Detailed description of pelvic organ prolapse from barek and Novak
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have sufficient, comprehensive content from Berek & Novak's Gynecology to provide a detailed answer. Let me compile the full description:
Pelvic Organ Prolapse - Berek & Novak's Gynecology
Source: Berek & Novak's Gynecology (ISBN 9781496380357), Chapter 30 - authored by Ballard AV, Meyer I, Varner RE, Gleason JL, Richter HE
Definition
Pelvic organ prolapse (POP) is defined as the "descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix), or the apex of the vagina (vaginal vault or cuff scar after hysterectomy)", correlated with symptoms and assisted by relevant imaging. More precisely, it is the progressive herniation of the pelvic organs through the urogenital diaphragm that most commonly leads to vaginal bulge symptoms.
Epidemiology
- The prevalence of at least one pelvic floor disorder (PFD) in a nationally representative U.S. sample was 23.7%; this more than doubles in women 80 years or older.
- Data from the Women's Health Initiative revealed: anterior POP in 34.3%, posterior wall prolapse in 18.6%, and uterine prolapse in 14.3% of women.
- The lifetime risk that a woman will undergo surgical correction of POP by age 80 is estimated at 1 in 5 (cumulative risk for POP surgery: 12.6%). A woman's combined risk for either POP or SUI surgery is 11.4% by age 60, rising to 15.9% at 70, and 20.2% by age 80.
- The total number of women expected to undergo POP surgery from 2010-2050 is projected to increase by 46%, with estimated annual procedures rising from 166,000 to 245,970.
- The estimated direct annual cost of ambulatory care for PFDs in the U.S. was $412 million in 2006.
Pathophysiology
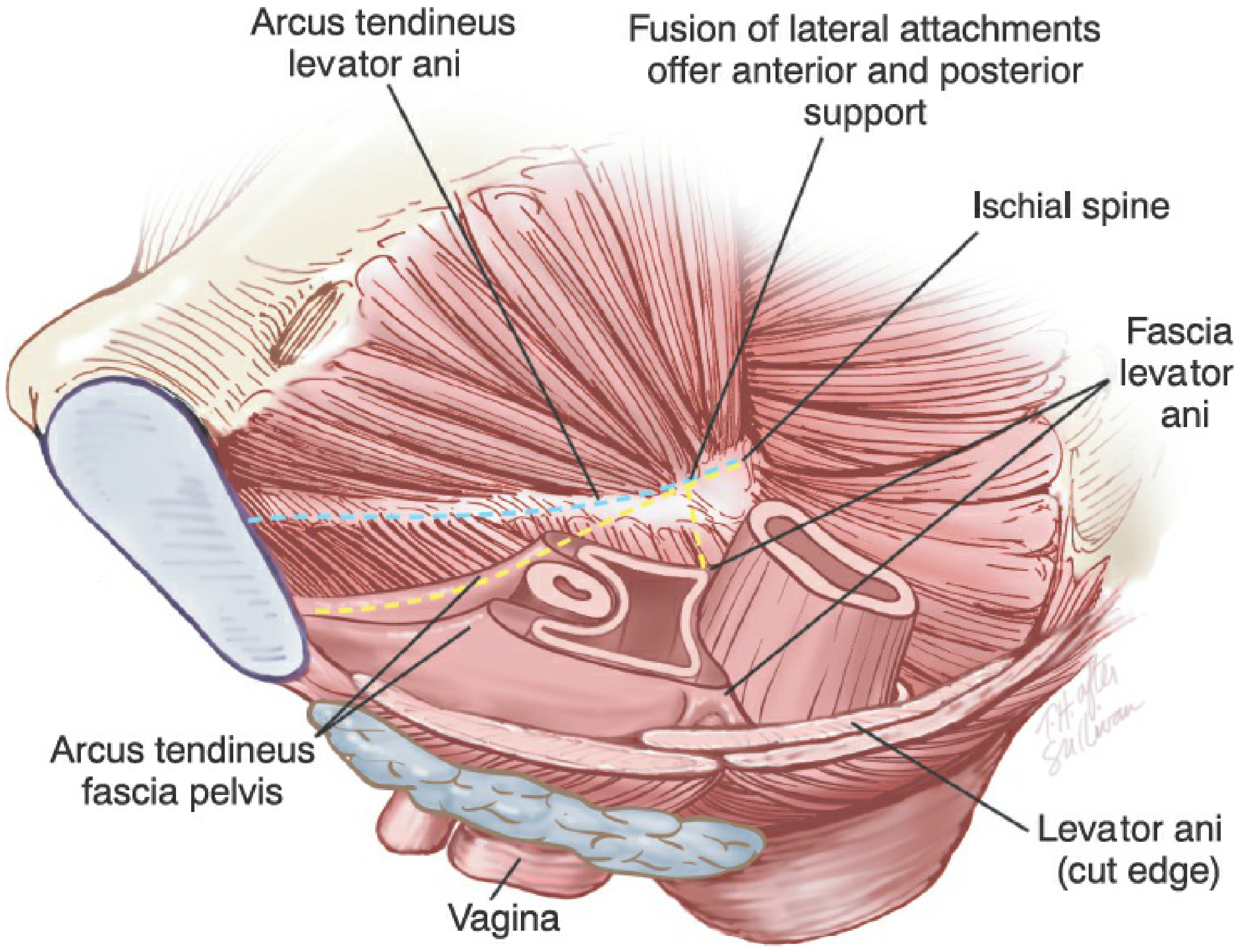
The interaction between the pelvic floor muscles, fibromuscular connective tissue, and intact innervation is key to maintaining support of the pelvic organs. The levator ani/coccygeus muscles hold the pelvic floor closed and provide lifting and closing forces, forming a supportive diaphragm through which the urethra, vagina, and rectum egress.
