Congenital dysplasia of hip
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
developmental dysplasia hip DDH
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have enough comprehensive information to write a thorough answer. Let me compile everything.
Congenital / Developmental Dysplasia of the Hip (CDH / DDH)
Definition and Spectrum
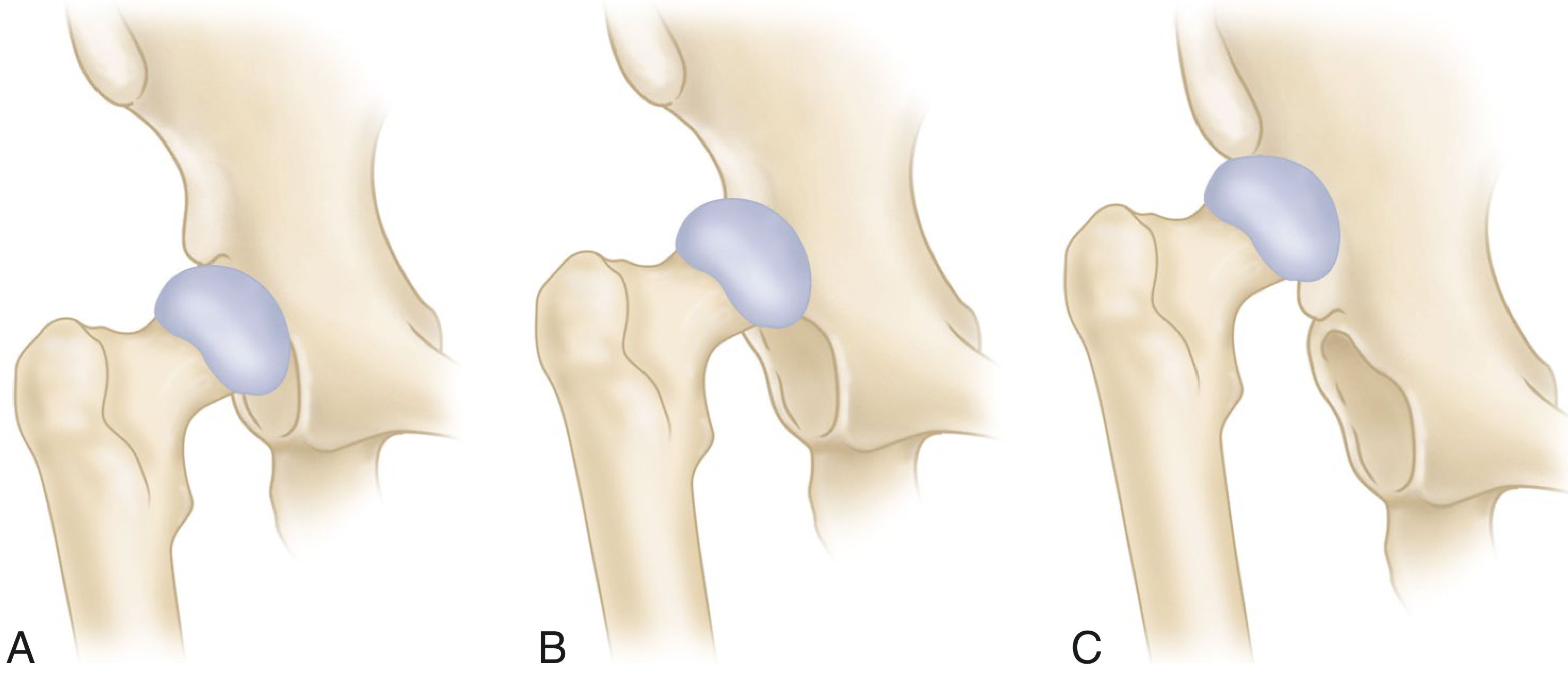
DDH is an umbrella term covering a spectrum of hip abnormalities ranging from mild acetabular dysplasia to frank dislocation. The key distinction is:
- Dysplasia - morphologic change in acetabulum or proximal femur without loss of contact
- Subluxation - articular surfaces in contact but not concentrically aligned
- Dislocation - articular surfaces of acetabulum and proximal femur have no contact at all
The spectrum can be visualized as follows:
Epidemiology and Risk Factors
- Clinical hip instability occurs in 1-2% of term infants; up to 15% have imaging findings
- Risk factors (additive):
- Breech presentation (most important)
- Female gender
- Positive family history (most important alongside breech)
- Incorrect lower extremity swaddling (forced hip extension/adduction)
- First-born child, oligohydramnios
A 2025 meta-analysis (Tirta et al., JAMA Netw Open, PMID 39853978) confirmed these risk factors before 3 months of age.
Pathoanatomy
In DDH, multiple structures are deformed:
| Structure | Deformity |
|---|---|
| Femoral head | Small, deformed |
| Femoral neck | Narrow, short, increased anteversion |
| Greater trochanter | Small, often posteriorly positioned |
| Femoral canal | Narrow (avg ~1.5 cm at 2 cm below lesser trochanter) |
| Acetabulum | Shallow, oblique roof; "false acetabulum" forms where head impinges on ilium |
| Abductors | Poorly developed, oriented more transversely |
| Adductors/psoas | Shortened and contracted |
| Sciatic nerve | Never assumed normal length; susceptible to stretch injury at correction |
Clinical Features and Diagnosis
Signs may be present at birth or develop during early infancy. Instability is the primary neonatal sign; by 3 months, instability diminishes as muscle tone increases, leaving abduction asymmetry as the main sign.
