Aortic stenosis
Reading File
Finding Sources
Searching PubMed
"aortic stenosis"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"aortic stenosis" AND "transcatheter aortic valve"
Finding Sources
Finding Sources
Finding Sources
Searching the Web
aortic stenosis pathophysiology diagnosis management guidelines 2024 2025
Finding Sources
Reading Web Page
https://123sonography.com/blog/news/highlights-updates-escea…
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple sources. Let me compile the full answer.
Aortic Stenosis
Overview
Aortic stenosis (AS) is obstruction to LV outflow across the aortic valve. It is the most common valvular heart disease in the developed world, present in ~15% of adults aged ≥65 years, and severe (AVA <1 cm²) in ~2%. Prevalence rises to ~3% by age 75.
Etiology
| Type | Features |
|---|---|
| Calcific/Degenerative | Most common in adults >65. Calcium deposits on normal tricuspid cusps, causing progressive obstruction |
| Congenital Bicuspid Valve | 1-2% of population; affects 66% of patients. Severe AS develops 1-2 decades earlier than in tricuspid valves. Often associated with aortic root dilation - risk of dissection/rupture |
| Rheumatic | Rare in Western countries. Results from fusion of commissures. Usually coexists with MS |
- Braunwald's Heart Disease, p. 1036
- Grainger & Allison's Diagnostic Radiology, p. 338
Pathophysiology
Thickening and calcification of valve leaflets leads to progressive obstruction to LV outflow. The LV compensates with concentric hypertrophy (pressure overload pattern), which:
- Maintains systolic function initially
- Increases LV end-diastolic pressure -> diastolic dysfunction
- Makes the LV noncompliant and highly dependent on atrial kick for filling (hence AF is very poorly tolerated)
- Eventually reduces LV compliance and stroke volume
The three classic symptoms arise through distinct mechanisms:
| Symptom | Mechanism | Mortality if untreated |
|---|---|---|
| Angina | Increased O₂ demand (hypertrophied LV) + decreased coronary perfusion time | 50% 5-year mortality |
| Syncope | Fixed CO unable to meet demands on exertion; also baroreceptor reflex miscommunication | 50% 3-year mortality |
| Dyspnea/HF | Elevated LVEDP -> pulmonary congestion | 50% 2-year mortality |
- Symptom to Diagnosis, p. 9340
Clinical Features
Murmur: Harsh, crescendo-decrescendo (diamond-shaped) systolic ejection murmur, best heard at the right 2nd intercostal space, radiating to the carotids. Typically grade III/VI or louder in severe AS. Note: ~31% of patients with moderate-severe AS may not have a detectable murmur.
Pulse: Slow-rising, low-volume pulse ("pulsus parvus et tardus") - though this sign is less reliable in elderly patients with arterial stiffening.
Heart sounds: S2 may be softened or absent when calcification is extensive.
