Hepatic encephalopathy management
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Hepatic Encephalopathy (HE) - Management
Definition and Scope
Hepatic encephalopathy (HE) encompasses a wide array of transient, reversible neurologic and psychiatric manifestations in patients with chronic liver disease and portal hypertension, or acute liver failure (ALF). It develops in 50-70% of patients with cirrhosis. Once overt HE occurs, prognosis is poor - 1-year and 3-year survival rates are approximately 42% and 23%, respectively, without liver transplantation.
Pathophysiology
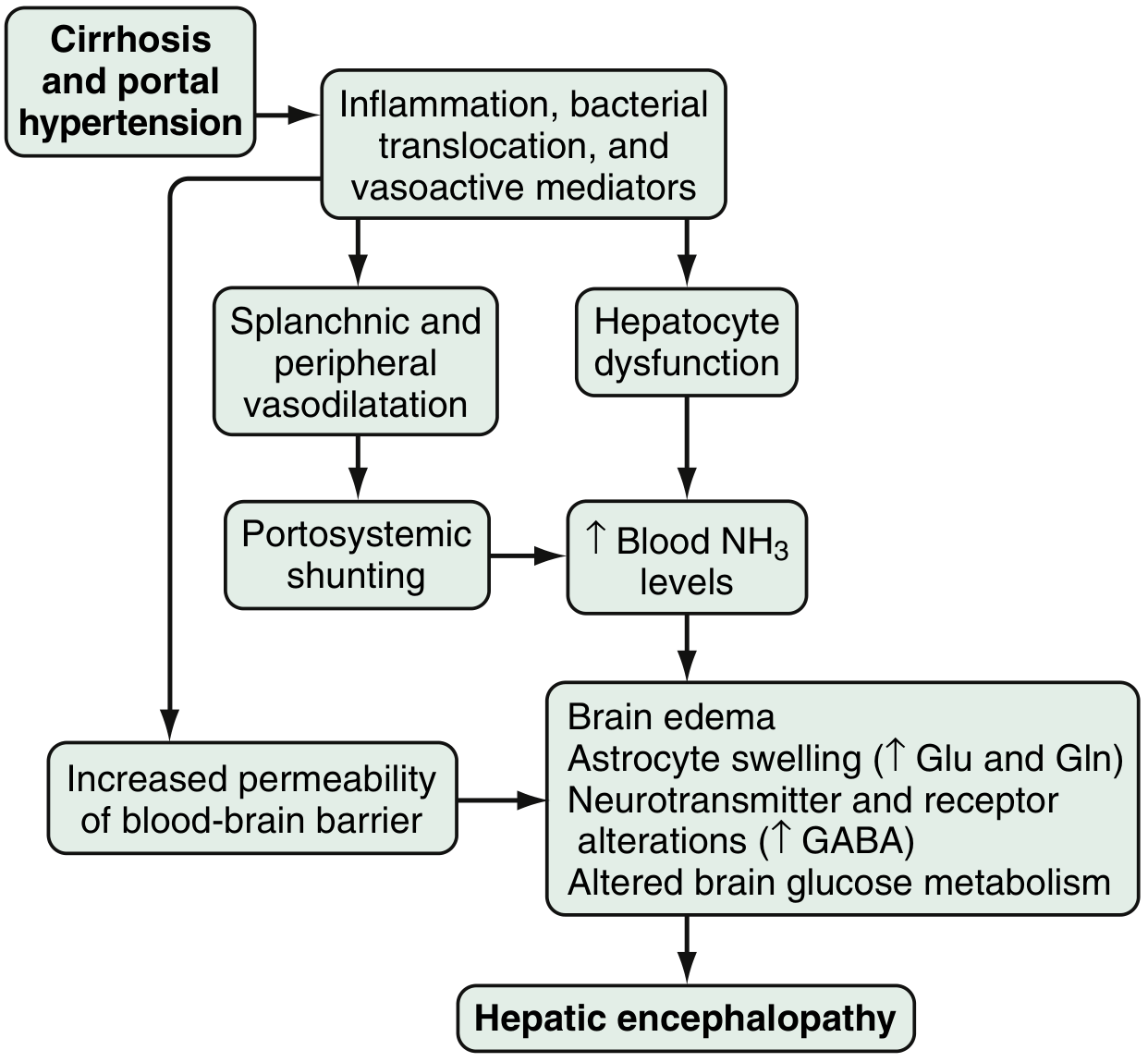
The key mechanisms involve:
- Ammonia toxicity: Produced in the colon from bacterial metabolism of proteins; in cirrhosis, reduced hepatocyte function and portosystemic shunting allow ammonia to accumulate in the bloodstream. Arterial hyperammonemia is present in up to 90% of HE patients.