POP results from attenuation of supportive structures - either actual tears/breaks or neuromuscular dysfunction or both:
- Muscle damage allows the levator hiatus to enlarge, facilitating pelvic organ descent with protrusion of one or both vaginal walls through the hiatus.
- Birth-induced injury to the pubococcygeal portion of the levator ani muscles is seen in 55% of women with prolapse vs. only 16% of women with normal support.
- Failure of the connective tissue attachments between the uterus/vagina and the pelvic wall (cardinal, uterosacral, paravaginal) are strongly related with prolapse.
Three Levels of Pelvic Support (DeLancey)
| Level | Structures | Function |
|---|---|---|
| Level I | Uterosacral/cardinal ligament complex | Maintains vaginal length and axis; suspends the apex |
| Level II | Paravaginal attachments of the lateral vagina to the arcus tendineus and levator fascia | Maintains midline position of the vagina |
| Level III | Muscles and connective tissue surrounding the distal vagina and perineum | Distal vaginal support |
Types and Definitions
Prolapse can involve three compartments:
1. Anterior Compartment - Cystocele
A cystocele is the protrusion of the bladder into the vaginal lumen resulting from failure of the pubocervical (vesicovaginal) fibromuscular connective tissue. It may result from a midline (central) defect, a paravaginal (lateral) defect, or a transverse defect. It is the most common type (34.3% prevalence).
2. Posterior Compartment - Rectocele and Enterocele
A rectocele is a protrusion of the rectum into the vaginal lumen resulting from weakness in the muscular wall of the rectovaginal septum (Denonvillier's fascia). It may be associated with defecatory dysfunction such as constipation, tenesmus, and fecal incontinence.
An enterocele is a true hernia of the peritoneal sac (containing small bowel) that enters through a defect in the rectovaginal septum, typically at the vaginal apex.
3. Apical Compartment - Uterine Prolapse and Vault Prolapse
Uterine prolapse (displacement of the uterus into the vaginal canal) typically is not an isolated event and is associated with a variety of pelvic support defects. Following hysterectomy, the vaginal apex must be suspended or the patient will likely develop posthysterectomy vaginal vault prolapse.
Risk Factors
Obstetric:
- Vaginal delivery is the primary risk factor - women with at least one vaginal delivery are twice as likely as nulliparous women to develop POP.
Non-obstetric:
- Age (pelvic floor disorders increase with aging)
- Obesity/increasing weight
- Constipation and chronic straining
- Chronic obstructive pulmonary disease (chronic increased intra-abdominal pressure)
- Prior hysterectomy
- Race
- History of previous prolapse operations
Symptoms
- Vaginal bulge - the hallmark symptom. Vaginal descensus 0.5 cm distal to the hymen most accurately predicts bulge symptoms (sensitivity 69%, specificity 97%). The symptom of a vaginal bulge has an 81% positive predictive value and 76% negative predictive value.
- Lower urinary tract symptoms: urinary incontinence, urgency/frequency, obstructive voiding, urinary retention, upper renal compromise (pain or anuria in severe cases).
- Bowel symptoms: constipation, tenesmus, fecal incontinence, obstructed defecation.
- Pelvic pain, back and flank pain, overall pelvic discomfort.
- Dyspareunia and psychosexual issues.
Women with prolapse beyond the hymen are most likely to report bulge symptoms; more advanced prolapse is actually associated with fewer stress incontinence symptoms and more obstructive voiding (patients may need to manually reduce the prolapse to void).
Only about 10% to 20% of symptomatic women seek medical help.
Evaluation
Physical Examination
The pelvis is divided into compartments for systematic examination:
- Graves speculum or Baden retractor - evaluates the apical compartment.
- Univalve or Sims speculum - placed posteriorly to examine the anterior compartment, and anteriorly to examine the posterior compartment.
- Rectovaginal examination - useful for the posterior compartment to distinguish a posterior vaginal wall defect from a dissecting apical enterocele.