Other late features:
- Atrial fibrillation (poorly tolerated - LV relies on atrial kick)
- Acquired von Willebrand deficiency (large vWF multimers disrupted by turbulent flow across stenotic valve) - presents as GI bleeding (Heyde syndrome)
Diagnosis
Echocardiography (first-line)
Doppler echo is the gold standard. Key parameters:
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Peak velocity (m/s) | <3.0 | 3.0-4.0 | ≥4.0 |
| Mean gradient (mmHg) | <20 | 20-40 | ≥40 |
| AVA (cm²) | >1.5 | 1.0-1.5 | <1.0 |
| AVA indexed (cm²/m²) | - | - | <0.6 |
AVA is calculated by the continuity equation (principle of conservation of flow):
EOA = (SV of LVOT) / (VTI across aortic valve)
Low-flow, low-gradient AS (LFLG-AS) - an important and challenging subset:
- Valve area <1 cm² but mean gradient <40 mmHg
- Occurs when LV stroke volume index is <35 mL/m²
- More common in women with small LV cavities and in AF
- Must distinguish true severe (low flow due to poor LV function) from pseudo-severe (moderate AS that appears severe at low flow)
- Use dobutamine stress echo OR cardiac CT calcium scoring: an Agatston score ≥1600 in men / ≥1200 in women confirms severe AS without needing stress echo (2025 ESC/EACTS update)
Braunwald's Heart Disease, p. 1036
Chest X-ray
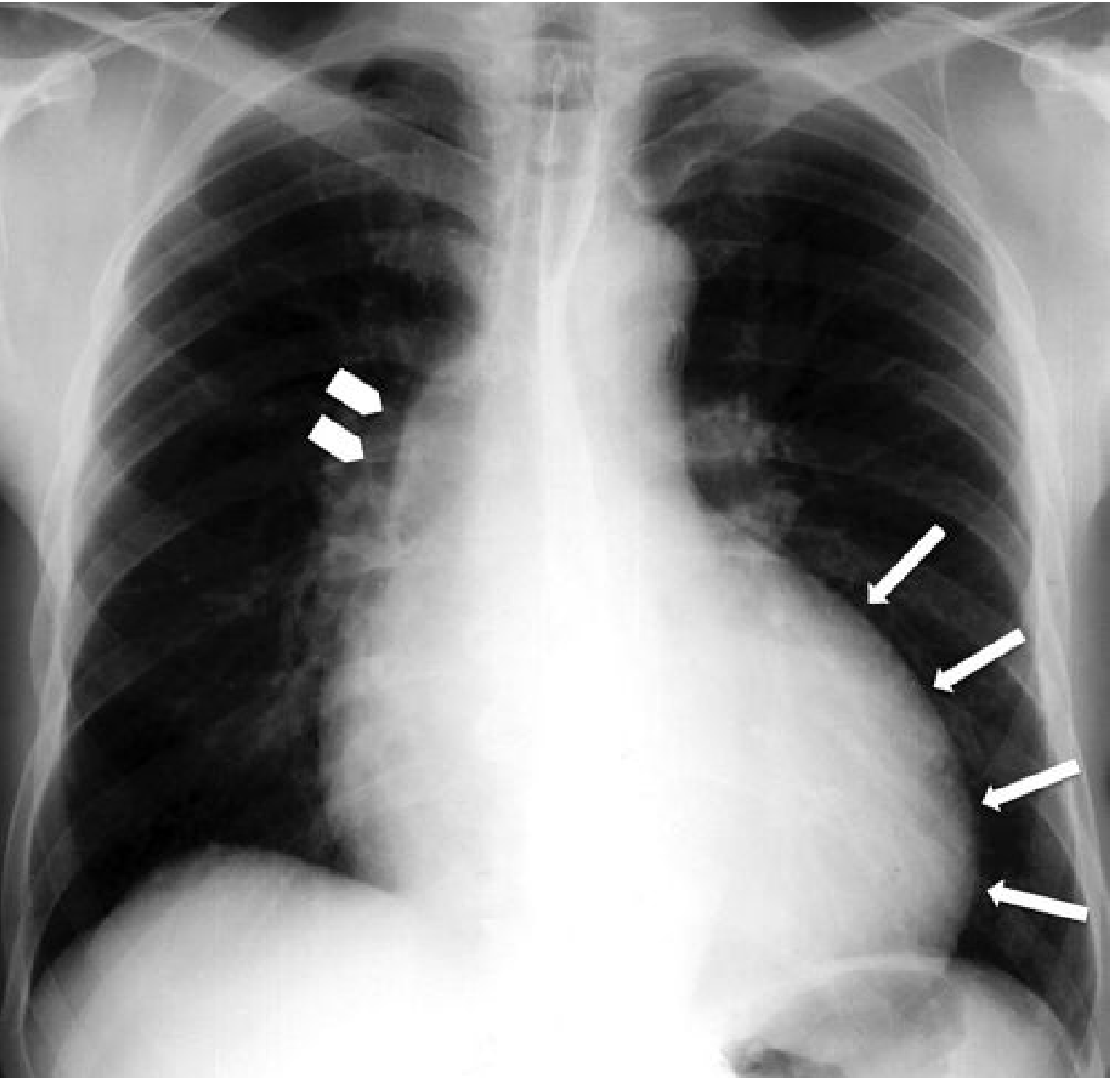
- Rounding of LV apex (LVH)
- Poststenotic dilation of the ascending aorta
- Aortic valve calcification visible on lateral view
Echocardiogram (B-mode)
Cardiac CT
- Excellent for calcium scoring (Agatston score)
- Allows direct planimetry of the valve orifice
- Essential for pre-TAVR anatomy assessment (annulus sizing, coronary ostia height, access)
- Agatston score of 150 is 100% sensitive for discriminating velocities <2.5 m/s from >2.5 m/s
CMR
- Direct planimetry of valve orifice possible
- Less sensitive than CT for calcium detection
- Useful adjunct when echo is suboptimal
Management
Medical Therapy
There is no proven medical therapy that slows progression or replaces valve intervention once symptoms develop. Statins were trialed but did not reduce disease progression. Symptomatic patients who refuse or cannot undergo intervention should receive:
- Diuretics cautiously for HF symptoms (avoid over-diuresis given diastolic dysfunction)
- ACE inhibitors/ARBs - can be used cautiously; avoid vasodilators that precipitate hypotension
- Rate control for AF (these patients are preload-dependent)
Intervention Indications
Class I - Intervention is indicated:
