Male patient came with hypokalemia, creatinine high does it indication cld or ckd
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Now I have enough information. Let me provide a comprehensive clinical answer.
Hypokalemia + Elevated Creatinine: CLD vs. CKD?
This combination does not clearly point to one diagnosis alone — both CLD (chronic liver disease/cirrhosis) and CKD can produce this picture, but through different mechanisms. Here is a structured breakdown:
1. Why Both Can Cause Hypokalemia
In CLD (Cirrhosis):
- Secondary hyperaldosteronism: Portal hypertension → splanchnic vasodilation → reduced effective circulating volume → RAAS activation → aldosterone-driven urinary K⁺ wasting
- Diuretic therapy (furosemide, spironolactone) for ascites — loop diuretics in particular cause significant kaliuresis
- Vomiting, poor intake, alcoholism — common in cirrhotic patients
- AVP (vasopressin) release from circulatory dysfunction → stimulates K⁺ secretion in the distal tubule
- Hypomagnesemia (common in cirrhosis) → impairs K⁺ reabsorption
"Hyponatremia and hypokalemia are common... patients with cirrhosis and ascites have avid renal sodium and water retention" — Morgan & Mikhail's Clinical Anesthesiology
In CKD:
- Early/moderate CKD: Hypokalemia can occur with tubular dysfunction, diuretic use, or poor intake
- Hypokalemic nephropathy: Chronic hypokalemia → renal interstitial fibrosis → can itself cause or worsen CKD
- However, hyperkalemia is far more characteristic of advanced CKD (GFR <20 mL/min) due to reduced distal K⁺ secretion
"Chronic hypokalemia can lead to renal interstitial fibrosis and development of chronic kidney disease" — Comprehensive Clinical Nephrology, 7th Ed.
2. Why Both Can Cause Elevated Creatinine
In CKD:
- Creatinine rises directly due to reduced GFR — this is the hallmark of CKD
- Rise is proportional to nephron loss
In CLD (Cirrhosis):
- Creatinine may be falsely low due to muscle wasting (less creatine substrate) and reduced hepatic creatinine production — this is a critical pitfall: creatinine underestimates true renal dysfunction in cirrhosis
- Despite this, creatinine rises when:
- Hepatorenal syndrome (HRS) develops — Type 1 (rapidly progressive) or Type 2 (slower); caused by renal vasoconstriction from systemic inflammation and hemodynamic alterations in advanced cirrhosis/ascites
- Aggressive diuresis causes prerenal azotemia
- Superimposed infection (SBP) triggers AKI
"Cirrhosis of the liver is often associated with renal failure as a result of the hepatorenal syndrome. Serum BUN and creatinine rise to markedly elevated levels" — Henry's Clinical Diagnosis
"An elevated serum creatinine level suggests acute or chronic renal failure, which can be intrinsic or occur with advanced heart failure (cardiorenal) or hepatic cirrhosis (hepatorenal failure)" — Goldman-Cecil Medicine
3. Key Differentiating Clues
| Feature | Favors CLD | Favors CKD |
|---|---|---|
| Potassium | Hypokalemia (aldosterone, diuretics) | Hyperkalemia (advanced), hypokalemia (early/tubular) |
| Creatinine | May be deceptively low; rises with HRS | Steadily elevated, reflects GFR loss |
| Liver markers | ↑ ALT/AST, ↑ bilirubin, ↑ PT/INR, ↓ albumin | Usually normal |
| Proteinuria | Minimal (unless HRS) | Significant (especially diabetic/hypertensive CKD) |
| Urinary Na⁺ | Very low (<10 mEq/L) in HRS | Usually >20 mEq/L in intrinsic CKD |
| Physical exam | Jaundice, ascites, spider angiomata, palmar erythema, gynecomastia | Pallor, edema, hypertension |
| Albumin | Low (↓ synthesis) | Low (urinary losses if nephrotic) |
| Sodium | Hyponatremia common | Variable |
| GFR estimate | Cystatin-C more reliable than creatinine | Creatinine-based eGFR adequate |
4. The Important Overlap: Cardiorenal-Hepatic Axis
In a male patient:
- CKD can cause secondary hypertension → liver congestion (not CLD but can mimic)
- CLD can cause HRS — which presents exactly as renal failure with hypokalemia (from prior diuresis)
- Primary aldosteronism must be excluded when spontaneous hypokalemia + hypertension + elevated creatinine coexist — this causes both hypokalemia AND CKD progression
Bottom Line
| CLD | CKD | |
|---|---|---|
| Hypokalemia | ✅ Very common (aldosterone, diuretics, poor intake) | ⚠️ Less common; hyperkalemia more typical in advanced disease |
| High creatinine | ✅ Via HRS (functional renal failure) or prerenal AKI | ✅ Direct marker (the hallmark finding) |
The combination of hypokalemia + elevated creatinine is more characteristic of CLD (especially cirrhosis with secondary hyperaldosteronism and/or hepatorenal syndrome), because in advanced CKD you would expect hyperkalemia rather than hypokalemia.
Workup to distinguish:
- LFTs, bilirubin, PT/INR, albumin (liver function)
- Urine Na⁺, fractional excretion of Na⁺ (FENa)
- Cystatin-C (more accurate GFR in cirrhosis)
- Urine protein/creatinine ratio
- Abdominal ultrasound (liver echotexture, ascites, splenomegaly, kidney size)
- Aldosterone/renin ratio (rule out primary aldosteronism)
Write me a long case of cld with these data
Here is a comprehensive long clinical case of Chronic Liver Disease incorporating hypokalemia and elevated creatinine:
Clinical Case: Chronic Liver Disease (CLD)
PATIENT IDENTIFICATION
Name: Mr. Ahmed Hassan
Age: 52 years
Sex: Male
Occupation: Retired laborer
Marital status: Married, 3 children
Residence: Rural area
Date of admission: May 2026
Referred by: Primary care physician
CHIEF COMPLAINTS
- Progressive abdominal distension — 4 months
- Bilateral leg swelling — 3 months
- Generalized weakness and fatigue — 2 months
- Yellowish discoloration of eyes and skin — 6 weeks
- Decreased urine output — 1 week
HISTORY OF PRESENTING ILLNESS
Mr. Ahmed Hassan, a 52-year-old male, was brought to the medicine ward by his family with a 4-month history of progressively worsening abdominal distension. Initially he noticed mild bloating after meals which he attributed to indigestion, but over the following weeks the abdomen became uniformly distended and tense, with visible prominence of the flanks. He reports a feeling of fullness and inability to eat a full meal. He required multiple increment changes in trouser size over these months.
