Lynphomas
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have enough comprehensive information from authoritative textbooks to write a thorough response on lymphomas. Let me compile the full answer.
Lymphomas - Comprehensive Overview
Lymphomas are malignant neoplasms of lymphoid cells. They are broadly divided into two major groups: Hodgkin Lymphoma (HL) and Non-Hodgkin Lymphoma (NHL). The distinction matters clinically because behavior, staging, and treatment differ significantly.
Normal Counterparts - Origin of Lymphomas
Understanding where in lymphoid differentiation a lymphoma arises explains its biology:
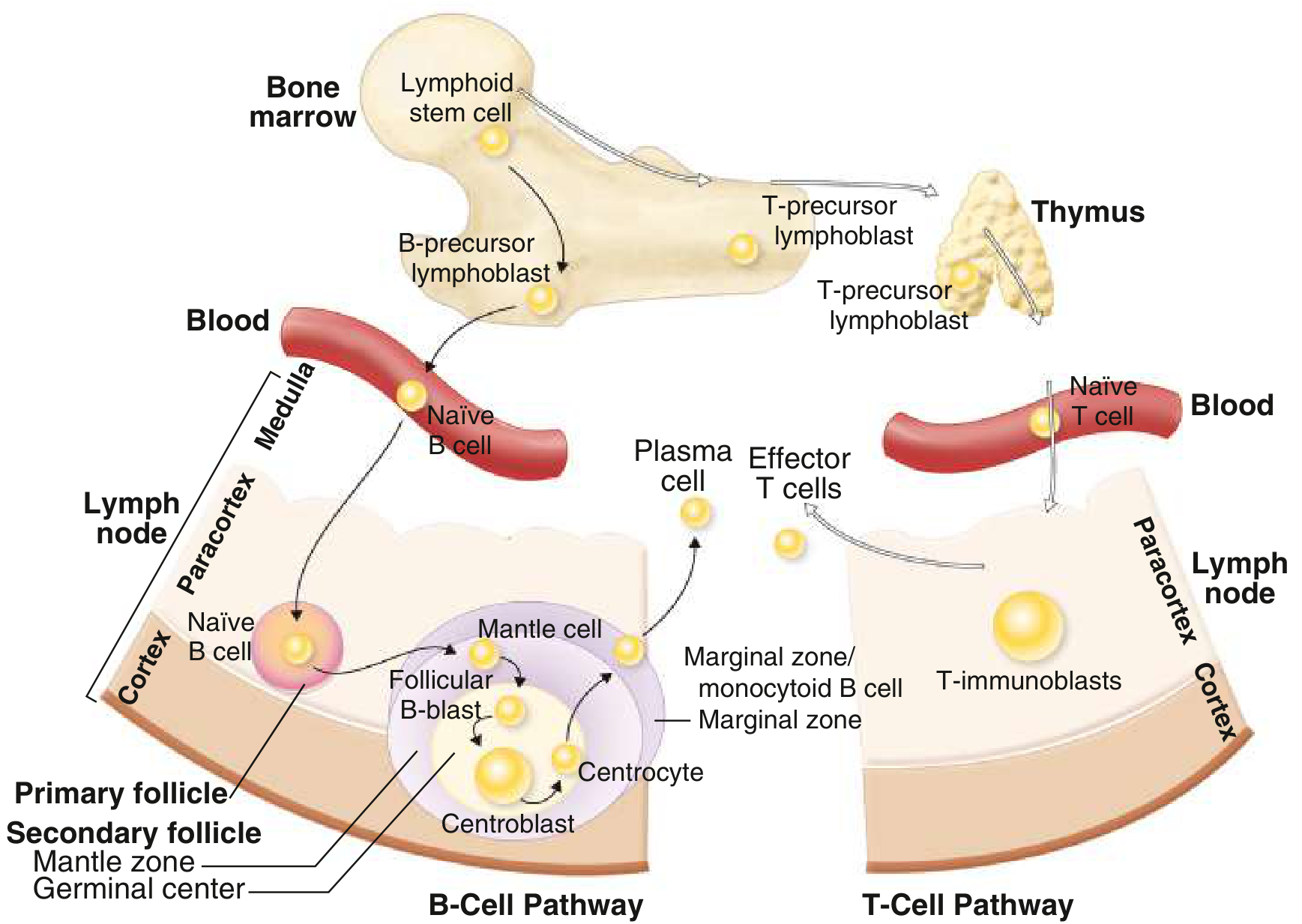
Postulated normal counterparts of B- and T-cell malignancies. Lymphoid stem cells in bone marrow differentiate into B-cell precursors (cortex/germinal center) or T-cell precursors (thymus), giving rise to specific lymphoma subtypes at each stage.