POP-Q (Pelvic Organ Prolapse Quantification) System
The validated POP-Q system is used for objective, standardized measurement of prolapse. It allows the ability to follow prolapse over time and evaluate results of treatment. Nine specific points are measured in relation to the hymenal ring (positive values = beyond hymen, negative values = above hymen):
| Point | Location |
|---|---|
| Aa | Anterior vaginal wall, 3 cm proximal to urethral meatus |
| Ba | Most distal position of anterior vaginal wall |
| C | Most distal edge of cervix or vaginal vault |
| D | Posterior fornix (omitted post-hysterectomy) |
| Ap | Posterior vaginal wall, 3 cm proximal to hymen |
| Bp | Most distal position of posterior vaginal wall |
| gh | Genital hiatus |
| pb | Perineal body |
| tvl | Total vaginal length |
POP-Q Staging:
| Stage | Description |
|---|---|
| 0 | No prolapse demonstrated |
| I | Most distal portion of prolapse is >1 cm above the hymen |
| II | Most distal portion is between −1 cm and +1 cm (at or near hymen) |
| III | Most distal portion is >1 cm beyond hymen but protrudes less than (tvl − 2 cm) |
| IV | Complete or near-complete eversion - most distal portion ≥ (tvl − 2 cm) |
Additional Evaluations
- Bladder function: urodynamics, cystoscopy if indicated
- Bowel function: defecography, colonoscopy as warranted
- Imaging: pelvic floor fluoroscopy and MRI can provide dynamic assessment
Treatment
Nonsurgical / Conservative
Pelvic Floor Muscle Training (PFMT):
- Kegel exercises strengthen the levator ani and pelvic floor muscles.
- Most effective for mild to moderate prolapse; improves symptoms.
Mechanical Devices - Pessaries:
Pessaries are intravaginal devices that mechanically support the pelvic organs. They are available in a wide variety of shapes and sizes:
- Ring, Gellhorn, Donut, Cube, Shaatz, Incontinence Dish - selection depends on degree and type of prolapse.
- Fitting is determined by the degree of prolapse (1st/2nd degree vs. 3rd degree), presence of cystocele or rectocele, and whether urinary incontinence is coexistent.
Surgical Management
The primary aims of surgery are to relieve symptoms and, in most cases, restore vaginal anatomy so that sexual function may be maintained or improved. An individualized, multi-compartmental approach is required based on:
- Previous treatment attempts
- Activity level and health status
- Route (vaginal vs. abdominal)
- Reconstructive vs. obliterative
- Native tissue vs. graft augmentation
Vaginal Procedures:
Apical Compartment:
- Sacrospinous ligament fixation - suspends vaginal apex to the sacrospinous ligament unilaterally or bilaterally.
- Uterosacral ligament suspension - restores high vaginal apical support.
- Uterine-sparing approaches have been studied for appropriate candidates.
Anterior Compartment:
- Anterior vaginal colporrhaphy - central defect repair by plicating pubocervical fascia in the midline.
- Paravaginal repair - reattaches the anterior lateral vaginal sulcus to the obturator internus fascia at the level of the arcus tendineus pelvis ("white line"). Observational studies report 80%-95% success rates.
Posterior Compartment:
- Traditional posterior colporrhaphy - mobilizes Denonvillier's fascia, plicates it in the midline with absorbable (or permanent non-braided) sutures. Perineal body reconstruction is performed if a defective perineum is present.
Abdominal Procedures:
- Abdominal sacrocolpopexy - attaches the vaginal apex to the anterior sacrum (S1-S3) with mesh; considered the gold standard for vault prolapse with the best long-term durability.
- Laparoscopic/robotic sacrocolpopexy - equivalent anatomic and functional outcomes at 12 months with reduced complications and hospital stay.
- Abdominal uterosacral suspension and abdominal/laparoscopic posterior repair.
Obliterative Procedures:
- Colpocleisis (Le Fort procedure) - for women who do not desire future vaginal intercourse; highly effective with low morbidity.
Transvaginal Mesh:
- Use of synthetic mesh has been controversial. The FDA issued warnings regarding vaginal mesh due to complications (erosion, pain, dyspareunia). The decision to use mesh must balance improved anatomic outcomes against risks.
Management of Concurrent Urinary Symptoms:
- Occult stress urinary incontinence may be unmasked after prolapse repair (the "kinking" effect of the prolapsed bladder neck is relieved).
- Consideration of concurrent anti-incontinence procedures (e.g., midurethral sling) should be individualized.
Key Points Summary (from Berek & Novak)
- POP is an increasingly common condition commensurate with an aging population.
- Causes are multifactorial - weakening of pelvic support connective tissue, muscles, and nerve damage.
- Understanding the three levels of pelvic support (DeLancey's levels I, II, III) is essential to identify defects in a consistent and individualized manner.
- Physical examination requires thoughtful attention to all vaginal compartments plus levator muscle and anal sphincter complex; the validated POP-Q system allows objective longitudinal follow-up.
- Nonsurgical treatment options include pelvic floor muscle training and intravaginal devices.
- Surgical treatment involves an individualized, multicompartmental approach with increasing level I evidence to guide treatment.
Berek & Novak's Gynecology, Chapter 30 (Pelvic Organ Prolapse), pp. 1593-1650
Detailed description of each surgeries (steps) in pelvic organ prolapse
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from Berek & Novak. Let me compile the complete surgical description:
Surgical Procedures for Pelvic Organ Prolapse - Step-by-Step
Source: Berek & Novak's Gynecology, Chapter 30
Overview: Categories of Surgery
Procedures for POP are broadly grouped into three types:
- Reconstructive - use the patient's own (native) endogenous support structures
- Compensatory/Augmentation - replace deficient support with permanent graft/mesh material
- Obliterative - close or partially close the vagina
The surgical route is chosen based on type and severity of prolapse, surgeon training and experience, patient preference, and expected surgical outcome.
I. VAGINAL PROCEDURES - APICAL COMPARTMENT
1. Sacrospinous Ligament Fixation (SSLF)
Overview: Suspension of the vaginal apex to the sacrospinous ligament (the tendinous component of the coccygeus muscle). First described in 1958. Success for apical support: 89%-97%.