Three months prior to admission, he developed bilateral pitting edema of the lower limbs, initially limited to the ankles and feet, but gradually ascending to involve the mid-shin bilaterally. The edema is worse toward the end of the day and partially improves overnight.
Over the past two months, the patient has experienced profound generalized fatigue and weakness, describing an inability to perform routine household activities. He notes marked muscle wasting, particularly of the upper limbs and temporal region. He complains of easy bruising, bleeding from the gums when brushing teeth, and occasional epistaxis over the past month. He also reports pruritus predominantly over the trunk and inner thighs.
Six weeks prior to admission, his family noticed yellowish discoloration of the sclera and skin, which has progressively deepened in color. Urine became dark (tea-colored), and stools became pale and clay-colored.
One week before admission, he noticed a marked reduction in urine output — producing less than 400 mL/day — associated with worsening of abdominal distension and a new onset of confusion and drowsiness.
He also reports muscle cramps, predominantly in the calves and thighs, occurring multiple times daily — a finding consistent with his documented hypokalemia.
PAST MEDICAL HISTORY
- Hepatitis C virus (HCV) infection — diagnosed 14 years ago; never received antiviral treatment
- Type 2 Diabetes Mellitus — diagnosed 8 years ago; on oral hypoglycemics (metformin, recently stopped due to renal impairment)
- Hypertension — diagnosed 6 years ago; on amlodipine 5 mg OD
- No prior surgeries
- No prior blood transfusions reported (though occupational exposure possible)
DRUG HISTORY
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Furosemide | 40 mg OD | 3 months | Started for ascites management |
| Spironolactone | 100 mg OD | 3 months | Started with furosemide |
| Amlodipine | 5 mg OD | 6 years | For hypertension |
| Metformin | 500 mg BD | Stopped 2 weeks ago | Withheld due to rising creatinine |
| Lactulose | 30 mL TDS | 3 weeks | For encephalopathy prevention |
SOCIAL HISTORY
- Alcohol: Significant alcohol use — 3–4 units/day for approximately 20 years; reduced over last 2 years but not completely stopped
- Smoking: 20 pack-year history; stopped 5 years ago
- Diet: Poor nutritional intake; predominantly high-carbohydrate, low-protein diet
- Occupation: Retired laborer with prior occupational exposure to chemicals
- Travel: No recent travel outside country
FAMILY HISTORY
- Father died of liver disease (unknown type)
- No known hereditary liver conditions
- No family history of renal disease or diabetes
SYSTEMIC REVIEW
- CNS: Mild confusion, sleep inversion (sleepy during day, awake at night), occasional flapping tremor (asterixis) noted by family — suggestive of early hepatic encephalopathy. No seizures.
- CVS: Palpitations, no chest pain, no orthopnea (though cannot lie flat due to ascites)
- Respiratory: Mild breathlessness at rest, worsening on exertion — likely due to diaphragmatic splinting from massive ascites
- GI: Anorexia, nausea, early satiety, no hematemesis, no melena
- Renal: Oliguria, dark urine, frothy urine absent
- Musculoskeletal: Generalized muscle cramps, proximal muscle weakness
- Skin: Jaundice, pruritus, easy bruising
PHYSICAL EXAMINATION
General Appearance
Chronically ill-looking male, icteric, pale, cachectic with obvious muscle wasting. Alert but mildly confused and disoriented to time. Cooperative but slow in responding to commands.
Vital Signs
| Parameter | Finding |
|---|---|
| Temperature | 37.4°C (low-grade) |
| Blood Pressure | 100/65 mmHg |
| Heart Rate | 96 bpm, regular |
| Respiratory Rate | 20 breaths/min |
| SpO₂ | 96% on room air |
| Weight | 68 kg (estimated dry weight ~60 kg) |
| BMI | 22.3 kg/m² (low, muscle-wasted) |
Head & Neck
- Eyes: Deep icteric sclera bilaterally; no Kayser-Fleischer rings
- Parotid glands: Bilaterally enlarged (alcohol-associated)
- Mouth: Bleeding gums, fetor hepaticus (musty, sweet smell)
- Neck: No lymphadenopathy; no JVP elevation
Hands & Upper Limbs
- Palmar erythema — bilateral, involving thenar and hypothenar eminences
- Dupuytren's contracture — right hand, ring finger
- Leukonychia (whitening of nails)
- Asterixis — positive bilateral (flapping tremor on sustained wrist extension)
- Muscle wasting — bilateral, prominent
Chest
- Spider naevi — 8 lesions noted over upper chest, neck, and shoulders (>5 = significant)
- Gynecomastia — bilateral, non-tender breast tissue enlargement
- Chest expansion — reduced at bases bilaterally (small bilateral pleural effusions, right > left)
- Dull on percussion at right base; reduced air entry
Abdomen
- Inspection: Grossly distended, flanks full, umbilicus everted, dilated superficial veins (caput medusae pattern around umbilicus)
- Palpation: Tense, non-tender; liver impalpable (shrunken cirrhotic liver); splenomegaly — spleen palpable 4 cm below left costal margin; no renal masses
- Percussion: Shifting dullness — positive; fluid thrill — positive (tense ascites)
- Auscultation: Bowel sounds present; no hepatic bruit
Lower Limbs
- Bilateral pitting edema — grade 3+, extending to mid-shin
- Muscle wasting of thighs and calves
CNS
- Mildly confused; GCS 13/15 (E4V4M5)
- Asterixis present
- No focal neurological deficit
- West Haven Grade II hepatic encephalopathy
Genitourinary
- Scrotal edema present
- Urine output: 300–400 mL over previous 24 hours (oliguria)
INVESTIGATIONS
Haematology
| Test | Patient Value | Normal Range |
|---|---|---|
| Haemoglobin | 9.2 g/dL | 13.5–17.5 g/dL |
| MCV | 104 fL | 80–100 fL |
| WBC | 3.1 × 10⁹/L | 4–11 × 10⁹/L |
| Platelets | 74 × 10⁹/L | 150–400 × 10⁹/L |
| PT | 22 seconds | 11–14 seconds |
| INR | 1.9 | <1.2 |
| aPTT | 46 seconds | 25–35 seconds |
Comment: Pancytopenia consistent with hypersplenism. Macrocytic anaemia from folate deficiency and alcohol. Coagulopathy from reduced hepatic synthesis of clotting factors.
