Cold abscess
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cold abscess" tuberculosis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full synthesis:
Cold Abscess
Definition
A cold abscess is a collection of pus that develops slowly, lacks the classical signs of acute inflammation — redness (rubor), warmth (calor), and tenderness (dolor) — due to the low-grade, granulomatous nature of the underlying infection. The term "cold" reflects the absence of heat and the insidious clinical course, in contrast to a "hot" pyogenic abscess.
Pathogenesis
The paradigmatic cause is tuberculosis (TB), where Mycobacterium tuberculosis induces a granulomatous immune response. Instead of rapid neutrophilic destruction (as in pyogenic infections), TB provokes:
- Macrophage-dominated granuloma formation
- Central caseous (cheese-like) necrosis — liquefaction of the caseous material produces pus
- Accumulation in a well-defined, smooth-walled cavity with minimal surrounding inflammatory reaction
Because the host response is chronic and T-cell mediated rather than neutrophilic, there is little prostaglandin-driven heat, erythema, or acute pain — hence the abscess is "cold."
Common Sites & Clinical Presentations
1. Scrofuloderma (Cutaneous TB)
Subcutaneous tuberculosis leads to cold abscess formation and secondary breakdown of overlying skin. It represents contiguous involvement of skin overlying another infected site — most commonly tuberculous lymphadenitis, TB of bones/joints, or tuberculous epididymitis.
- Most often in parotideal, submandibular, and supraclavicular regions (can be bilateral)
- Begins as a firm, well-defined, freely movable, asymptomatic subcutaneous nodule
- Gradually softens → liquefaction and perforation → ulcers and sinuses with linear or serpiginous undermined edges and bluish-purple skin
- Sinusoidal tracts undermine the skin; scar tracts bridge ulcerated areas

2. Mycobacterial Lymphadenitis (Scrofula)
Both M. tuberculosis and non-tuberculous mycobacteria (NTM) cause chronic cervical lymphadenitis presenting as a chronic, minimally tender "cold abscess" with overlying violaceous skin. Spontaneous drainage transforms it into a chronic draining sinus. — Tintinalli's Emergency Medicine
3. Spinal TB / Pott's Disease — Psoas Abscess
The most feared cold abscess. TB of the spine begins in the subchondral region of the vertebral body, erodes the intervertebral disc, and pus tracks along fascial planes:
- Along the psoas sheath → presenting as a groin mass (psoas/iliopsoas abscess)
- As paraspinal soft-tissue density on AP radiographs
- Can track far from the original lesion without warmth or acute tenderness
From Gray's Anatomy for Students: "The infected disc material extruded around the disc anteriorly and passed into the psoas muscle sheath… the pus spread within the psoas muscle sheath beneath the inguinal ligament to produce a hard mass in the groin. This is a typical finding for a psoas abscess."
4. Genital TB