Steps:
- Patient positioning: Dorsal lithotomy with Trendelenburg.
- Incision: A midline posterior vaginal wall incision is made from the vaginal apex to the perineal body.
- Access: The rectovaginal space is entered and dissected bluntly in an extraperitoneal manner. The pararectal space (through the Denonvillier fascia) is penetrated at the level of the ischial spine to expose the coccygeus muscle and sacrospinous ligament lateral and posterior to the rectum.
- Identification of ligament: The sacrospinous ligament runs from the ischial spine to the lateral sacrum and coccyx. It is palpated and identified with direct visualization or with retractors (e.g., Breisky-Navratil).
- Suture placement: Two permanent or delayed absorbable sutures are placed through the sacrospinous ligament, typically 1.5-2 cm medial to the ischial spine (to avoid the pudendal nerve and vessels which run just medial/posterior to the ischial spine). Various suture carriers (e.g., Miya hook, Deschamps needle, or Capio device) are used to place sutures into the ligament.
- Attachment to vagina: The free ends of the sutures are attached to the fibromuscular layer of the posterior vaginal apex with large bites.
- Tying sutures: The sutures are tied after repair of any concurrent anterior compartment defect. This pulls the vaginal apex up to the level of the sacrospinous ligament, producing a characteristic posterior and lateral deflection of the vaginal axis.
- Concurrent repair: Anterior colporrhaphy and perineal repair are performed as needed.
- Closure: The vaginal epithelium is closed with absorbable sutures.
Key points:
- Usually performed on the right side (unilateral) for easier access via the right ischiorectal fossa.
- The procedure creates a posterior vaginal deflection, which may predispose to subsequent anterior compartment prolapse - so the anterior wall must also be addressed.
- Risk of sciatic or pudendal nerve injury if sutures are placed too laterally.
2. Uterosacral Ligament Suspension (ULS)
Overview: Suspension of the vaginal apex to the uterosacral ligament (USL) remnants at or above the level of the ischial spine. Success rates excellent in observational studies (302 participants).
Steps:
- Entry: Via the vaginal cuff after hysterectomy, or through a transverse incision at the vaginal cuff for vault prolapse, or rarely through a posterior colpotomy for uterine conservation.
- Exposure: The pelvic sidewall lateral to the sigmoid colon is exposed using Breisky-Navratil retractors and a pack to hold the small bowel cephalad and place the sigmoid colon and sidewall peritoneum on stretch.
- Identify the USL: After palpation of the ischial spine, the uterosacral ligament remnant is found adjacent to the pelvic sidewall peritoneum, just cephalad to the palpable ischial spine. The ligament is often found as a firm band running from the sacrum to the vaginal apex/cervix.
- Suture placement: Permanent sutures (0 or 1-polypropylene) are placed through the peritoneum and the adjacent uterosacral ligament, approximately 1 cm cephalad to and at the same posterior level as the ischial spines. Up to three sutures are placed in each ligament (bilateral). Traction on the sutures and palpation confirms firm attachment to the ligamentous structures. Sutures are tagged for later use.
- Posterior repair: The peritoneum is dissected off the posterior vaginal fibromuscular wall at the cuff. If a rectovaginal enterocele is present, it is dissected, reduced, and closed by approximating the prerectal fascia or anterior rectal wall to the posterior fibromuscular vaginal tissue just caudal to the suspension suture sites.
- Suture incorporation: The suspension sutures are secured with large bites into both the posterior and anterior fibromuscular tissue of the vaginal apex, then locked in place, approximating anterior to posterior connective tissue and fixing the suture to the vaginal apex. For large vaginal cuffs, a second delayed absorbable suture may be added on each side.
- Cuff closure: Absorbable cuff closure sutures are placed at each cuff angle. Approximation of anterior to posterior vaginal cuff is done over the suspension suture sites. A box stitch of the central cuff anterior to the posterior fibromuscular tissue may be performed when indicated. The running closure hides the suspension suture knots.
- Cystoscopy (MANDATORY): Intraoperative cystoscopy is performed after every ULS to confirm bilateral ureteral patency - ureteral obstruction from kinking or suture incorporation occurs in approximately 2%-3% of cases (as high as 11% intraoperative kinking reported). Any ureteral obstruction must be corrected before closing.
Note: Some surgeons approximate the ligaments in the midline to close the cul-de-sac and prevent enterocele. Others leave the cul-de-sac open to avoid impairing bowel function.
3. Iliococcygeal Vaginal Suspension
Overview: Attachment of the vaginal apex bilaterally to the iliococcygeus muscle and fascia. Fewer case series than SSLF but comparable cure rates.
Steps:
- Incision: Midline posterior vaginal wall incision, extraperitoneal access via the posterior vagina.
- Dissection: The ischial spine is used as a landmark to identify both the sacrospinous ligament and the iliococcygeal fascia (anteriorly and caudad to the ligament).
- Suture placement: A polydioxanone (PDS) suture is placed through the iliococcygeal fascia (not the sacrospinous ligament itself) and attached to the vaginal apex as a pulley stitch.