Biochemistry
| Test | Patient Value | Normal Range | Interpretation |
|---|---|---|---|
| Sodium (Na⁺) | 128 mEq/L | 135–145 | Hyponatremia (dilutional) |
| Potassium (K⁺) | 2.8 mEq/L | 3.5–5.0 | Hypokalemia |
| Chloride (Cl⁻) | 92 mEq/L | 98–106 | Low (hypochloremic) |
| Bicarbonate (HCO₃⁻) | 30 mEq/L | 22–29 | Mild metabolic alkalosis |
| Urea (BUN) | 28 mg/dL | 7–20 | Mildly elevated |
| Creatinine | 2.1 mg/dL | 0.7–1.2 | Elevated |
| eGFR (CKD-EPI) | 32 mL/min/1.73m² | >60 | Reduced (Stage 3b) |
| Cystatin-C | 1.9 mg/L | 0.5–1.0 | Elevated (confirms true GFR reduction) |
| Glucose (fasting) | 78 mg/dL | 70–100 | Low-normal (impaired gluconeogenesis) |
| Albumin | 2.1 g/dL | 3.5–5.0 | Severely low |
| Total Bilirubin | 7.8 mg/dL | 0.2–1.2 | Severely elevated |
| Direct Bilirubin | 5.4 mg/dL | 0–0.3 | Predominantly conjugated |
| AST | 112 U/L | 10–40 | Elevated (AST > ALT pattern) |
| ALT | 68 U/L | 7–56 | Mildly elevated |
| ALP | 210 U/L | 44–147 | Elevated |
| GGT | 320 U/L | 8–61 | Markedly elevated (alcohol marker) |
| Total Protein | 5.2 g/dL | 6.4–8.3 | Low |
| LDH | 280 U/L | 140–280 | Upper limit |
| Ammonia (serum) | 98 µmol/L | 11–51 | Elevated (encephalopathy) |
| Uric Acid | 7.2 mg/dL | 3.5–7.2 | Upper limit |
| Calcium | 7.6 mg/dL | 8.5–10.2 | Hypocalcemia |
| Magnesium | 1.4 mg/dL | 1.7–2.2 | Hypomagnesemia |
| Phosphate | 2.8 mg/dL | 2.5–4.5 | Normal |
Liver Function / Synthetic Function Summary
| Parameter | Value | Significance |
|---|---|---|
| INR | 1.9 | ↓ Clotting factor synthesis |
| Albumin | 2.1 g/dL | ↓ Albumin synthesis |
| Total Bilirubin | 7.8 mg/dL | ↓ Bilirubin conjugation/excretion |
| Ammonia | 98 µmol/L | ↓ Urea cycle function |
Urine Analysis
| Test | Finding |
|---|---|
| Colour | Dark amber |
| Protein | Trace (not nephrotic-range) |
| Blood | Negative |
| Glucose | Negative |
| Bilirubin | Positive |
| Urobilinogen | Increased |
| Microscopy | Granular casts (tubular injury) |
| Urinary Na⁺ | 8 mEq/L (< 10 — consistent with HRS/prerenal) |
| FENa | 0.2% (< 1% — HRS pattern) |
| Urine creatinine | 42 mg/dL |
| Urine osmolality | 480 mOsm/kg (concentrated urine) |
Comment: Low urinary sodium with concentrated urine in the setting of oliguria and cirrhosis is characteristic of hepatorenal syndrome rather than intrinsic CKD.
Viral Serology
| Test | Result |
|---|---|
| Anti-HCV | Positive |
| HCV RNA (PCR) | 1.2 × 10⁶ IU/mL (active viremia) |
| HBsAg | Negative |
| Anti-HBs | Negative |
| HBeAg | Negative |
| Anti-HAV IgM | Negative |
| HIV | Negative |
Autoimmune Panel
| Test | Result |
|---|---|
| ANA | Negative |
| ASMA | Negative |
| AMA | Negative |
| Anti-LKM1 | Negative |
Tumour Markers
| Marker | Value | Normal |
|---|---|---|
| AFP (Alpha-fetoprotein) | 48 ng/mL | < 20 ng/mL |
Comment: Mildly elevated AFP in the context of cirrhosis warrants further imaging to exclude hepatocellular carcinoma (HCC).
Imaging
Abdominal Ultrasound
- Liver: Small, shrunken, coarsened echogenicity, irregular surface — consistent with established cirrhosis. No focal lesion seen on standard US (AFP elevated → proceed to triple-phase CT)
- Portal vein: Dilated at 14 mm (normal <13 mm) — portal hypertension
- Spleen: Enlarged at 16 cm (splenomegaly)
- Ascites: Massive free fluid in the peritoneal cavity
- Kidneys: Both kidneys normal in size (10 cm), smooth outline, no hydronephrosis, no stones — argues against intrinsic CKD/obstruction
- Gallbladder: Thin-walled, contracted
Upper GI Endoscopy
- Oesophageal varices: Grade II–III oesophageal varices (tortuous, occupying <1/3 of lumen, with red wale markings — high bleeding risk)
- Gastric varices: Not seen
- Portal hypertensive gastropathy: Mild
Chest X-Ray
- Right-sided pleural effusion (hepatic hydrothorax)
- No consolidation, no cardiac enlargement
ECG
- Sinus tachycardia
- Prominent U waves in V2–V4 — consistent with hypokalemia
- Prolonged QT interval (480 ms) — risk of arrhythmia
Scoring Systems
Child-Pugh Score
| Parameter | Finding | Points |
|---|---|---|
| Bilirubin | 7.8 mg/dL (>3.0) | 3 |
| Albumin | 2.1 g/dL (<2.8) | 3 |
| INR | 1.9 (1.7–2.3) | 2 |
| Ascites | Tense (severe) | 3 |
| Encephalopathy | Grade II | 2 |
| Total | 13 |
Child-Pugh Class C — severe hepatic decompensation. 1-year survival ~35%.
