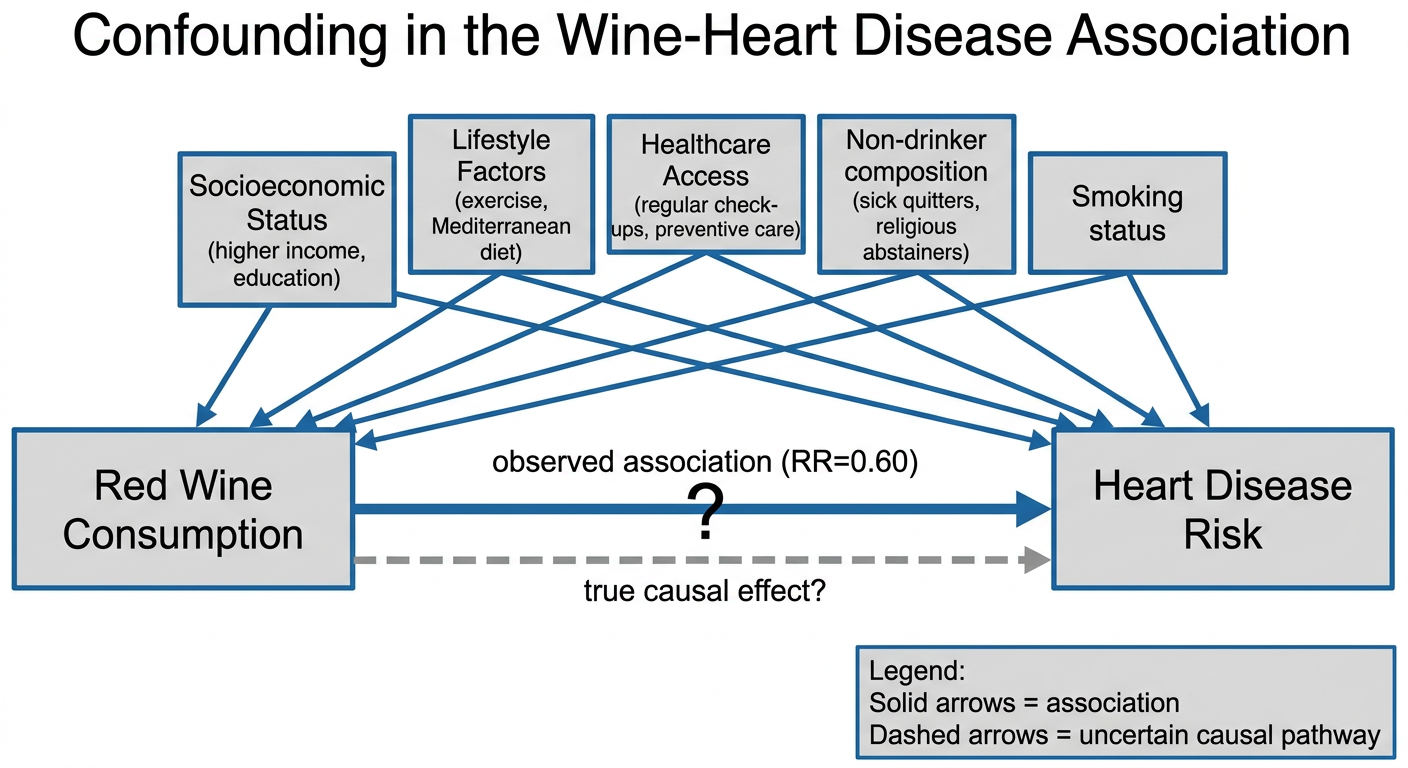
Dr Amandeep Singh, a cardiologist at a major teaching hospital, is reviewing a recently published cohort study that followed 50,000 adults for 15 years. The study found that people who drink 1-2 glasses of red wine daily have a 40% lower risk of heart disease compared to non-drinkers (RR=0.60, 95% CI: 0.45-0.80, p<0.001). The local media has picked up the story with headlines like "Red Wine: The Heart-Healthy Choice Doctors Recommend". However, Dr Singh notices some concerning patterns in the baseline characteristics table. Wine drinkers were more likely to be college-educated (78% vs 45%); have higher incomes (median £65,000 vs £35,000); exercise regularly (65% vs 32%); eat Mediterranean-style diets (71% vs 28%); and have regular healthcare check-ups (89% vs 54%). Non-drinkers included a higher proportion of former alcoholics (23%) and people with religious/cultural prohibitions against alcohol (31%). Dr Singh is now questioning whether red wine truly protects against heart disease or whether other factors might explain this association. I'd like the group to identify potential confounders in this scenario and explain your reasoning. What variables might be associated with both wine consumption and heart disease risk? Please bring evidence from your clinical experience to support your discussion of how these factors might operate. Let's explore the concept of confounding more deeply. Can you construct a simple diagram showing the relationships between wine consumption, the potential confounders you've identified, and heart disease outcomes? I want the group to consider: what makes a variable a true confounder versus just a risk factor? Now I'd like you to discuss what methods the researchers could have used at the design stage to control for these confounders. What are the advantages and limitations of each approach in this specific scenario? Please consider the practical implications for conducting such a study. Finally, let's consider the analysis stage. The authors reported they 'adjusted for age, sex, and smoking status'. Based on your confounding analysis, is this sufficient? What additional variables would you want to see included in a multivariable model, and why? I want the group to think about the concept of residual confounding – can we ever control for everything? The following article could help you: Hernán, M.A. and Robins, J.M. (2020) 'Confounding', in Causal Inference: What If. Boca Raton: Chapman & Hall/CRC, Chapter 7. Available at: https://static1.squarespace.com/static/675db8b0dd37046447128f5f/t/677676888e31cc50c2c33877/1735816881944/hernanrobins_WhatIf_2jan25.pdf
confounding confounder definition adjustment control methods
"alcohol" AND "cardiovascular disease" AND "confounding"
"alcohol" AND "healthy user bias" AND "cardiovascular"
"sick quitter" OR "abstainer bias" AND alcohol cardiovascular
"Mendelian randomization" AND alcohol AND "cardiovascular disease"
sick quitter bias abstainer bias alcohol cardiovascular studies healthy user bias evidence 2023 2024
Confounding in Observational Research: The Red Wine & Heart Disease Case