- Bilateral approach: This procedure is more easily performed bilaterally than SSLF (less tension per side) and is preferred when the vagina is shortened, as it applies less tension.
- Advantages: Lower risk of major vessel, nerve, or ureteral injury compared with other transvaginal suspensions.
II. VAGINAL PROCEDURES - ANTERIOR COMPARTMENT
4. Anterior Vaginal Colporrhaphy (Central Defect Repair)
Overview: Repair of a midline (central) fascial defect causing cystocele. Addresses failure of pubocervical (vesicovaginal) fascia.
Steps:
- Hydrodissection: Dilute vasopressin or saline is injected subepithelially along the anterior vaginal wall to aid dissection.
- Incision: A midline longitudinal incision is made in the anterior vaginal wall from the bladder neck to within 1-2 cm of the vaginal apex. Alternatively, a diamond-shaped incision removes a wedge of redundant epithelium.
- Dissection of flaps: The vaginal epithelium is sharply and bluntly dissected off the underlying pubocervical (vesicovaginal) fibromuscular layer bilaterally using Metzenbaum scissors. The dissection extends laterally toward the arcus tendineus fascia pelvis (ATFP, "white line").
- Identify fascial defect: The pubocervical fascia is inspected for midline defects, tears, or attenuation. The bladder may be visible through thin or absent fascia.
- Fascial plication: The pubocervical fibromuscular tissue is plicated in the midline using delayed absorbable sutures (e.g., 2-0 Vicryl) placed in interrupted or running fashion. This imbrication reinforces the fascial layer and elevates the bladder.
- Excess epithelium excision: Redundant vaginal epithelium is trimmed (not excessively - to avoid narrowing the vagina).
- Closure: The vaginal epithelium is closed with a running locked or interrupted absorbable suture.
- Apical suspension: Apical suspension must be performed concurrently - failure to address the apex greatly increases the risk of recurrent anterior prolapse.
Limitations: Observational and randomized studies show recurrence rates of 20%-30% with native tissue repair alone.
5. Paravaginal (Lateral Defect) Repair
Overview: Reattachment of the anterior lateral vaginal sulcus to the obturator internus fascia at the level of the arcus tendineus fascia pelvis (ATFP, "white line"). Addresses lateral/paravaginal detachment. Reported success: 80%-95%.
Steps:
- Access: Can be performed transvaginally, retropubically (abdominal), or laparoscopically.
- Transvaginal approach: Following the anterior colporrhaphy incision and lateral dissection, the areolar tissue of the retropubic space (space of Retzius) is entered by blunt dissection through the endopelvic fascia lateral to the bladder.
- Identify the ATFP: The arcus tendineus fascia pelvis is identified as a white fibrous band running from the pubic bone to the ischial spine along the pelvic sidewall (the obturator internus fascia).
- Identify the detachment: Most women with anterolateral detachments have separation of the upper vaginal fornices from the ATFP immediately adjacent to the ischial spine. These specific areas must be resuspended.
- Suture placement: Interrupted permanent or delayed absorbable sutures are placed from the lateral vaginal sulcus (including the fibromuscular layer) to the obturator internus fascia/ATFP at multiple points from the ischial spine to the pubic symphysis (usually 4-6 sutures per side).
- Tying: Sutures are tied sequentially from most distal to most proximal, restoring the normal lateral attachment of the vagina to the pelvic sidewall.
Note: When large central defects coexist with lateral defects, combining techniques can be challenging (opposing tension on suture lines). Options include: extensive central repair with apical support procedure, or placement of a graft spanning the entire anterior vaginal plate.
III. VAGINAL PROCEDURES - POSTERIOR COMPARTMENT
6. Traditional Posterior Colporrhaphy
Overview: Repair of posterior vaginal wall defect (rectocele) by plicating the Denonvillier (rectovaginal) fascia in the midline. First described with pubococcygeus muscle plication; subsequently modified to preserve sexual function.
Steps:
- Perineal incision: A transverse incision is made at the posterior fourchette/perineal body. This is connected to a midline vertical incision extending from the perineal body to the vaginal apex or to the cephalad border of the rectocele.
- Flap development: The vaginal epithelium is sharply and bluntly dissected off the underlying Denonvillier fascia (rectovaginal fascia/septum) bilaterally, leaving as much of this fibromuscular tissue as possible attached laterally to the levator fascia. The dissection is carried laterally to the levator ani muscles.
- Rectal wall repair: Any obvious defects in the rectal muscularis are directly repaired first.
- Fascial plication: The Denonvillier fascia is plicated in the midline using interrupted or continuous sutures. The authors of Berek & Novak prefer delayed absorbable sutures for this plication. Permanent non-braided suture may also be used - braided permanent sutures carry greater risk of stitch infection and granulation tissue formation.
- Excess epithelium: Redundant vaginal epithelium is trimmed and closed with absorbable sutures.
- Perineal body reconstruction: When a defective perineal body or perineal membrane is present, reconstruction follows posterior colporrhaphy. The superficial perineal muscles and bulbocavernosus fascia are plicated in the midline. The skin is closed as in an episiotomy repair. Detachments of the inferior portion of the levator ani from the perineal body may also be repaired.
Key: The Denonvillier fascia is mobilized off the vaginal epithelium - not removed - to preserve as much fibromuscular support as possible.