MELD-Na Score
| Variable | Value |
|---|---|
| Creatinine | 2.1 mg/dL |
| Bilirubin | 7.8 mg/dL |
| INR | 1.9 |
| Sodium | 128 mEq/L |
| MELD-Na Score | ~28 |
MELD-Na ≥25 indicates high 3-month mortality risk. This patient requires urgent liver transplant evaluation.
DIAGNOSIS
Primary Diagnosis:
Chronic Liver Disease (CLD) — Decompensated Liver Cirrhosis (Child-Pugh C)
Aetiology:
- Chronic Hepatitis C (HCV, active viremia) — primary cause
- Alcohol-associated liver disease — contributing cause (20 years of significant use)
Complications Present:
- Massive ascites with spontaneous bacterial peritonitis (SBP) risk
- Hepatic encephalopathy — West Haven Grade II
- Oesophageal varices — Grade II–III with high bleeding risk
- Hepatorenal syndrome (HRS) — Type 2 (gradual creatinine rise, oliguria, low urinary Na⁺)
- Hypokalemia (K⁺ 2.8 mEq/L) — secondary hyperaldosteronism + diuretic use
- Hyponatremia — dilutional (Na⁺ 128 mEq/L)
- Hepatic hydrothorax — right-sided pleural effusion
- Coagulopathy — INR 1.9
- Hypersplenism — thrombocytopenia, anaemia, leukopenia
- Raised AFP — HCC surveillance required
PATHOPHYSIOLOGY SUMMARY
Chronic HCV + Alcohol
↓
Hepatocyte necrosis → Stellate cell activation → Fibrosis → Cirrhosis
↓
Portal Hypertension
↙ ↘
Varices Splanchnic vasodilation
↓
↓ Effective blood volume
↓
RAAS activation + ↑ ADH
↓
Na⁺ & H₂O retention → Ascites + Edema
↓
K⁺ wasting → HYPOKALEMIA
↓
Renal vasoconstriction → HRS → ↑ CREATININE
MANAGEMENT PLAN
1. Immediate / Emergency
- IV access (large bore), strict fluid balance monitoring
- Urine output hourly
- Avoid nephrotoxic drugs (NSAIDs, aminoglycosides, contrast)
- Stop metformin (already done) — lactic acidosis risk with renal impairment
- ECG monitoring (QT prolongation risk with hypokalemia)
2. Hypokalemia Correction
- Oral potassium supplementation: KCl 40 mEq TDS (if tolerating oral)
- If K⁺ < 2.5 mEq/L or symptomatic: IV KCl infusion (10–20 mEq/hour via central line, with continuous cardiac monitoring)
- Correct hypomagnesemia first (Mg²⁺ 1.4 mg/dL) — hypokalemia refractory to treatment until Mg²⁺ is normalized
- IV Magnesium sulfate 2 g over 20 minutes, then 1 g/hour infusion
- Re-check electrolytes every 4–6 hours
- Review diuretic dosing — temporarily withhold furosemide; increase spironolactone (K⁺-sparing)
3. Ascites Management
- Therapeutic paracentesis — large-volume paracentesis (LVP) 5–6 L with IV albumin 8 g per litre removed (prevent post-paracentesis circulatory dysfunction)
- Diuretics (after K⁺ correction): Spironolactone 200 mg + Furosemide 80 mg ratio — titrate to weight loss of 0.5 kg/day
- Low-sodium diet (< 88 mEq/day, ~2 g Na⁺/day)
- Fluid restriction to 1.0–1.5 L/day given hyponatremia
4. Hepatorenal Syndrome (Elevated Creatinine)
- Terlipressin 0.5–1 mg IV every 4–6 hours (vasoconstrictor of choice for HRS-AKI)
- IV Albumin 1 g/kg on Day 1, then 20–40 g/day (expands effective intravascular volume)
- Hold all diuretics until creatinine stabilizes
- Avoid contrast media, NSAIDs
- Target: creatinine reduction to <1.5 mg/dL or by >50%
- If no response in 3 days: escalate terlipressin or consider TIPS (transjugular intrahepatic portosystemic shunt) in select cases
5. Hepatic Encephalopathy
- Lactulose 30–45 mL every 6 hours — titrate to 2–3 soft stools/day; prevents ammonia absorption
- Rifaximin 550 mg BD — non-absorbable antibiotic reducing ammonia-producing gut bacteria
- Identify and treat precipitating factors: infection, constipation, electrolyte imbalance
- Adequate protein intake: 1.2–1.5 g/kg/day (do not restrict protein — worsens sarcopenia)
- Correct hypokalemia (hypokalemia → ↑ ammonia production → worsens encephalopathy)
6. Oesophageal Varices — Prophylaxis
- Non-selective beta-blocker: Propranolol 20 mg BD or Carvedilol 6.25 mg BD (titrate to HR 55–60 bpm) — for secondary prophylaxis
- Band ligation at endoscopy — elective (not during acute crisis)
- Avoid drugs that raise portal pressure
7. HCV Treatment
- Refer to hepatology for Direct-Acting Antiviral (DAA) therapy
- Sofosbuvir-based regimen (e.g., Sofosbuvir/Velpatasvir) — once renal function stabilizes
- SVR (sustained virological response) may halt further fibrosis progression
- Note: dose adjustment required for GFR <30 mL/min
8. HCC Surveillance
- AFP mildly elevated at 48 ng/mL — requires triple-phase CT abdomen
- If no lesion found: 6-monthly ultrasound + AFP
- Refer to multidisciplinary liver team
9. Liver Transplantation Assessment
- MELD-Na score 28 — qualifies for transplant listing in most centers (threshold ≥15)
- Refer to transplant centre for evaluation
- Alcohol abstinence requirement: minimum 6 months (already partially met)
- Treat HCV prior to transplant if feasible
10. Nutrition
- High-calorie, adequate-protein diet (35 kcal/kg/day, 1.2–1.5 g protein/kg/day)
- Branched-chain amino acid (BCAA) supplements
- Vitamin supplementation: Thiamine, Folate, Zinc
- Dietitian referral
MONITORING PARAMETERS
| Parameter | Frequency |
|---|---|
| Electrolytes (K⁺, Na⁺, Mg²⁺) | Every 4–6 hours initially, then daily |
| Creatinine, BUN | Daily |
| Urine output | Hourly |
| PT/INR | Every 48 hours |
| Serum ammonia | Daily |
| Weight (dry weight) | Daily |
| Mental status (encephalopathy grade) | Every shift |
| Blood pressure | Every 4 hours |
| ECG | Daily (QT monitoring) |
PROGNOSIS
- Child-Pugh Class C with MELD-Na 28 carries a 3-month mortality of approximately 20–30% without transplant
- Hepatorenal syndrome — without treatment, median survival Type 2 HRS is 3–6 months
- Hypokalemia in this context is correctable but its persistent presence (via aldosterone, diuretics) worsens both encephalopathy and renal function
- HCV SVR with DAA therapy, if achievable, significantly improves long-term outcomes including regression of fibrosis in some patients
- Without transplant, progressive decompensation is expected
LEARNING POINTS FROM THIS CASE
- Hypokalemia in CLD results from secondary hyperaldosteronism, diuretic therapy, and vomiting — not from renal disease per se.
