PPI
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Proton Pump Inhibitors (PPIs) drawn from Goodman & Gilman's Pharmacological Basis of Therapeutics, Goldman-Cecil Medicine, and Yamada's Textbook of Gastroenterology.
Proton Pump Inhibitors (PPIs)
Overview
PPIs are the most potent suppressors of gastric acid secretion available. They inhibit the gastric H+/K+-ATPase (the proton pump) and reduce daily acid production (basal and stimulated) by 80-95%.
Available Agents and Doses
| Drug | Standard Dose | Maintenance Dose |
|---|---|---|
| Omeprazole | 20-40 mg/day | 20 mg/day |
| Lansoprazole | 15-30 mg/day | 15 mg/day |
| Pantoprazole | 40 mg/day | 40 mg/day |
| Rabeprazole | 20 mg/day | 10-20 mg/day |
| Esomeprazole (S-isomer of omeprazole) | 20-40 mg/day | 20 mg/day |
| Dexlansoprazole (R-enantiomer of lansoprazole) | 30-60 mg/day | 30 mg/day |
All PPIs have equivalent efficacy at comparable doses.
Mechanism of Action
PPIs are prodrugs that require activation in an acid environment. Here is the step-by-step mechanism:
- Oral PPI is absorbed in the small bowel and enters systemic circulation
- It diffuses into gastric parietal cells and concentrates in the acidic secretory canaliculi
- Proton-catalyzed conversion forms a tetracyclic sulfenamide (active form), trapping the drug in the canaliculus
- The activated sulfenamide binds covalently to sulfhydryl groups of cysteines on the H+/K+-ATPase
- This irreversibly inactivates the pump - acid secretion resumes only when new pumps are synthesized (24-48 hours)
Because PPIs block the final common step in acid production, they suppress all stimulated acid (histamine, gastrin, acetylcholine pathways) as well as basal secretion.
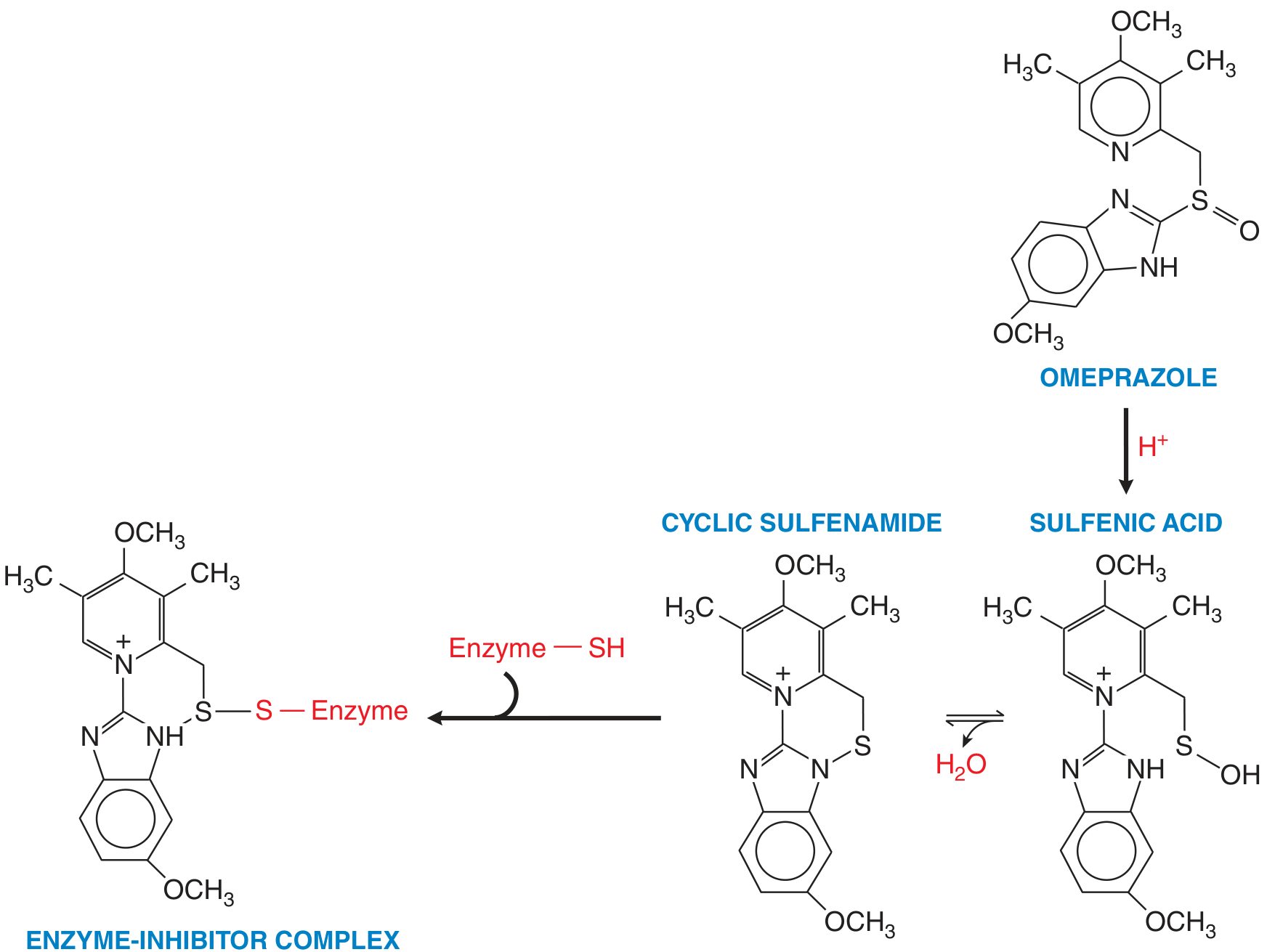
Activation of a PPI (omeprazole) from its prodrug form. The sulfenamide reacts covalently with sulfhydryl groups on the proton pump, irreversibly inhibiting it. - Goodman & Gilman's, Fig. 53-2
Pharmacokinetics (ADME)
- Take 30 min before a meal - food stimulates acid production, which activates the prodrug in the canaliculus
- Rapidly absorbed in the small bowel; highly protein bound
- Extensively metabolized by CYP2C19 and CYP3A4
- Plasma t½ is short (~0.5-3 h), but acid suppression lasts 24-48 h due to irreversible pump binding
- Full effect takes 2-5 days (not all pumps are active simultaneously; once-daily dosing takes time to reach steady-state ~70% inhibition)
- Formulations protect against acid degradation in the stomach:
- Enteric-coated pellets (e.g., rabeprazole)
- Delayed-release tablets (lansoprazole, pantoprazole, rabeprazole)
- Delayed-release capsules (dexlansoprazole, esomeprazole, omeprazole, lansoprazole)
- IV forms available: esomeprazole sodium, omeprazole sodium, pantoprazole
CYP2C19 polymorphisms: Asians (25-30%) and Oceanians (~60%) are more likely to be poor metabolizers of PPIs vs. ~15% of Caucasians or Africans. Poor metabolizers achieve higher plasma levels - may require dose reduction for chronic use.
Clinical Indications