7. Enterocele Repair
Overview: Repair of a true peritoneal hernia sac entering through the rectovaginal septum. May be approached vaginally, abdominally, or laparoscopically.
Steps:
- Identification: The enterocele sac (containing small bowel covered by peritoneum) is identified beneath the posterior vaginal epithelium, usually at the vaginal apex.
- Opening the sac: The peritoneum of the enterocele sac is opened, the small bowel contents reduced into the abdominal cavity.
- Management - one of four approaches:
- (a) Removal of the peritoneal sac with closure of the peritoneal defect, followed by repair of the fascial/fibromuscular defect below it.
- (b) Dissection and reduction of the peritoneal sac with closure of the defect (high ligation).
- (c) Obliteration of the peritoneal sac from within via transabdominal Halban or Moschcowitz procedures, or transvaginal McCall or Halban procedures (closing the cul-de-sac with concentric or sagittal purse-string sutures through the uterosacral ligaments, posterior vagina, and anterior rectal wall).
- (d) If the posterior vaginal wall is significantly elongated and enlarged, excision of that area to establish acceptable vaginal length and eliminate redundancy.
- Upper vaginal wall: Any attenuated fibromuscular upper vaginal wall is repaired or covered with graft material. If severely attenuated, removal of that portion of the upper vaginal wall is considered.
- Apical suspension: The vaginal cuff (or cervix) is suspended without excessive tension.
- Defect closure: Any defect in attachment of the upper vagina to the rectum at or below the sigmoid junction is corrected.
IV. ABDOMINAL PROCEDURES
8. Abdominal Sacrocolpopexy
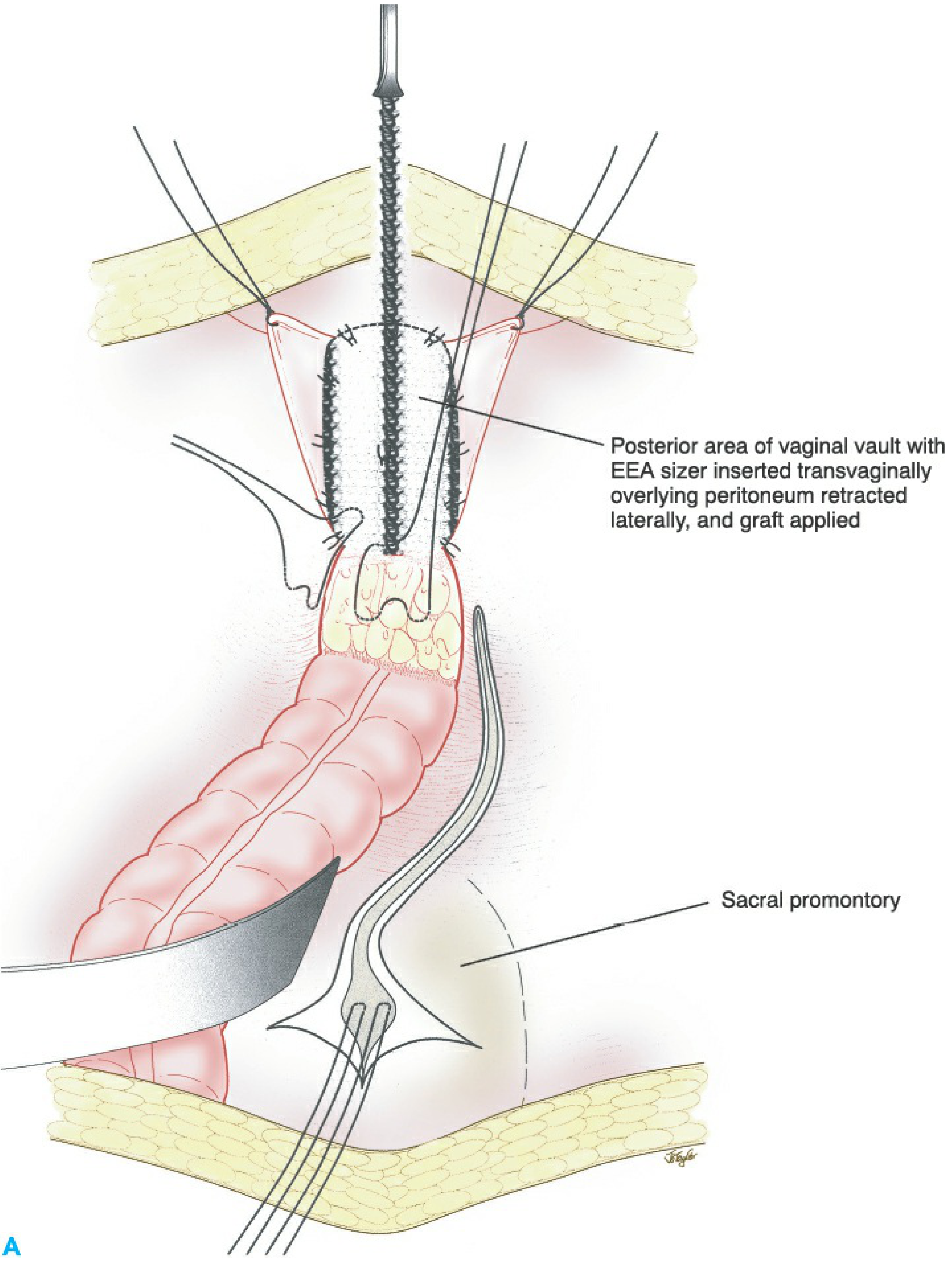
Overview: Attachment of the vaginal apex (and anterior/posterior walls) to the anterior longitudinal ligament of the sacrum using graft material. Considered the gold standard for apical prolapse, especially vault prolapse. Cure rates for apical prolapse: 78%-100% (most >90%).