I. CLASSIFICATION
WHO Classification (2016/Updated)
The WHO classification integrates morphology, immunophenotype, cytogenetics, and clinical behavior. Lymphomas are divided by:
- Cell of origin: B-cell vs. T/NK-cell
- Maturity: Precursor (immature) vs. peripheral (mature/post-thymic)
-
In the US and Europe, 85-90% of NHLs are B-cell in origin
-
Most frequent NHL worldwide: Diffuse Large B-Cell Lymphoma (DLBCL) ~30%
-
Second most frequent: Follicular Lymphoma ~20%
-
Less common types (~5-10% each): Extranodal marginal zone/MALT, Peripheral T-cell, Small Lymphocytic Lymphoma (SLL), Mantle Cell Lymphoma
-
Goldman-Cecil Medicine, p. 1951
II. EPIDEMIOLOGY & RISK FACTORS
Autoimmune and Inflammatory Conditions
- Rheumatoid arthritis: 2-fold increased NHL risk
- Sjögren syndrome: 30-40 fold increased marginal zone lymphoma risk
- Hashimoto thyroiditis: increased thyroid lymphoma risk
- Celiac disease: associated with enteropathy-type T-cell lymphoma
Infectious Agents
| Agent | Associated Lymphoma |
|---|---|
| EBV | Burkitt lymphoma (>95% endemic form), post-transplant lymphoproliferative disorders, DLBCL of elderly, NK/T-cell lymphoma |
| HTLV-1 | Adult T-cell leukemia/lymphoma (virtually all cases) |