- Astrocyte swelling: Hyperammonemia causes astrocyte glutamine accumulation via glutamine synthetase, leading to cytotoxic brain edema.
- GABA-benzodiazepine system activation: Enhanced sensitivity of astrocyte (peripheral-type) benzodiazepine receptors potentiates GABA-A-mediated inhibition, partly via neurosteroid production (allopregnanolone, tetrahydrodeoxycorticosterone).
- Blood-brain barrier disruption: Increases cerebral uptake of ammonia and other neurotoxins.
- Other contributors: Serotonin, nitric oxide, opioid peptides, manganese, and inflammatory mediators from bacterial translocation.
Classification
| Feature | Type |
|---|---|
| Underlying disease | Type A (acute liver failure), Type B (portosystemic bypass), Type C (cirrhosis - most common) |
| Severity | Covert/minimal HE (subclinical) vs. Overt HE (West Haven Grade I-IV) |
| Time course | Episodic, Recurrent (>2 episodes within 6 months), Persistent |
| Spontaneous vs. precipitated | Based on presence/absence of a triggering event |
Common Precipitating Factors
Identifying and correcting precipitants is the cornerstone of management:
- GI bleeding (most common)
- Infection / spontaneous bacterial peritonitis (SBP)
- Overdiuresis / dehydration / hypokalemia / hyponatremia
- Constipation
- High oral protein load (especially animal protein)
- Sedatives, narcotics, benzodiazepines
- TIPS (transjugular intrahepatic portosystemic shunt) - may require shunt reduction
- Renal failure
- Non-compliance with lactulose
Treatment Framework
1. Step 1 - Identify and Treat Precipitants (Always First)
This alone may be sufficient to resolve an episode of HE. Correct infections with antibiotics, replace volume, treat GI bleeding, stop offending medications, and address constipation.
2. Ammonia-Lowering Therapy
Lactulose (First-Line)
Lactulose is the cornerstone of treatment. It works by:
- Cathartic action - removes dietary and endogenous sources of ammonia
- Lowering colonic pH - inhibits ammonia absorption and reduces urease-producing bacteria population
- Trapping ammonia as ammonium (NH4+) in the gut lumen
Dosing:
- Acute episode: 30 mL every 1-2 hours until bowel movements begin, then taper to every 4-6 hours
- Maintenance: 15-45 mL PO bid-qid, titrated to produce 2-3 soft stools per day (Washington Manual targets 3-5/day)
- Rectal enema: 300 mL lactulose + 700 mL distilled water for patients unable to take orally or at aspiration risk
Side effects: Flatulence, abdominal cramping, diarrhea, hypovolemia, hypernatremia. Avoid in ileus or bowel obstruction.
Polyethylene glycol (PEG) 3350: 4 L orally or via NG tube over 4 hours may produce a faster clinical response than lactulose in acute episodes (Goldman-Cecil Medicine).
Rifaximin (Second-Line / Adjunct)
A minimally absorbed, oral broad-spectrum antibiotic that concentrates in the gut. FDA-approved in 2010 for prevention of recurrence of overt HE.
- Dose: 550 mg PO twice daily
- Mechanism: Reduces ammonia-producing enteric gram-negative bacteria in the colon
- Evidence: In a placebo-controlled trial, rifaximin + lactulose reduced risk of HE recurrence by ~49.1% compared to lactulose alone and decreased time to first hospitalization over 6 months
- Indications:
- Recurrent HE: Add to lactulose
- Intolerance to lactulose: Use as monotherapy
- Failure to respond to lactulose alone within 48-72 hours
- Advantage: Superior tolerability and side-effect profile compared to lactulose (though at higher cost)
Other Antibiotics (Limited Use)
| Antibiotic | Dose | Note |
|---|---|---|
| Neomycin | 500 mg-1 g TID | Risk of ototoxicity and nephrotoxicity limits chronic use |
| Metronidazole | 250 mg 2-4x/day | Neurotoxicity with prolonged use; use short-term only |
| Vancomycin | Variable | Limited evidence; used in combination |
3. Dietary Management
- Protein restriction is NOT recommended - it is harmful and should not be used chronically; it worsens sarcopenia.