Steps:
- Incision: Lower midline or Pfannenstiel laparotomy incision. The patient is placed in Trendelenburg with bowel packed out of the pelvis.
- Peritoneal dissection: The peritoneum overlying the vaginal apex and posterior vagina is incised and flapped laterally. The retroperitoneal space is developed to expose the anterior and posterior vaginal walls.
- Anterior vaginal wall dissection: The bladder is dissected off the anterior vaginal wall, exposing the anterior fibromuscular vaginal wall down to the level of the bladder neck.
- Posterior vaginal wall dissection: The peritoneum is dissected off the posterior vaginal wall distally toward (or to) the rectovaginal junction or the rectal-sigmoid junction.
- Presacral space development: The peritoneum overlying the sacral promontory is incised. The presacral space is carefully developed, identifying and protecting the right ureter, the middle sacral artery and vein, and the iliac vessels. The anterior longitudinal ligament of the sacrum (at S1-S3) is exposed - the attachment site for the graft.
- Graft preparation: A Y-shaped or two-piece synthetic mesh (typically macroporous polypropylene, type I) is prepared. The two arms of the graft are attached to the anterior and posterior vaginal walls.
- Anterior graft attachment: The anterior limb of the graft is sutured to the anterior vaginal fibromuscular wall with multiple permanent or delayed absorbable sutures placed in the fibromuscular tissue (avoiding full-thickness passage through the vaginal epithelium to reduce erosion risk). The graft extends from the level of the bladder neck to the vaginal apex.
- Posterior graft attachment: The posterior limb is sutured to the posterior vaginal fibromuscular wall, from the vaginal apex distally to or below the rectosigmoid junction. The overlying peritoneum is flapped laterally during this step.
- Sacral fixation: The apex of the Y-graft (or proximal end of the joined graft) is attached under appropriate (not excessive) tension to the anterior longitudinal ligament of the sacrum (usually at S1) using permanent sutures (polypropylene or similar). Small-gauge monofilament sutures are preferred, placed into the fibromuscular tissue - not full thickness - to prevent erosion.
- Culdoplasty/Enterocele prevention: The cul-de-sac is obliterated using a Halban or Moschcowitz procedure (box closure of the cul-de-sac peritoneum lateral to the sigmoid, attachment of the presigmoid fat to the graft centrally) to treat or prevent enterocele/sigmoidocele.
- Reperitonealization: The graft is covered by retroperitoneum - the peritoneum is re-approximated over the graft through the right side of the cul-de-sac. This is important to reduce adhesion formation and bowel obstruction risk.
- Cystoscopy: Bilateral ureteral patency is confirmed.
- Closure: Fascia and skin are closed in layers.
To prevent graft erosion:
- Preoperative tissue optimization with vaginal estrogen and treatment of any vaginitis.
- Use small-gauge monofilament sutures placed in fibromuscular tissue only.
- Excise portions of thin, avascular vaginal apex if necessary before attaching graft.
- Avoid graft placement across a concurrent hysterectomy suture line.
- Use macroporous polypropylene mesh (type I) - less porous grafts like GORE-TEX have higher infection and erosion rates.
Complications: Mesh/suture erosion (3.4%), intraoperative hemorrhage from presacral venous plexus (4.8%), postoperative ileus (3.6%), small bowel obstruction requiring reoperation (1.1%), intra-abdominal adhesions, wound complications (4.6%), mesh erosion probability at 7 years: 10.5%.
9. Abdominal Uterosacral Ligament Suspension
Overview: Plication or reattachment of the uterosacral ligaments to support the vaginal apex at the time of abdominal hysterectomy or as a separate procedure. Described prophylactically during hysterectomy or therapeutically for vaginal apex suspension.
Steps:
- Access: Via laparotomy or laparoscopy. The cul-de-sac is entered and the uterosacral ligaments are identified bilaterally.
- USL identification: The uterosacral ligaments are identified at their insertion on the sacrum and traced to the cervix/vaginal apex.
- Suture placement: Multiple permanent or delayed absorbable sutures are placed into the uterosacral ligaments.
- Vaginal attachment: The sutures are incorporated into the anterior and posterior fibromuscular layer of the vaginal apex.
- Cul-de-sac closure: Some surgeons approximate the ligaments in the midline to prevent enterocele. Others leave it open to avoid impairing bowel function.
- Cystoscopy (MANDATORY): Performed after every abdominal/laparoscopic USL suspension to confirm ureteral patency.
10. Laparoscopic and Robotic Sacrocolpopexy
Overview: Laparoscopic or robotic-assisted replica of the open abdominal sacrocolpopexy. Evidence shows equivalent anatomic and functional outcomes at 12 months, with reduced complications and shorter hospital stay compared to open approach.