| HHV-8 | Primary effusion lymphoma (immunocompromised) |
| Hepatitis C virus | Lymphoplasmacytic lymphoma, marginal zone lymphoma |
| H. pylori | Gastric MALT lymphoma |
| Borrelia burgdorferi | Marginal zone B-cell lymphoma of skin |
Environmental Factors
-
Agricultural chemicals (phenoxy herbicides/Agent Orange), ionizing radiation, organic solvents, high-fat diet, ultraviolet radiation
-
Prior treatment for Hodgkin lymphoma: 20-fold increased NHL risk
-
Heavy smoking: increased follicular lymphoma risk
-
Goldman-Cecil Medicine, pp. 845-864
III. NON-HODGKIN LYMPHOMAS (NHL)
A. B-Cell NHLs
1. Follicular Lymphoma
- ~20% of all NHLs; more common in North America and Western Europe
- Cell of origin: Germinal center B cells (centrocytes + centroblasts)
- Key genetic lesion: t(14;18) translocation → BCL2 overexpression → blocks apoptosis
- Morphology: Nodular (follicular) growth pattern; mixture of small centrocytes (cleaved nuclei) and larger centroblasts
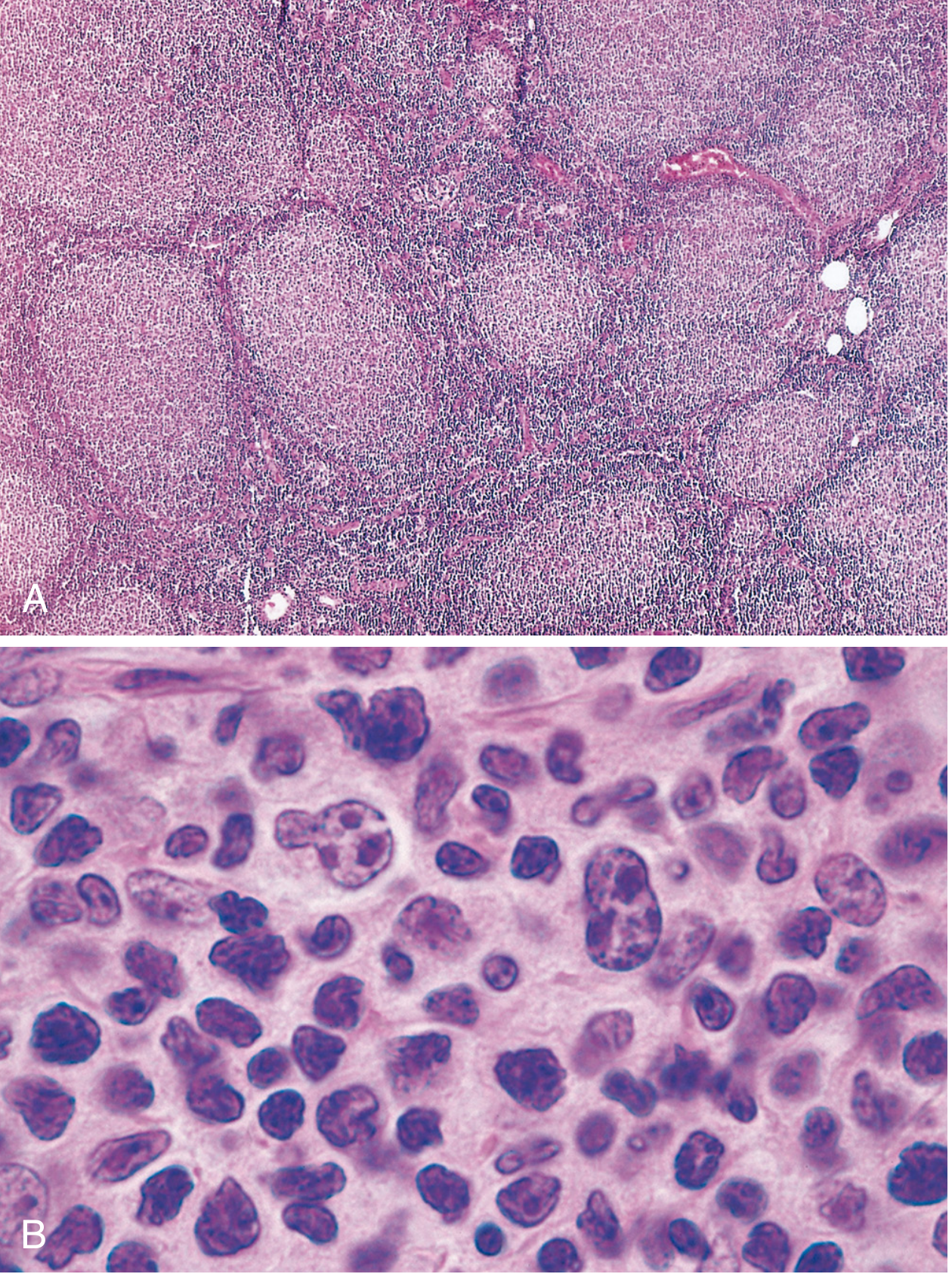
Fig. A - Low power: nodular aggregates throughout the lymph node. Fig. B - High power: small centrocytes with cleaved nuclei mixed with larger centroblasts with nucleoli.