- Elevated creatinine in CLD is most commonly hepatorenal syndrome (functional renal failure) — differentiated from CKD by low urinary Na⁺, normal kidney size on US, and absence of proteinuria.
- Creatinine underestimates GFR in cirrhosis — always confirm with cystatin-C.
- Hypokalemia worsens hepatic encephalopathy by increasing renal ammonia production and releasing ammonia to the portal circulation.
- Correct hypomagnesemia before hypokalemia — refractory hypokalemia is often due to unrecognized hypomagnesemia.
- MELD-Na guides transplant urgency — score ≥15 qualifies for listing.
- The AST > ALT pattern (AST:ALT ratio >2) suggests alcoholic hepatitis on top of HCV cirrhosis.
This case integrates hypokalemia (K⁺ 2.8 mEq/L) and elevated creatinine (2.1 mg/dL) as direct complications of decompensated cirrhosis, explaining each via the underlying pathophysiological cascade from portal hypertension through to hepatorenal syndrome and secondary hyperaldosteronism.
Stigmata of cld
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
stigmata chronic liver disease spider nevi palmar erythema cirrhosis
Finding Sources
Finding Sources
Searching Images
jaundice ascites caput medusae spider angioma cirrhosis physical signs
Excellent material gathered. Here is a comprehensive, system-by-system breakdown of all stigmata of CLD:
Stigmata of Chronic Liver Disease (CLD)
The stigmata of CLD are the clinical signs that arise from three underlying mechanisms:
- Impaired hepatic synthetic/metabolic function (hypoalbuminemia, coagulopathy)
- Portal hypertension (hyperdynamic circulation, varices, ascites)
- Hyperestrogenism (impaired hepatic estrogen metabolism → feminization signs)
HANDS
1. Palmar Erythema
- Bilateral redness of the thenar and hypothenar eminences and fingertips
- Caused by hyperestrogenism → cutaneous vasodilation
- Blanchable on pressure
- Also seen in pregnancy, rheumatoid arthritis, thyrotoxicosis

2. Dupuytren's Contracture
- Thickening and fibrosis of the palmar fascia, causing flexion of the ring ± little finger
- Predominantly in alcoholic cirrhosis
- Mechanism: alcohol-related fibroblast activation
3. Leukonychia (White Nails)
- Terry's nails — white nails with a narrow pink distal band (cirrhosis)
- Muehrcke's lines — paired white transverse bands (hypoalbuminemia); fade with pressure (apparent leukonychia)
- Mechanism: hypoalbuminemia → altered nail bed vascularity
4. Clubbing
- Bulbous enlargement of the fingertip with loss of nail angle
- Associated with hypoalbuminemia and hepatopulmonary syndrome
- Also indicates chronic hypoxia in CLD
5. Flapping Tremor (Asterixis)
- Sustained dorsiflexion of wrists → irregular "flap" as tone briefly lapses
- Indicates hepatic encephalopathy (ammonia-related impairment of inhibitory motor networks)
- Not a true tremor — it is a negative myoclonus
- Also seen in renal failure, CO₂ retention
6. Muscle Wasting
- Most prominent in thenar/hypothenar eminences and bitemporal regions
- Reflects sarcopenia from protein catabolism, hyperammonemia, and malnutrition
FACE & NECK
7. Jaundice (Icterus)
- Yellow discoloration of sclera (first visible site, detected at bilirubin >2–3 mg/dL) → skin → mucous membranes
- Due to impaired hepatic bilirubin conjugation and excretion
- Dark (conjugated hyperbilirubinemia) urine + pale stools accompany it
8. Parotid Enlargement
- Bilateral painless parotid gland swelling
- Characteristic of alcoholic liver disease
- Mechanism: alcohol-related sialosis (fatty infiltration of parotid)
9. Fetor Hepaticus
- A distinctive musty, sweetish breath odour ("smell of a freshly opened corpse")
- Caused by exhaled dimethyl sulfide and other mercaptans derived from gut bacteria passing through portosystemic shunts
- Indicates significant portosystemic shunting and encephalopathy
10. Xanthelasma
- Yellowish plaques around eyelids
- Seen in primary biliary cholangitis and other cholestatic liver diseases
- Due to hypercholesterolaemia from impaired bile excretion
CHEST & TRUNK
11. Spider Naevi (Spider Angiomata)
- Central arteriole with radiating capillary legs ("spider legs"), which blanch and refill from the centre on pressure
- Found on the upper chest, arms, face, neck (distribution of the superior vena cava)
- >5 spider naevi = significant (pathological)
- Due to hyperestrogenism → vasodilation; also mediated by VEGF
- A single spider naevus can be normal; bilateral and numerous = CLD until proven otherwise

12. Paper Money Skin
- Numerous fine thread-like telangiectasias scattered over the torso, resembling the security threads in bank notes
- A variant of cutaneous vasodilation from hyperestrogenism
13. Gynaecomastia
- Benign enlargement of breast tissue in males
- Due to elevated estrogen (impaired hepatic metabolism) and decreased testosterone
- Bilateral, non-tender
- Must distinguish from lipomastia (fat, not glandular tissue)
14. Loss of Body Hair
- Loss of chest, axillary, and pubic hair in males
- Hyperestrogenism → feminization pattern
15. Scratch Marks (Excoriation)
- Generalised skin excoriations from pruritus
- Caused by bile salt deposition in skin (especially in cholestatic liver disease)