PART 1 — Identifying the Potential Confounders
What Is a Confounder?
The Confounders in This Study
| Variable | Associated with wine drinking? | Associated with heart disease? | Not on causal pathway? |
|---|---|---|---|
| Socioeconomic status (income, education) | Yes — 78% vs 45% college-educated; £65k vs £35k income | Yes — higher SES → better housing, nutrition, lower occupational stress, less financial strain | Yes |
| Regular exercise | Yes — 65% vs 32% | Yes — exercise reduces CV risk by 35–50% (reduces BP, improves lipid profiles, reduces insulin resistance) | Yes |
| Mediterranean diet | Yes — 71% vs 28% | Yes — strong independent protection against CVD (PREDIMED trial data) | Yes |
| Healthcare access | Yes — 89% vs 54% regular check-ups | Yes — earlier detection of hypertension, dyslipidaemia, diabetes | Yes |
| Smoking status | Likely — wine drinkers may have different smoking patterns | Yes — major independent CV risk factor | Yes |
| Non-drinker composition: "sick quitters" | Yes — 23% of non-drinkers are former alcoholics | Yes — former heavy drinkers have residual CV and hepatic damage | Not applicable (selection bias subtype) |
| Religious/cultural abstainers | Yes — 31% of non-drinkers | Varies — some cultural groups have higher/lower baseline CV risk | Not applicable |
The "Sick Quitter" / "Abstainer Bias" Problem
Confounder vs. Risk Factor: A Critical Distinction
- Age — if age is associated with both wine preference and heart disease and is not mediated by wine: confounder ✓
- LDL cholesterol — if wine itself lowers LDL as part of its mechanism, adjusting for LDL would block the very causal pathway you're trying to study (this is an intermediate variable or mediator), and adjusting for it would introduce bias, not remove it. Hernán & Robins are explicit: "confounders cannot be descendants of treatment" — adjusting for intermediaries blocks causal paths and produces incorrect estimates.
PART 2 — Confounding Diagram (DAG)
PART 3 — Design-Stage Methods to Control Confounding
A. Randomisation
- Ethically problematic — you cannot randomise people to consume alcohol daily for 15 years
- Practically impossible for a 15-year follow-up
- Compliance issues: randomised participants may not adhere to assigned alcohol levels
- Blinding is essentially impossible (participants know whether they're drinking wine)
B. Restriction
- Severely limits generalisability (external validity)
- Cannot restrict on all potential confounders simultaneously without making the study population impossibly small from 50,000 participants
- Restricting on SES or lifestyle would make the sample unrepresentative of the general population
C. Matching
- Difficult to match on more than 4–5 variables simultaneously
- With 50,000 participants and many confounders (SES, diet, exercise, healthcare access, religion, prior alcohol history), many participants would be unmatchable and excluded, reducing power and introducing selection bias
- Cannot match on unmeasured variables
D. Stratification at Design Stage
Practical Recommendation for This Study
PART 4 — Analysis-Stage Adjustment and Residual Confounding
Is Adjustment for Age, Sex, and Smoking Sufficient?