- Vegetable and dairy proteins are preferable to animal proteins (more favorable calorie-to-nitrogen ratio; lower ammoniagenic potential).
- Branched-chain amino acid (BCAA) supplementation (oral) may help in refractory/persistent HE but does not improve mortality.
- Small, frequent meals including a late-night snack help reduce catabolism.
- Total caloric intake: 35-40 kcal/kg/day; protein intake: 1.2-1.5 g/kg/day.
4. Emerging and Adjunct Agents
| Agent | Mechanism | Status |
|---|---|---|
| L-ornithine-L-aspartate (LOLA) | Activates urea cycle; promotes ammonia fixation | Studied; promising in some trials |
| Sodium benzoate / phenylbutyrate / glycerol phenylbutyrate | Increase urinary ammonia excretion; alternative nitrogen pathways | FDA-approved for urea cycle defects; being studied in cirrhosis |
| Zinc supplementation | Zinc deficiency is common in cirrhosis; zinc activates ornithine transcarbamylase in the urea cycle | Limited evidence |
| Probiotics | Modify intestinal flora; reduce ammonia generation | Cochrane review: probably improves overt HE, quality of life, and plasma ammonia; no mortality benefit |
| Acarbose | Alpha-glucosidase inhibitor; shifts colonic flora toward saccharolytic species | RCT showed benefit in mild HE with type 2 diabetes |
| MARS (Molecular Adsorbent Recirculating System) | Extracorporeal albumin dialysis | Reduces blood ammonia in acute-on-chronic liver failure; bridge to transplant |
5. Secondary Prophylaxis
Once an episode of overt HE resolves:
- Lactulose secondary prophylaxis is recommended indefinitely after the first episode
- Rifaximin + lactulose for recurrent HE (2+ episodes)
- Prophylaxis may be discontinued if a precipitant is clearly identified and well-controlled, or if liver function improves
- Switching from animal to vegetable protein source is reasonable for recurrent/persistent HE
6. Management of Refractory HE / Special Situations
- TIPS-related HE: Shunt reduction or occlusion may be required
- ALF with cerebral edema: More aggressive management including ICP monitoring, mannitol, hypertonic saline, and mechanical ventilation
- Sedation avoidance: Minimize benzodiazepines and narcotics; if reversal is needed, flumazenil may transiently improve HE but does not alter outcomes
7. Liver Transplantation
The definitive treatment for HE. LT generally fully reverses HE. Consider when:
- Child-Pugh score ≥ 7, or MELD/MELD-Na score ≥ 15
- Recurrent or persistent HE despite maximal medical management
- HE as part of overall decompensated cirrhosis
Summary Algorithm
Acute Overt HE
│
├─► Identify & treat precipitants (bleeding, infection, electrolytes, meds)
│
├─► Lactulose (30 mL q1-2h acute → titrate to 2-3 soft BM/day)
│ │
│ ├─ No improvement → Add rifaximin 550 mg PO bid
│ │
│ └─ Unable to take PO → Lactulose enema OR PEG 3350
│
├─► Correct nutrition: vegetable/dairy protein preferred, NO protein restriction
│
├─► After resolution: Secondary prophylaxis (lactulose ± rifaximin)
│
└─► Recurrent/refractory → Evaluate for liver transplantation
Recent PubMed alert (2025): A systematic review and meta-analysis (PMID 40812534) found that proton pump inhibitor (PPI) use is associated with increased risk of HE in cirrhotic patients. Unnecessary PPIs should be reviewed and discontinued where clinically appropriate, as they may promote small intestinal bacterial overgrowth and alter gut flora.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Ch. 94) | Goldman-Cecil Medicine | Washington Manual of Medical Therapeutics | Symptom to Diagnosis (4th ed.) | Mulholland and Greenfield's Surgery (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.