ABDOMEN
16. Ascites
- Fluid accumulation in the peritoneal cavity
- Signs: shifting dullness, fluid thrill (massive ascites), everted umbilicus, flanks full
- Due to: portal hypertension + hypoalbuminemia (low oncotic pressure) + RAAS activation (Na⁺ and H₂O retention)
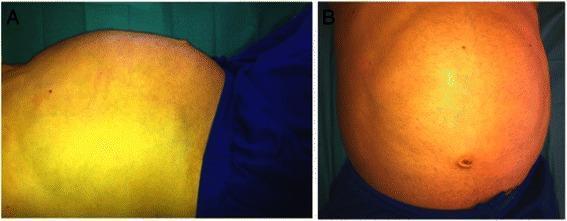
17. Caput Medusae
- Dilated, tortuous superficial abdominal veins radiating from the umbilicus
- Blood flows away from the umbilicus (distinguishes it from IVC obstruction where blood flows upward)
- Due to recanalization of the paraumbilical vein as a portosystemic collateral under portal hypertension
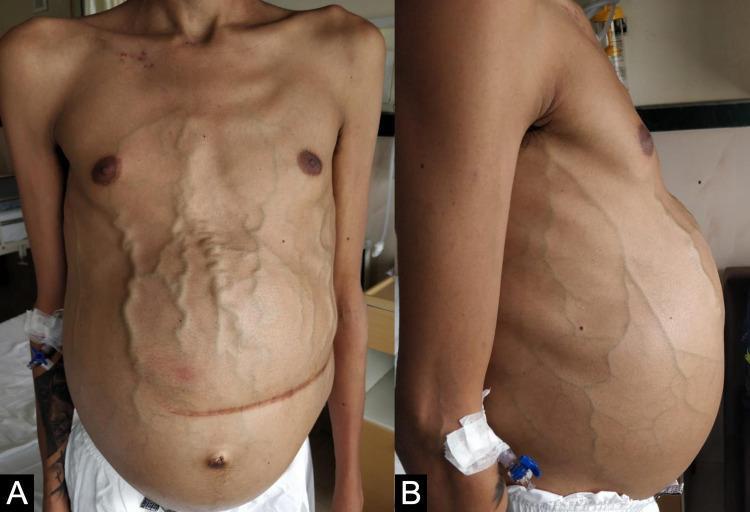
18. Splenomegaly
- Palpable spleen >12 cm, palpable below left costal margin
- Due to portal hypertension → splenic venous congestion
- Leads to hypersplenism → pancytopenia (low Hb, WBC, platelets)
19. Hepatomegaly or Small Liver
- Early CLD: liver enlarged (fatty infiltration, hepatitis)
- Advanced cirrhosis: liver shrunken, hard, nodular — span <7 cm on percussion
- Pathognomonic of cirrhosis: small right lobe + palpable, nodular, firm left lobe
LOWER LIMBS
20. Pitting Oedema
- Bilateral, dependent, pitting oedema of ankles and legs
- Due to hypoalbuminemia (↓ oncotic pressure) + Na⁺ retention + portal hypertension
- Extends proximally as disease worsens
21. Muscle Wasting (Legs)
- Wasting of quadriceps, calves (sarcopenia)
- Reflects protein catabolism, hyperammonemia, reduced physical activity
GENITALIA (MALES)
22. Testicular Atrophy
- Reduced testicular size and firmness
- Due to hyperestrogenism suppressing gonadotropins → hypogonadism
- Incidence ~45% in cirrhotic males (Mulholland & Greenfield's Surgery)
- Associated with reduced libido and infertility
CNS / NEUROLOGICAL
23. Hepatic Encephalopathy Signs
- Asterixis (as above)
- Confusion, disorientation, sleep inversion
- Constructional apraxia (inability to draw a 5-pointed star)
- Fetor hepaticus (as above)
- Graded West Haven I–IV
SUMMARY TABLE
| Region | Stigma | Mechanism |
|---|---|---|
| Hands | Palmar erythema | Hyperestrogenism → vasodilation |
| Hands | Dupuytren's contracture | Alcohol → fibroblast activation |
| Hands | Leukonychia / Terry's nails / Muehrcke's lines | Hypoalbuminemia |
| Hands | Clubbing | Hypoalbuminemia, hepatopulmonary syndrome |
| Hands | Asterixis | Hyperammonemia → encephalopathy |
| Hands | Muscle wasting (thenar) | Sarcopenia, malnutrition |
| Face | Jaundice / Icterus | ↓ Bilirubin conjugation & excretion |
| Face | Parotid enlargement | Alcohol-related sialosis |
| Breath | Fetor hepaticus | Dimethyl sulfide via portosystemic shunts |
| Face | Xanthelasma | Cholestasis → hypercholesterolaemia |
| Chest | Spider naevi (>5) | Hyperestrogenism + VEGF |
| Chest | Paper money skin | Telangiectasias from vasodilation |
| Chest | Gynaecomastia | ↑ Estrogen / ↓ Testosterone |
| Chest | Loss of body hair | Hyperestrogenism (feminization) |
| Skin | Scratch marks / excoriation | Pruritus from bile salt deposition |
| Skin | Bruising / petechiae | ↓ Clotting factors + thrombocytopenia |
| Abdomen | Ascites | Portal HTN + ↓ albumin + RAAS activation |
| Abdomen | Caput medusae | Paraumbilical vein recanalization (portal HTN) |
| Abdomen | Splenomegaly | Portal HTN → splenic congestion |
| Abdomen | Small, nodular liver | Fibrosis, regenerative nodules (cirrhosis) |
| Legs | Pitting oedema | ↓ Albumin + Na⁺ retention |
| Genitalia | Testicular atrophy | Hyperestrogenism → hypogonadism |
| Neuro | Confusion, sleep inversion | Hepatic encephalopathy |
Key Memory Points
- Spider naevi + palmar erythema + gynaecomastia + testicular atrophy = the classic tetrad of hyperestrogenism in cirrhosis
- Asterixis + fetor hepaticus + confusion = hepatic encephalopathy triad
- Caput medusae — blood flows away from umbilicus (portal HTN); vs. IVC obstruction — blood flows upward
- Terry's nails (white nails) = specific for cirrhosis; Muehrcke's lines = hypoalbuminemia (any cause)
- Parotid enlargement is specific to alcoholic liver disease
- A small, hard, nodular liver on percussion/palpation is pathognomonic of cirrhosis
"On physical examination, stigmata of cirrhosis consist of muscle atrophy, mainly involving the bitemporal muscle regions and thenar/hypothenar eminences; spider angiomas, mostly on the trunk, face, and upper limbs; and palmar erythema involving the thenar and hypothenar eminences" — Goldman-Cecil Medicine
dexamethasone
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material. Here is the full pharmacology of dexamethasone:
Dexamethasone — Full Pharmacology
DRUG CLASS & BASIC PROFILE
| Property | Detail |
|---|---|
| Class | Synthetic fluorinated glucocorticoid |
| Structure | Fluorinated at C9α + methyl at C16α (fluorine → potency; methyl → negligible mineralocorticoid activity) |
| Routes | PO, IV, IM, intrathecal, intraocular, topical |
| Half-life | Plasma: ~3–5 hours; Biologic: 36–54 hours (long-acting) |
| Anti-inflammatory potency | 25–30x hydrocortisone |
| Mineralocorticoid activity | Negligible (≈ 0) |
| Equivalent dose | 0.75 mg = 5 mg prednisone = 20 mg hydrocortisone |