- Immunophenotype: CD20+, BCL2+ (unlike reactive germinal centers), CD10+
- BCL2 immunostain: positive in neoplastic follicles (negative in reactive germinal centers) - key diagnostic feature
- Clinical behavior: Indolent, waxing and waning; median survival 7-9 years; NOT improved by aggressive therapy - palliated with anti-CD20 (rituximab) + gentle chemotherapy
- Histologic transformation: 30-50% transform to DLBCL; if MYC is acquired, prognosis is particularly poor (median survival 3-5 years)
- EZH2 inhibitors are active in the subset with EZH2 gain-of-function mutations
2. Diffuse Large B-Cell Lymphoma (DLBCL)
- Most common NHL (~30%)
- Aggressive but potentially curable
- Includes several distinct subtypes: primary CNS lymphoma, primary mediastinal (thymic) large B-cell lymphoma, leg-type cutaneous DLBCL, plasmablastic lymphoma, double/triple-hit lymphomas
- Double-hit lymphoma: MYC rearrangement + BCL2 and/or BCL6 rearrangements - now classified as "high-grade B-cell lymphoma with MYC and BCL2/BCL6 rearrangements"; requires aggressive regimens (DA-R-EPOCH)
- Primary CNS lymphoma: very sensitive to corticosteroids; treated with high-dose methotrexate ± rituximab; whole-brain RT adds toxicity without benefit
- Plasmablastic lymphoma: Most common in HIV+ patients; CD20 negative, so does NOT benefit from rituximab
3. Mantle Cell Lymphoma
- Cell of origin: Naive B cells in the mantle zone
- Moderately aggressive course
- Key genetic lesion: t(11;14) → cyclin D1 overexpression → confirmed by FISH; CD5+
- Distinct from CLL/SLL by cyclin D1
4. Marginal Zone Lymphoma / MALT Lymphoma
- Indolent tumors of antigen-primed B cells at sites of chronic immune stimulation
- Gastric MALT lymphoma: driven by H. pylori; eradication of H. pylori can induce regression
- Often remain localized for long periods
5. Burkitt Lymphoma
- t(8;14) - MYC translocation (or variants t(2;8) or t(8;22))
- Endemic form: African children, jaw tumors, nearly all EBV+
- Sporadic form: abdominal/ileocecal mass, ~15-35% EBV+
- AIDS-associated form: aggressive, often involves CNS
- "Starry sky" pattern on histology (macrophages phagocytosing apoptotic cells)
6. Small Lymphocytic Lymphoma (SLL) / CLL
- Tissue manifestation of CLL; indolent
- CD5+, CD23+, weak surface Ig
7. Lymphoplasmacytic Lymphoma (Waldenström's Macroglobulinemia)