Steps:
The steps mirror the abdominal sacrocolpopexy, performed through laparoscopic or robotic ports:
- Trendelenburg positioning; laparoscopic access (4-5 ports).
- Peritoneal dissection over vaginal apex and posterior vagina using laparoscopic scissors/energy devices.
- Anterior dissection of bladder off anterior vaginal wall.
- Development of presacral space over the sacral promontory.
- Graft (synthetic mesh) preparation, cut to appropriate shape.
- Anterior vaginal attachment with laparoscopic sutures or tacking devices.
- Posterior vaginal attachment.
- Sacral fixation at S1 anterior longitudinal ligament with permanent sutures.
- Culdoplasty (Halban or Moschcowitz) laparoscopically.
- Reperitonealization of the mesh.
- Laparoscopic cystoscopy to confirm ureteral patency.
Robotic approach: Uses microprocessor-assisted laparoscopy (da Vinci system) for enhanced dexterity - comparable outcomes to standard laparoscopy.
11. Abdominal/Laparoscopic Posterior Repair (Enterocele Repair)
Steps:
- Identify the cul-de-sac enterocele or rectocele through abdominal approach.
- Obliterate the cul-de-sac with Halban culdoplasty (sagittal sutures from anterior rectal wall to posterior vaginal wall, closing the cul-de-sac) or Moschcowitz culdoplasty (concentric purse-string sutures in the cul-de-sac, incorporating the uterosacral ligaments, posterior vaginal wall, and anterior rectal serosa).
- Posterior repair and enterocele sac excision or high ligation as described in vaginal approach.
V. OBLITERATIVE PROCEDURES
12. Colpocleisis / Partial Colpocleisis (Le Fort Procedure)
Overview: Partial or total closure of the vagina. Appropriate for debilitated patients who do not desire vaginal function and cannot tolerate longer reconstructive procedures. Case series report success rates as high as 100%. Regret after the procedure is rare.
Steps (Partial Colpocleisis / Le Fort):
- Marking: Rectangular strips of vaginal epithelium are marked on both the anterior and posterior vaginal walls, with lateral drainage channels preserved on each side.
- Epithelium removal: The marked rectangular strips of vaginal epithelium are excised from the anterior and posterior vaginal walls. The lateral channels (strips of intact epithelium) are preserved on each side to allow drainage of any cervical or uterine secretions.
- Approximation: The raw denuded anterior and posterior vaginal walls are approximated (sutured together) using multiple rows of interrupted or continuous delayed absorbable sutures, starting from the apex and working toward the introitus. This creates a sealed channel obliterating the vaginal lumen.
- High perineorrhaphy: A high perineorrhaphy is always included - the perineal body is reconstructed to narrow the genital hiatus.
- Puborectalis plication: The puborectalis muscles are plicated in the midline to reinforce posterior support, reduce the genital hiatus, and decrease the chance of recurrent prolapse.
- Skin closure: Perineal skin is closed.
Total colpectomy (all vaginal epithelium removed from hymen posteriorly to within 0.5-2 cm of the external urethral meatus anteriorly) is an option when even more complete obliteration is desired.
Modified colporrhaphy approach: In cases where most defects are anterior and posterior, a modified anterior and posterior colporrhaphy removes large portions of both vaginal walls and closes them, creating a narrow (1-2 cm diameter) cylindrical vaginal remnant. This is augmented by extensive perineorrhaphy and puborectalis plication.
Important considerations:
- If hysterectomy is performed concurrently, blood loss is greater and operative time is longer.
- Preoperative evaluation for stress urinary incontinence and voiding dysfunction is essential - midurethral slings may be added concurrently.
- The patient must be fully counseled that vaginal intercourse will not be possible after the procedure. Regret is rare but should be thoroughly discussed preoperatively.
Summary Comparison Table
| Procedure | Route | Target Compartment | Approach | Key Step |
|---|---|---|---|---|
| Anterior colporrhaphy | Vaginal | Anterior | Native tissue | Midline fascial plication |
| Paravaginal repair | Vaginal/abdominal/laparoscopic | Anterior | Native tissue | Lateral sulcus to ATFP |
| Posterior colporrhaphy | Vaginal | Posterior | Native tissue | Denonvillier fascia plication |
| Enterocele repair | Vaginal/abdominal | Apical/posterior | Native tissue | Peritoneal sac excision + high ligation |
| Sacrospinous fixation | Vaginal | Apical | Native tissue | Apex to sacrospinous ligament |
| Uterosacral suspension | Vaginal | Apical | Native tissue | Apex to USL; MANDATORY cystoscopy |
| Iliococcygeal suspension | Vaginal | Apical | Native tissue | Apex to iliococcygeal fascia bilaterally |
| Abdominal sacrocolpopexy | Abdominal/laparoscopic/robotic | Apical | Mesh | Apex + vaginal walls to sacral ligament |
| Abdominal USL suspension | Abdominal/laparoscopic | Apical | Native tissue | USL plication/reattachment |
| Colpocleisis | Vaginal | All compartments | Obliterative | Denudation + approximation of vaginal walls |
Berek & Novak's Gynecology, Chapter 30 (pp. 1620-1645). Authors: Ballard AV, Meyer I, Varner RE, Gleason JL, Richter HE.
This is a shared conversation. Sign in to Orris to start your own chat.