Screening Tests
< 3 months of age:
- Barlow test: Hip in 90° flexion + adduction; posterior lateral pressure applied. A clunk = femoral head dislocating out the back of the acetabulum.
- Note: AAP (2016) recommends no posterior-directed force - the test has no proven predictive value for future dislocation and can itself cause instability if performed forcefully.
- Ortolani test: From similar starting position, hip is abducted with gentle anterior pressure on the greater trochanter. A clunk = femoral head reducing into the socket.
- "Hip clicks" (soft tissue snapping) are benign and must be distinguished from the pathological "hip clunk"
After 3 months (Barlow/Ortolani sensitivity diminishes):
- Limited abduction - the most reliable sign
- Galeazzi sign - apparent limb length discrepancy due to proximal femoral migration (see image below)
- Asymmetric thigh/gluteal skin folds
- Trendelenburg gait or limp in older, walking children

Imaging
| Age | Preferred Modality | Notes |
|---|---|---|
| < 4-6 weeks | Not routinely indicated; ultrasound if high-risk | 96% of ultrasound-detected abnormalities resolve in first 6 weeks |
| 4 weeks - 6 months | Ultrasound (Graf method) | Ossific nucleus not yet visible on x-ray |
| > 4-6 months | AP radiograph of pelvis | Ossific nucleus appears; lines (Hilgenreiner, Perkin's, Shenton's) become useful |
AP pelvis x-ray lines:
- Hilgenreiner's line - horizontal line through triradiate cartilages
- Perkin's line - vertical line through lateral edge of acetabulum
- Femoral head ossification center should be in the inferomedial quadrant
- Shenton's line - smooth arc along inferior femoral neck to superior obturator foramen; disrupted in dislocation
- Acetabular index - normally <30° at birth, <20° by 2 years
Crowe Classification (for surgical planning in adults/late DDH)
Based on degree of proximal femoral migration relative to the acetabulum:
| Type | Subluxation |
|---|---|
| I | < 50% |
| II | 50-75% |
| III | 75-100% |
| IV | > 100% (complete dislocation) |
Estimated as: vertical distance (medial head-neck junction to interteardrop line) / vertical diameter of opposite femoral head × 100%.
Treatment - Age-Based Algorithm
Newborn - 6 months: Pavlik Harness (First-Line)
- Holds hips in flexion and abduction, allowing gradual reduction and acetabular remodeling
- Success rate ~85% when initiated before 6 months
- Used for: dislocated, located but unstable, or dysplastic hips
- An isolated positive Barlow test up to 2 weeks will often stabilize spontaneously - can monitor for 4-6 additional weeks
- Because 96% of pathologic ultrasound findings resolve within first 6 weeks, treatment can be safely delayed to that time if the hip is stable
6 - 18 months: Closed/Open Reduction + Spica Cast
- If Pavlik fails or child is older than 6-8 months: closed reduction under anesthesia followed by spica cast immobilization
- Arthrogram performed at time of reduction to confirm concentric position
- Open reduction may be needed if closed reduction fails
> 18 months: Open Reduction ± Osteotomies
- Most children beyond 18 months require open reduction
- Combined with:
- Innominate (Salter) osteotomy - redirects acetabulum anterolaterally (most common for ages 18 months - 6 years)
- Pemberton osteotomy - acetabuloplasty for residual dysplasia
- Femoral osteotomy - derotation/shortening as needed to reduce tension on vessels
- Triple innominate osteotomy - for older children/young adults with open triradiate cartilage
- Periacetabular osteotomy (Ganz PAO) - preferred for skeletally mature patients with retained cartilage space
Adult / Late Presentation: Total Hip Arthroplasty (THA)
For symptomatic arthritis secondary to dysplasia:
- Acetabular component placed at true acetabulum (not false acetabulum)
- Very small cup may be needed (≤40 mm)
- Limb lengthening limited to 3-4 cm maximum (sciatic nerve risk)
- Femoral osteotomy often needed to correct anteversion, angular deformity, narrow canal
- Abductor muscles are poorly developed and may require extensive release
Complications
- Avascular necrosis (AVN) of femoral head - most feared complication; can occur from reduction (especially forceful) or from the untreated dislocation itself
- Residual acetabular dysplasia - may persist after successful reduction, requiring secondary procedures
- Re-dislocation - after closed/open reduction
- Sciatic nerve palsy - with aggressive lengthening or reduction of high dislocations
- Trendelenburg gait - from abductor weakness or coxa vara
- Early osteoarthritis - the inevitable endpoint of untreated or inadequately treated DDH
Long-term Consequences if Untreated
- Progressive osteoarthritis
- Chronic back pain (from compensatory lumbar scoliosis)
- Aseptic necrosis of femoral head
- Significant limb length discrepancy and gait abnormality
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter: Congenital and Developmental Dysplasia of the Hip
- Rosen's Emergency Medicine - Concepts and Clinical Practice, Chapter 170: Pediatric Hip Disorders
- Harriet Lane Handbook 23rd Ed, Chapter 26: Hip Disorders
- Recent evidence: Tirta et al. (2025) Meta-Analysis on DDH risk factors, PMID 39853978 | Shanaa et al. (2025) Hip Resurfacing in DDH, PMID 40680148
This is a shared conversation. Sign in to Orris to start your own chat.