| Unadjusted Confounder | Why It Matters |
|---|---|
| SES (income + education) | Both independently predict heart disease through multiple pathways (diet, housing, stress, access to care) |
| Physical activity | 65% vs 32% exercise rates — a massive imbalance with direct, strong CV protection |
| Mediterranean diet | 71% vs 28% — PREDIMED data shows ~30% CV risk reduction independent of other factors |
| Healthcare utilisation | 89% vs 54% — earlier hypertension and diabetes detection in wine drinkers |
| Non-drinker composition | Combining sick quitters (23%) and religious abstainers (31%) with healthy never-drinkers creates a biased reference group |
What a Multivariable Model Should Include
- Age and sex (already done)
- Smoking (already done)
- Physical activity (quantified — MET-hours/week)
- Dietary pattern (Mediterranean diet score or fruit/vegetable intake)
- SES composite (income + education as separate terms or an index)
- Healthcare access (frequency of GP visits, insurance status)
- Non-drinker subtype (lifetime abstainer vs. former drinker vs. health-restricted) — this is not adjustment but rather reference group redefinition
- Comorbidities at baseline (BMI, pre-existing hypertension, diabetes, dyslipidaemia)
- Social support / marital status (independent CV predictors often correlated with moderate drinking)
The Concept of Residual Confounding
-
Measurement error in covariates — SES measured at a single point misses lifetime trajectory; diet questionnaires are imprecise; exercise is self-reported. Imperfect measurement of a confounder means imperfect adjustment.
-
Unknown and unmeasured confounders — We cannot adjust for what we have not measured. Genetic predispositions (e.g., ALDH2 variants affecting alcohol metabolism), personality traits, social network quality, and childhood exposures may all confound the relationship.
-
Time-varying confounding — Confounders may change over 15 years. Someone who starts exercising at year 5 and starts wine drinking at year 3 creates time-dependent confounding that standard regression cannot handle.
-
Granularity of adjustment — Adjusting for "exercise" as a binary yes/no is far less effective than a continuous quantitative measure. Coarse categorisation leaves within-category confounding.
Advanced Analysis Approaches Available
| Method | Advantage | Limitation |
|---|---|---|
| Multivariable regression | Simple, interpretable | Cannot handle unmeasured confounders |
| Propensity score matching/weighting | Balances many confounders simultaneously; intuitive | Still only adjusts for measured variables |
| Instrumental variable analysis | Can address unmeasured confounding if a valid instrument exists | Valid instruments for alcohol consumption are rare; alcohol-related genetic SNPs (e.g., ADH1B, ALDH2) can serve as instruments in Mendelian randomisation |
| Mendelian randomisation | Uses genetic variants as "natural experiments"; randomises at conception so unmeasured lifestyle confounders are not inherited | Assumes genetic variant affects outcome only through the exposure (exclusion restriction); pleiotropy is a concern |
| Difference-in-differences | Can adjust for unmeasured time-stable confounders | Requires pre/post data; strong assumptions about parallel trends |
| Negative control outcomes | Tests whether the exposure affects an outcome with no plausible biological mechanism (if it does, confounding is present) | Requires identifying a credible negative control |
Summary for Dr Singh's Group
- Wine drinkers are systematically healthier, wealthier, better educated, more physically active, better fed, and better engaged with healthcare
- The non-drinker reference group is diluted with former alcoholics and health-restricted abstainers who are systematically sicker
- Adjustment for only age, sex, and smoking leaves the vast majority of confounding uncorrected
- When Mendelian randomisation is used to approximate an unconfounded estimate, the apparent cardioprotective effect disappears and in some analyses reverses
- Goldman-Cecil Medicine, 28th ed. (confounding, multivariable statistics)
- Miller's Anaesthesia, 10e (confounding in research design)
- Hernán MA & Robins JM (2020). Causal Inference: What If, Chapter 7 — confounding, DAGs, backdoor paths, conditional exchangeability
- Krittanawong C et al. (2022). Alcohol Consumption and Cardiovascular Health. Am J Med. [PMID: 35580715]
- Biddinger KJ et al. (2022). Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw Open. [PMID: 35333364]
- Larsson SC et al. (2020). Alcohol Consumption and Cardiovascular Disease: A Mendelian Randomization Study. Circ Genom Precis Med. [PMID: 32367730]