- Symptomatic severe AS (dyspnea, angina, syncope) - this is the primary indication regardless of age or LV function
- Asymptomatic severe AS with LVEF <50%
- Asymptomatic severe AS undergoing cardiac surgery for another reason
Class IIa (2025 ESC/EACTS update):
- Early intervention is a reasonable option vs. watchful waiting in asymptomatic severe AS with normal LVEF
- Asymptomatic patients with peak velocity ≥5.5 m/s or very rapid progression (velocity increase >0.3 m/s per year) - intervention recommended even without symptoms
TAVR vs. SAVR
| Patient Profile | Preferred Approach |
|---|---|
| High/prohibitive surgical risk | TAVR (any age) |
| Age >80 or life expectancy <10 years | TAVR |
| Age 65-80, low-intermediate surgical risk | Shared decision-making; TAVR or SAVR both acceptable |
| Age <65-70, low surgical risk | SAVR preferred (concern for long-term valve durability with TAVR) |
| Symptomatic, any age, high surgical risk + expected survival >12 months with acceptable QoL | TAVR |
Key TAVR evidence:
- PARTNER trial (inoperable patients, mean age 83): 1-year mortality 30% TAVR vs. 50% medical therapy
- PARTNER low-risk trial: composite of death, stroke, or hospitalization at 1 year 8.5% (TAVR) vs. 15.1% (SAVR)
- Registry data: 30-day TAVR mortality has declined from 4% to 2% over time
TAVR risks vs. SAVR: Higher risk of stroke (though declining), vascular complications, permanent pacemaker need, and paravalvular leak. Lower risk of new-onset AF and shorter hospital stay.
- Braunwald's Heart Disease, p. 1036
2025 ESC/EACTS Guideline Update (Key Changes)
- CT calcium scoring elevated to same level as dobutamine stress echo for LFLG-AS workup
- Stronger recommendation for early intervention in asymptomatic patients (2A)
- Continued 2A recommendation for high-risk asymptomatic patients (peak velocity ≥5 m/s)
- TAVR expanded for intermediate-risk patients (previously required high risk)
- For patients <70 at low surgical risk, SAVR remains preferred
Prognosis
Once symptoms develop, prognosis without intervention is poor (see table above). After successful AVR or TAVR, 5-year survival approaches that of age-matched controls. Bioprosthetic valve deterioration is slower in older patients, making repeat intervention less likely within their remaining lifespan.
Recent literature note: A 2025 JACC review on TAVR beyond severe AS (PMID 40044299) discusses expanding TAVR indications to moderate AS in HF patients - an evolving area to watch.
Hand drawn diagrams for examination
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.