In males, tuberculous epididymitis may manifest with a scrotal cold abscess. When it ruptures, it leaves a non-healing post-rupture sinus. — Comprehensive Clinical Nephrology
5. Other Locations
- Osteoarticular TB — any bone or joint; abscesses have smooth, thin walls
- Peritoneal/intra-abdominal TB — retroperitoneal cold abscesses
- Scrofuloderma from rib TB, sternal TB
Radiology
MRI Features (Tuberculous vs. Pyogenic)
| Feature | Pyogenic Abscess | Cold (Tuberculous) Abscess |
|---|---|---|
| Onset | Acute, severe | Insidious, chronic |
| Surrounding inflammation | Prominent, ill-defined | Minimal, well-defined |
| Abscess wall | Thick, irregular | Smooth, thin |
| Surrounding soft tissue | Widespread oedema | Little surrounding signal change |
| Sites | Usually single | Often multiple |
| Systemic markers | Elevated (high CRP, fever) | Less prominent |
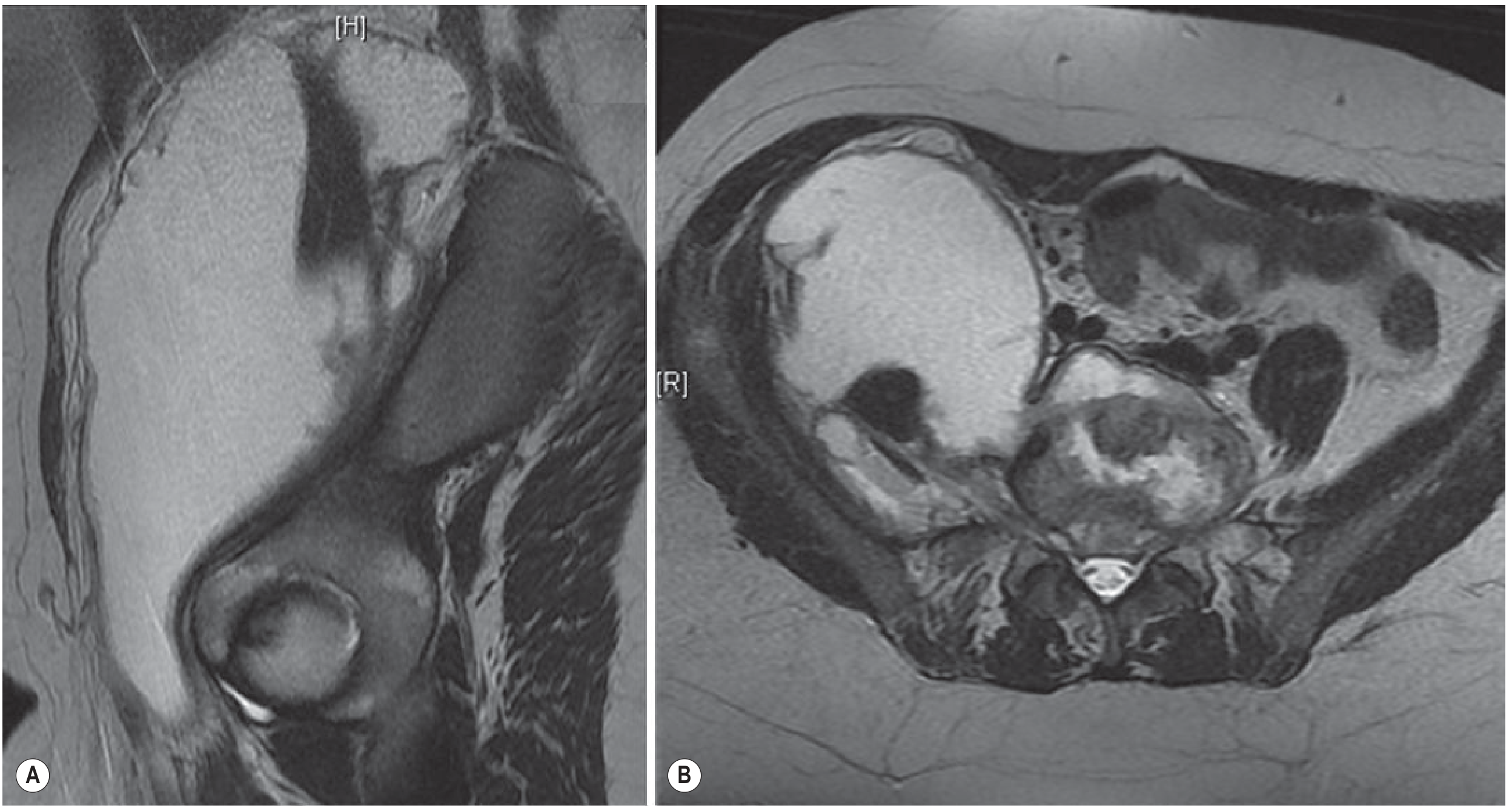
On plain radiographs of the spine, a cold abscess appears as paraspinal soft-tissue density. On CT/PET, foci of calcification within the abscess are characteristic of chronic TB cold abscesses. — Goldman-Cecil Medicine
Histopathology
- Central: massive necrosis and abscess formation (non-specific)
- Periphery / margins of sinuses: tuberculoid granulomas — the diagnostic finding
- Multinucleated Langhans giant cells surrounded by epithelioid macrophages and a rim of lymphocytes
Diagnosis
| Test | Utility |
|---|---|
| Tuberculin skin test (Mantoux) | Strongly reactive in TB cold abscess |
| Differential Mantoux (combined antigens) | Identifies TB vs. NTM in ~93% |
| Culture of aspirate | Gold standard; confirms diagnosis |
| AFB smear/NAAT (PCR) | Rapid identification of M. tuberculosis |
| Chest X-ray | Concurrent pulmonary TB in ~50% |
| MRI | Best for defining extent of soft-tissue abscess and bone involvement |
Treatment
| Cause | Treatment |
|---|---|
| M. tuberculosis | Standard 4-drug anti-TB therapy (HRZE) for 6–12 months |
| Non-tuberculous mycobacteria (NTM) | Surgical excision (lymphadenitis); NTM are more resistant |
| Psoas/large abscess | Radiologically guided percutaneous drainage + anti-TB therapy |
| Scrofuloderma | Anti-TB therapy; surgical debridement if extensive sinus tracts |
Treatment for NTM lymphadenitis is surgical excision; for tuberculous lymphadenitis, treat for 8–12 months with anti-TB drugs. — Tintinalli's Emergency Medicine
Key Distinguishing Features from a Hot (Pyogenic) Abscess
| Cold Abscess (TB) | Hot Abscess (Pyogenic) | |
|---|---|---|
| Pain | Minimal/absent | Severe, throbbing |
| Redness | None or violaceous skin | Erythema |
| Warmth | Absent | Present |
| Fluctuance | Present (late) | Present (early) |
| Systemic signs | Low-grade fever, night sweats, weight loss | High fever, rigors, leukocytosis |
| Pus consistency | Caseous / cheese-like | Creamy, purulent |
| Course | Months | Days |
Sources: Fitzpatrick's Dermatology (Vol. 1-2), Grainger & Allison's Diagnostic Radiology, Tintinalli's Emergency Medicine, Goldman-Cecil Medicine, Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.