"Relative anti-inflammatory potencies: cortisone 0.8; hydrocortisone 1; prednisone 4; methylprednisolone 5; dexamethasone 25" — Washington Manual of Medical Therapeutics
MECHANISM OF ACTION
1. Genomic (Primary) Mechanism
- Dexamethasone diffuses freely into cells and binds the cytosolic glucocorticoid receptor (GR-α)
- The drug-receptor complex translocates into the nucleus
- Binds glucocorticoid response elements (GREs) on DNA
- Transactivation: induces anti-inflammatory proteins (lipocortin/annexin-1, IL-10, IκB)
- Transrepression: suppresses pro-inflammatory gene transcription (TNF-α, IL-1, IL-6, IL-8, COX-2, iNOS, PLA₂)
2. Non-Genomic (Rapid) Mechanism
- At high doses: direct membrane effects
- Inhibition of NF-κB pathway → blocks transcription of >60 inflammatory mediators
- Rapid onset (within minutes) — independent of transcription
Net Anti-Inflammatory Effects:
- ↓ Capillary permeability and vasodilation (less edema)
- ↓ Neutrophil and macrophage migration to inflamed sites
- ↓ Phospholipase A₂ → ↓ arachidonic acid release → ↓ prostaglandins + leukotrienes
- ↓ Lymphocyte proliferation → immunosuppression
- Stabilises lysosomal membranes → prevents release of proteolytic enzymes
HPA Axis Suppression:
- Exogenous dexamethasone suppresses CRH (hypothalamus) and ACTH (pituitary) via negative feedback
- → ↓ Endogenous cortisol production
- This is the basis of the Dexamethasone Suppression Test (DST)
PHARMACOKINETICS
| Parameter | Detail |
|---|---|
| Absorption (oral) | Rapid; ~78% bioavailable |
| Peak plasma | 1–2 hours (oral); immediate (IV) |
| Protein binding | ~77% (albumin + transcortin) |
| Distribution | Widely distributed; crosses BBB, placenta |
| Metabolism | Hepatic (CYP3A4) → inactive metabolites |
| Excretion | Renal (primarily); small biliary component |
| Duration of action | Long — biologic effect lasts 36–54 hours |
CLINICAL INDICATIONS & DOSES
1. Cerebral Oedema (Brain tumour, metastasis, abscess)
- 4–8 mg IV every 6 hours
- Reduces vasogenic oedema around tumours by restoring blood-brain barrier integrity
- First-line corticosteroid for this indication (chosen because of negligible Na⁺-retaining effect — avoids worsening cerebral oedema)
2. Bacterial Meningitis
- 0.15 mg/kg IV every 6 hours × 4 days (given 15–20 min before or with first antibiotic dose)
- Reduces neurological complications (hearing loss, mortality in pneumococcal meningitis)
- Most effective in Streptococcus pneumoniae meningitis in adults
3. Croup (Laryngotracheobronchitis)
- 0.6 mg/kg IM/PO (single dose)
- Reduces airway inflammation and hospitalisation
4. Nausea & Vomiting (PONV / Chemotherapy)
- 4–8 mg IV — as part of antiemetic protocols
- Synergistic with ondansetron (different mechanisms)
5. Anaphylaxis / Severe Allergy
- 8–10 mg IV (after epinephrine — not first-line)
- Prevents biphasic reaction
6. Asthma Exacerbation
- 0.15–0.6 mg/kg/day (single dose often sufficient vs. multi-day prednisone)
7. Adrenal Insufficiency (Secondary)
- Alternative to hydrocortisone when mineralocorticoid replacement not needed
8. COVID-19 (Severe / Mechanically Ventilated)
- 6 mg OD × 10 days — RECOVERY trial: 22% reduction in mortality in ventilated patients
9. Septic Shock (Refractory)
- Adjunct in vasopressor-refractory shock
- Lower dose than hydrocortisone; used when relative adrenal insufficiency suspected
10. Haematological Malignancies
- Component of regimens: R-CHOP (lymphoma), VAD/VRd (myeloma), EPOCH
- High doses: 20–40 mg/day in myeloma protocols
11. Spinal Cord Compression (Metastatic)
- 16 mg/day initially, then taper
- Reduces perilesional oedema, preserves neurological function
12. Rheumatological / Inflammatory Conditions
- SLE, vasculitis, polymyositis flares
- Equivalent dosing to prednisone (0.75 mg dexamethasone = 5 mg prednisone)
13. Premature Labour (Foetal Lung Maturity)
- 12 mg IM every 24 hours × 2 doses (24–34 weeks gestation)
- Stimulates foetal surfactant production → reduces RDS, IVH, NEC
14. Dexamethasone Suppression Test (Diagnostic)
- Low-dose DST: 1 mg at 11 PM → cortisol at 8 AM
- Normal: cortisol suppressed to <1.8 µg/dL
- Cushing's: cortisol NOT suppressed
- High-dose DST: 8 mg → suppresses pituitary Cushing's (but NOT adrenal tumour or ectopic ACTH)
15. Post-Extubation Stridor
- 0.1–0.25 mg/kg IV × 1–3 doses — reduces post-extubation laryngeal oedema
COMPARISON WITH OTHER GLUCOCORTICOIDS
| Drug | Anti-inflam. Potency | Mineralocorticoid Activity | Duration | Equivalent Dose |
|---|---|---|---|---|
| Hydrocortisone | 1 | ++ | Short (8–12 hr) | 20 mg |
| Cortisone | 0.8 | ++ | Short | 25 mg |
| Prednisone | 4 | + | Intermediate (12–36 hr) | 5 mg |
| Prednisolone | 4 | + | Intermediate | 5 mg |
| Methylprednisolone | 5 | Minimal | Intermediate | 4 mg |
| Dexamethasone | 25–30 | Negligible | Long (36–54 hr) | 0.75 mg |
| Betamethasone | 25 | Negligible | Long | 0.6 mg |
| Fludrocortisone | 10 | Very high (+++) | Intermediate | — (mineralocorticoid) |
ADVERSE EFFECTS
Adverse effects are dose- and duration-dependent — generally significant with doses >10 mg/day prednisone-equivalent for >2 weeks.