- B-cell neoplasm with terminal differentiation to plasma cells
- Secretes monoclonal IgM → hyperviscosity syndrome
- Nearly all cases have MYD88 mutations
- No bone destruction (unlike myeloma)
B. T- and NK-Cell NHLs
Represent 5-10% of NHLs in the US/Europe; more common in East Asia.
- Peripheral T-cell lymphoma, NOS: Pleomorphic mixture of malignant T cells; reactive eosinophils and macrophages (cytokine-driven); express CD2, CD3, CD5; significantly worse prognosis than DLBCL
- Anaplastic Large Cell Lymphoma (ALCL): CD30+; ALK+ form has better prognosis; ALK- form has poor prognosis; distinct from Hodgkin lymphoma (CD15-negative)
- Adult T-cell leukemia/lymphoma: caused by HTLV-1; skin lesions, hypercalcemia, leukemia picture
- Mycosis fungoides / Sézary syndrome: Primary cutaneous T-cell lymphoma; starts as skin patches → plaques → tumors (Sézary syndrome = erythroderma + circulating atypical cells)
- Extranodal NK/T-cell lymphoma (nasal type): EBV-associated; midline destructive lesions of the nasopharynx; more common in Asia and Latin America
- Enteropathy-associated T-cell lymphoma: associated with celiac disease; intestinal involvement
C. Lymphoblastic Lymphoma / ALL
- Precursor B or T lymphoblasts
- T-cell LBL: mediastinal mass in young males; CNS involvement common
- B-cell LBL: solid tumors of skin and bones (~85% of ALL has B-cell phenotype)
- Treated with ALL-type regimens (cytarabine, high-dose methotrexate, maintenance therapy, CNS prophylaxis)
IV. HODGKIN LYMPHOMA (HL)
What Makes HL Distinct
- Reed-Sternberg (RS) cells - the neoplastic element
- Robust but ineffective host immune response; RS cells are only a small fraction of the tumor mass
- Arises in a single node/chain and spreads in stepwise contiguous fashion - important for radiotherapy planning
- Robbins Basic Pathology, p. 417
Reed-Sternberg Cells
- Large cells (~45 µm diameter) with bilobed or multilobed nuclei, each with a large "owl-eye" nucleolus (~5-7 µm, size of a small lymphocyte)
- Diagnostic RS cells must have at least two nuclear lobes/nuclei each with a nucleolus
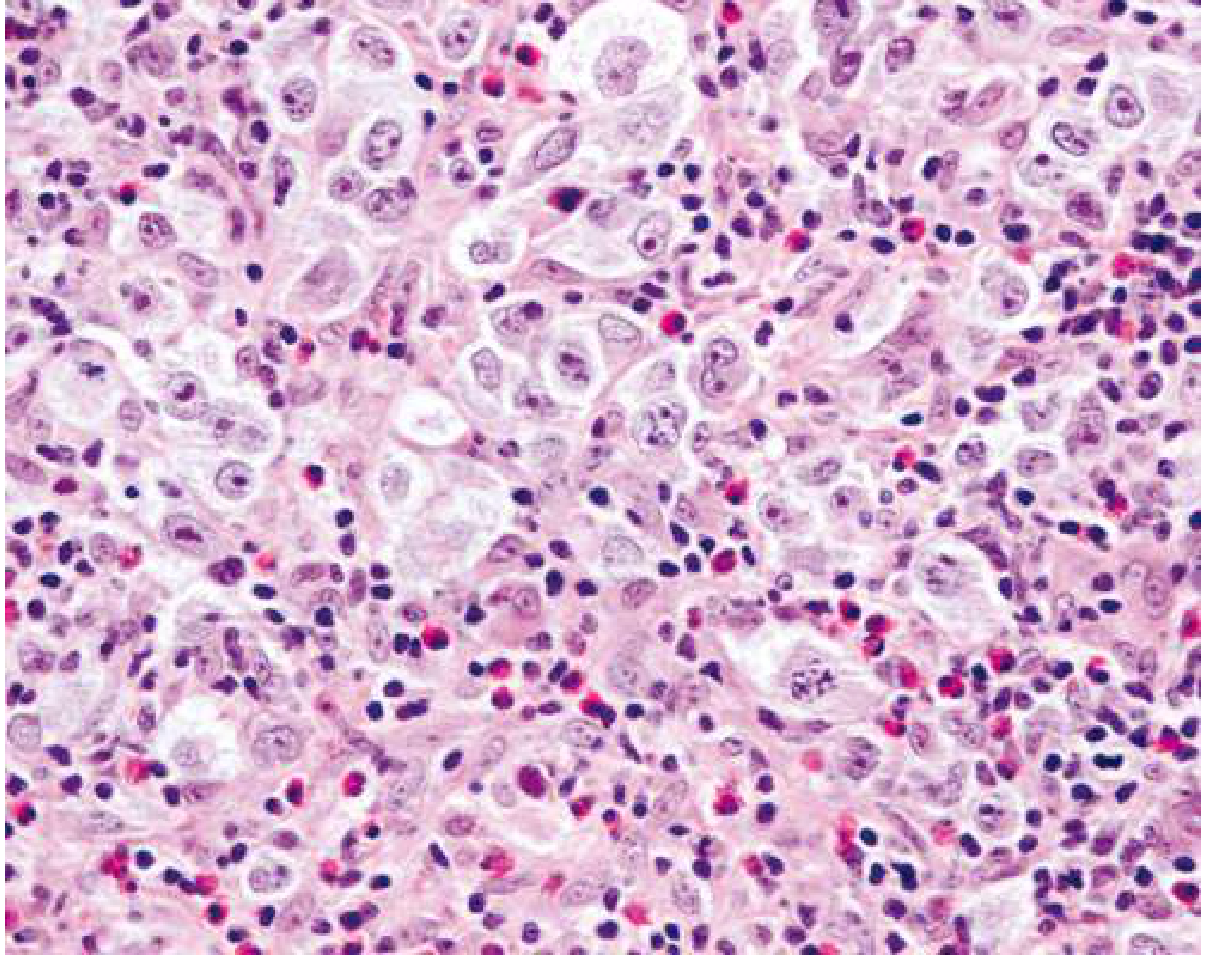
Nodular sclerosing Hodgkin lymphoma: large lacunar cells (RS variants) with abundant pale cytoplasm in a background of lymphocytes and eosinophils. Note the prominent large "owl-eye" nucleoli characteristic of Reed-Sternberg cells.