| Indication | Notes |
|---|---|
| GERD / Erosive esophagitis | First-line; superior to H2 blockers |
| Peptic ulcer disease (gastric & duodenal) | Promotes healing |
| H. pylori eradication | Used alongside antibiotics (triple/quadruple therapy) |
| Zollinger-Ellison syndrome | Drug of choice; controls hypersecretion in >95% |
| NSAID-associated ulcers | Prevention and treatment (lansoprazole, pantoprazole, esomeprazole approved) |
| GI bleeding (peptic ulcer) | High-dose IV PPI post-endoscopy reduces rebleeding and need for surgery |
For upper GI bleeding: IV esomeprazole 80 mg bolus then 8 mg/h for ~72 h after endoscopic hemostasis reduces rebleeding from 10.3% to 5.9%.
Drug Interactions
- Clopidogrel: PPIs (especially omeprazole) inhibit CYP2C19 conversion of clopidogrel to its active form. Pantoprazole is least likely to cause this interaction. Concurrent PPI + clopidogrel use significantly reduces GI bleeding without increasing adverse cardiac events.
- Warfarin: Interaction with esomeprazole, lansoprazole, omeprazole, rabeprazole
- Diazepam: Esomeprazole, omeprazole (increased levels)
- Atazanavir/Nelfinavir: Reduced absorption with all PPIs (avoid co-use with HIV antiretrovirals)
- Methotrexate: PPIs inhibit methotrexate elimination → elevated MTX levels (toxicity risk)
- Omeprazole specifically: Inhibits CYP2C19 (raises phenytoin, disulfiram levels) and induces CYP1A2 (increases clearance of theophylline, imipramine, antipsychotics)
Adverse Effects
Common (generally well-tolerated):
- Headache, nausea, abdominal pain, flatulence, constipation, diarrhea
Long-term / serious concerns:
- Hypomagnesemia (chronic use)
- Vitamin B12 deficiency (decreased absorption; clinical relevance not fully established)
- Fracture risk - decreased calcium absorption may reduce bone density
- Hypergastrinemia - secondary to acid suppression; may promote gastric polyposis and atrophic gastritis
- Rebound acid hypersecretion on discontinuation (can cause dyspepsia)
- Clostridium difficile and other GI infections (higher gastric pH reduces barrier)
- Small intestinal bacterial overgrowth (SIBO)
- Possible associations (not yet confirmed by prospective trials): chronic kidney disease, dementia
- COVID-19: Dose-dependent relationship between PPI use and more severe infection/secondary infections
Key Clinical Pearls
- Take 30-60 min before the first meal for optimal activation
- Pantoprazole is preferred when co-prescribing with clopidogrel
- Asian patients may need lower doses chronically due to CYP2C19 polymorphisms
- Don't use alongside atazanavir (reduced HIV drug absorption)
- Discontinuation after prolonged use should be gradual to avoid rebound hypersecretion
- PPI use should be limited to the lowest effective dose and only when clinically indicated
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 53; Goldman-Cecil Medicine, Chapter 124-125; Yamada's Textbook of Gastroenterology
This is a shared conversation. Sign in to Orris to start your own chat.