Endocrine / Metabolic
- Hyperglycaemia / iatrogenic diabetes (especially in pre-diabetics)
- Cushing's syndrome (moon face, buffalo hump, central obesity, striae, skin atrophy)
- Adrenal suppression → risk of adrenal crisis on abrupt withdrawal (assume suppression if >20 mg prednisone-equivalent for >3 weeks)
- Hypokalaemia — though dexamethasone has minimal mineralocorticoid effect, high doses can cause this at supraphysiologic levels
- Dyslipidaemia, weight gain
Musculoskeletal
- Osteoporosis → fractures (vertebral compression most common)
- Prevention: calcium 1–1.5 g/day + Vitamin D 1000 IU/day from day 1; bisphosphonates (alendronate) for long-term use
- Avascular necrosis (osteonecrosis) — femoral head most commonly affected
- Proximal myopathy — painless weakness of shoulder/hip girdle muscles; CK normal; resolves after stopping
Cardiovascular
- Hypertension (Na⁺ retention at high doses despite low mineralocorticoid activity)
- Dyslipidaemia
Immunologic
- Increased susceptibility to bacterial, fungal, viral, parasitic infections
- Reactivation of TB (always screen with TST/IGRA before prolonged use)
- Pneumocystis jirovecii pneumonia (PCP) — prophylaxis with co-trimoxazole if >20 mg prednisone-equivalent for >1 month
- Local signs of infection may be masked (fever generally not suppressed)
Ophthalmic
- Posterior subcapsular cataracts
- Glaucoma (raised IOP)
- Increased risk of herpetic eye infection
Psychiatric / CNS
- Euphoria, insomnia, mood swings, irritability (common at initiation)
- Depression, psychosis with prolonged use
- Pseudotumour cerebri (raised ICP) — especially on withdrawal in children
Dermatological
- Skin atrophy, striae, ecchymoses, acne, delayed wound healing, hirsutism
Gastrointestinal
- Peptic ulcer (particularly when combined with NSAIDs)
- Gastritis — co-prescribe PPI if high-risk
- Pancreatitis (rare)
Growth & Development
- Growth suppression in children with prolonged use
- Adrenal suppression in neonates if used in pregnancy long-term
CONTRAINDICATIONS & CAUTIONS
| Contraindication/Caution | Reason |
|---|---|
| Active systemic fungal infection | Severe immunosuppression risk |
| Live vaccines | Impaired immune response |
| Uncontrolled diabetes | Worsens hyperglycaemia significantly |
| Active TB (without antituberculous cover) | Risk of dissemination |
| Peptic ulcer + NSAID use together | Risk of GI haemorrhage |
| Psychiatric history | May precipitate psychosis |
| Osteoporosis (unprotected) | Accelerates bone loss |
| Breastfeeding (high doses) | Transferred to milk |
DRUG INTERACTIONS
| Drug | Interaction |
|---|---|
| CYP3A4 inducers (rifampicin, phenytoin, carbamazepine) | ↓ Dexamethasone levels (reduced effect) |
| CYP3A4 inhibitors (azole antifungals, erythromycin) | ↑ Dexamethasone levels (toxicity risk) |
| NSAIDs | ↑ GI ulceration risk |
| Warfarin | Altered INR — monitor closely |
| Antidiabetic drugs | Hyperglycaemia — adjust insulin/OHAs |
| Diuretics (thiazides, loop) | Additive hypokalaemia |
| Antihypertensives | May oppose blood pressure control |
| Live vaccines | Vaccine failure / disseminated infection |
WITHDRAWAL & TAPERING
Abrupt discontinuation after prolonged use causes adrenal crisis (hypotension, vomiting, collapse, death).
- Taper rule: if used >3 weeks at high doses, taper gradually
- Reduce by ~10–20% every 1–2 weeks
- Cover with "stress dosing" during surgery or severe illness
- Morning dosing (single daily) minimises HPA suppression
SPECIAL USES SUMMARY
| Indication | Dose | Notes |
|---|---|---|
| Cerebral oedema | 4–8 mg IV q6h | No mineralocorticoid effect — ideal |
| Meningitis | 0.15 mg/kg IV q6h × 4 days | With/before first antibiotic |
| Croup | 0.6 mg/kg PO/IM single dose | Reduces stridor within hours |
| Foetal lung maturity | 12 mg IM q24h × 2 | 24–34 weeks gestation |
| PONV prophylaxis | 4–8 mg IV | Pre-induction |
| COVID-19 | 6 mg OD × 10 days | Only if O₂ required (RECOVERY) |
| Cushing's DST (low) | 1 mg at 11 PM | Cortisol <1.8 µg/dL = normal |
| Cushing's DST (high) | 8 mg | Distinguishes pituitary vs adrenal/ectopic |
| Myeloma | 20–40 mg/day (protocols) | Part of combination regimens |
Key distinguishing features of dexamethasone vs. other steroids:
- Highest anti-inflammatory potency among commonly used agents (25–30x)
- Zero mineralocorticoid activity — preferred when Na⁺/water retention must be avoided (brain, spinal cord)
- Longest biologic half-life (36–54 hours) — once-daily dosing possible
- Crosses the blood-brain barrier well — CNS conditions
- Preferred for foetal lung maturation and diagnostic suppression testing
"Dexamethasone 25 [× hydrocortisone in anti-inflammatory potency]" — Washington Manual of Medical Therapeutics "The dexamethasone suppression test — the synthetic glucocorticoid dexamethasone suppresses cortisol release in normal individuals but not those with Cushing syndrome" — Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.