Pathogenesis of HL
- RS cells originate from germinal center B cells (proven by clonal IGH rearrangements + somatic hypermutation in microdissected RS cells)
- Classic HL RS cells paradoxically fail to express immunoglobulin genes - due to widespread epigenetic reprogramming
- NF-κB activation is the central molecular event:
- EBV LMP-1 (in ~70% of mixed-cellularity subtype) activates NF-κB
- EBV- tumors: loss-of-function mutations in IκB or TNFAIP3
- Immune evasion: RS cells express high levels of PD-L1 and PD-L2 (chromosome 9p amplification) → antagonizes cytotoxic T-cell responses
- Reactive background: RS cells secrete IL-5 (eosinophil chemoattractant), TGF-β (fibrogenic), IL-13 (autocrine growth)
WHO Classification of HL Subtypes
| Subtype | Frequency |
|---|---|
| Nodular sclerosis | 60% (most common) |
| Lymphocyte-rich | 3% |
| Mixed cellularity | 9% |
| Lymphocyte-depleted | 1% (worst prognosis) |
| Nodular Lymphocyte-Predominant HL (NLPHL) | 8% |
Data: Goldman-Cecil Medicine, Table 172-1
Key HL Subtypes
Nodular Sclerosis (most common):
- Young adults; mediastinal involvement common
- Collagen bands divide lymph node into nodules
- Lacunar cells (RS variants with retracted cytoplasm due to formalin fixation)
- Background: lymphocytes, eosinophils, plasma cells, neutrophils
Mixed Cellularity:
- Older adults; EBV present in ~70%
- Diagnostic RS cells easily found
- Background: lymphocytes, eosinophils, plasma cells, histiocytes
Lymphocyte-Depleted:
- Rarest; most aggressive; older/HIV patients
- Few lymphocytes; sheets of RS cells
Nodular Lymphocyte-Predominant HL (NLPHL):
- Distinct entity; neoplastic cells are "popcorn cells" (LP cells/lymphocytic and histiocytic cells)
- CD20+, CD79a+, CD45+ (unlike classic HL)
- CD30-, CD15- (unlike classic HL)
- More indolent course; associated with late relapse
Immunophenotype of Classic HL RS Cells
| Marker | Classic HL | NLPHL | Reactive/ALCL |
|---|---|---|---|
| CD30 | + (90-100%) | - | + (ALCL) |
| CD15 | + (75-85%) | - | - |
| CD20 | +/- (~40%, weak) | strongly + | - |
| PAX5/BSAP | + (>90%) | + | - |
| CD45 | - | + | - |
V. STAGING - ANN ARBOR SYSTEM (Modified Cotswolds)
| Stage | Definition |
|---|---|
| I | Single lymph node region OR one extralymphatic site (Ie) |
| II | Two or more nodal regions, same side of diaphragm (IIe = + local extralymphatic extension) |
| III | Nodal regions on both sides of diaphragm (IIIe = + local extralymphatic) |
| IV | Diffuse extranodal involvement (bone marrow, lung, bone, liver) |
| A | No B symptoms |
| B | ≥1 of: weight loss >10% in 6 months, unexplained fever >38°C, night sweats |
- Goldman-Cecil Medicine, Table 172-3
VI. WORKUP & STAGING INVESTIGATIONS
- Biopsy: Excisional lymph node biopsy (gold standard); fine needle aspiration is inadequate
- Laboratory: CBC, chemistry including LDH, uric acid
- Imaging: CT chest/abdomen/pelvis; FDG-PET/CT is now mandatory for HL and most aggressive NHLs - more sensitive than CT for staging and residual disease assessment; PET can replace bone marrow biopsy in HL
- Bone marrow biopsy: In NHL if results will change management (not needed if PET positive)
- Lumbar puncture: If CNS involvement suspected (DLBCL with high IPI, Burkitt, etc.)
VII. INTERNATIONAL PROGNOSTIC INDEX (IPI) - for aggressive NHLs
5 adverse factors (1 point each):
- Age > 60 years
- Elevated LDH
- Performance status 2-4
- More than 1 extranodal site
- Ann Arbor stage III or IV
| Score | Risk Group |
|---|---|
| 0-1 | Low |
| 2 | Low-intermediate |
| 3 | High-intermediate |
| 4-5 | High |
- Goldman-Cecil Medicine, Table 171-8
VIII. TREATMENT OVERVIEW
Hodgkin Lymphoma
- Limited stage (I-II, favorable): 2-4 cycles ABVD + involved-site radiotherapy
- Advanced stage (III-IV): 6-8 cycles ABVD or escalated BEACOPP
- BEACOPP: superior response rates but more toxicity (infertility with alkylating agents; not seen with ABVD)
- Brentuximab vedotin (anti-CD30 ADC): used in refractory/relapsed HL and upfront with AVD in stage III-IV
- PD-1 checkpoint inhibitors (nivolumab, pembrolizumab): active in relapsed/refractory HL (exploiting PD-L1 overexpression on RS cells)
- Relapsed/refractory HL: Second-line chemo → autologous hematopoietic stem cell transplant (HSCT) for chemosensitive disease
Non-Hodgkin Lymphoma - Key Treatments
| NHL Type | First-line Treatment |
|---|---|
| DLBCL | R-CHOP (rituximab + cyclophosphamide, doxorubicin, vincristine, prednisone) |
| Double/triple-hit | DA-R-EPOCH |
| Follicular (symptomatic) | R-CHOP, R-bendamustine + maintenance rituximab; EZH2 inhibitors (tazemetostat) for EZH2-mutant |
| Mantle cell | Rituximab-based + BTK inhibitors (ibrutinib, acalabrutinib); autologous HSCT in young fit patients |
| Burkitt | Intensive ALL-like regimens (CODOX-M/IVAC); CNS prophylaxis essential |
| MALT/Gastric | H. pylori eradication; radiotherapy for localized; rituximab |
| Primary CNS lymphoma | High-dose methotrexate ± rituximab ± cytarabine; avoid whole-brain RT as initial therapy |
| T-cell lymphomas | CHOP-based; worse prognosis than comparable B-cell lymphomas |
| Lymphoblastic lymphoma | ALL-type regimens with CNS prophylaxis |
Special Situations
- AIDS-associated NHL: Treat same as non-immunocompromised; add CNS prophylaxis; prognosis has improved with HAART
- Post-transplant lymphoproliferative disorder (PTLD): Reduce immunosuppression first; rituximab; chemotherapy for refractory cases
- Elderly patients: Dose-adjusted regimens; careful assessment of cardiac function for anthracyclines
IX. KEY GENETIC LESIONS SUMMARY
| Lymphoma | Translocation/Mutation | Effect |
|---|---|---|
| Follicular lymphoma | t(14;18) | BCL2 overexpression → blocked apoptosis |
| Mantle cell lymphoma | t(11;14) | Cyclin D1 overexpression → uncontrolled cell cycle |
| Burkitt lymphoma | t(8;14) [or t(2;8), t(8;22)] | MYC overexpression → uncontrolled proliferation |
| DLBCL - double hit | MYC + BCL2/BCL6 rearrangements | Highly aggressive |
| Classic Hodgkin HL | 9p amplification (PD-L1/L2); NF-κB activation | Immune evasion; survival signaling |
| NLPHL | - | Germinal center B-cell origin; CD20+ |
| Lymphoplasmacytic lymphoma | MYD88 mutation | NF-κB activation |
| Hairy cell leukemia | BRAF V600E mutation | Constitutive MAPK signaling |
| ALCL | ALK translocation (subset) | ALK+ has better prognosis |
X. CLINICAL PEARLS
- Lymphoma spreads stepwise and contiguously in HL but skips nodes more often in NHL
- "B symptoms" (fever >38°C, night sweats, >10% weight loss) are adverse prognostic signs and affect staging (A vs. B designation)
- RS cells in classic HL: CD15+, CD30+ - the hallmark immunoprofile
- RS-like cells can appear in infectious mononucleosis, solid tumors, and some NHLs - diagnosis requires clinicopathologic correlation
- Follicular lymphoma is incurable with standard therapy but follows an indolent course; transformation to DLBCL occurs in 30-50%
- Gastric MALT lymphoma often regresses with H. pylori eradication alone
- High macrophage infiltrate in HL is a predictor of treatment resistance
- PET/CT has replaced gallium scanning and is now the gold standard for staging and response assessment in HL and aggressive NHLs
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine International Edition (2-volume set)
This is a shared conversation. Sign in to Orris to start your own chat.