Anticoagulant for abg analysis
Reading File
Finding Sources
Searching the Web
anticoagulant arterial blood gas ABG analysis heparin lithium
Reading File
Here is a complete summary on anticoagulants for ABG analysis, sourced from Tietz Textbook of Laboratory Medicine (7th Ed.) and Roberts & Hedges' Clinical Procedures in Emergency Medicine.
Anticoagulant for ABG Analysis
Recommended Anticoagulant: Lyophilized Balanced Lithium Heparin (Li-Heparin)
Lithium heparin is the only anticoagulant used for ABG sample collection. The current standard (CLSI C46-A2) specifies:
- Final concentration: 20 IU/mL blood in the collected sample
- Form: Lyophilized (spray-dried/dry) balanced heparin, not liquid
Why Lithium Heparin Specifically?
| Feature | Reason |
|---|---|
| Prevents coagulation | Inhibits thrombin and factor Xa |
| Lithium salt preferred | Does not interfere with electrolyte (Na+, K+) measurements unlike sodium or ammonium heparin |
| Balanced/pre-saturated heparin | Heparin is negatively charged and binds cations (Ca++, Na+, K+) - balanced heparin has binding sites pre-saturated with calcium, preventing electrolyte underestimation |
Why Lyophilized (Dry) Form is Preferred Over Liquid Heparin
Liquid heparin syringes are available but have significant drawbacks:
- Dilution error: Liquid heparin dilutes the sample, causing significant differences in blood gas parameters (pH, pO2, pCO2)
- pH distortion: Heparin pH is ~7.0 (slightly acidic); excess liquid heparin lowers sample pH
- pO2/pCO2 errors: Liquid heparin has pO2 and pCO2 near room air values - excess heparin falsely raises pO2 and lowers pCO2
- Using ordinary syringes flushed with liquid heparin is strongly discouraged per CLSI standards
Dry/lyophilized heparin coats the syringe walls and dissolves only when blood enters, eliminating the dilution problem.
Common Sources of Sample Contamination (to avoid)
- Liquid heparin excess - dilutes sample, alters pH, pO2, pCO2
- Venous blood contamination - falsely lowers pO2/sO2, raises pCO2
- Air bubbles - even 1% of sample volume can significantly raise pO2 and sO2, lower pCO2; effects worsen with time and agitation
Quick Summary
Use lyophilized balanced Li-heparin in dedicated pre-heparinized ABG syringes at a final concentration of 20 IU/mL. Avoid liquid heparin flush techniques and ordinary syringes.
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Anticoagulants & Sample Contamination sections
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - Arterial Puncture chapter
Preferred sites for sample collection
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I now have very detailed source material. Here is the complete answer:
Preferred Sites for ABG Sample Collection
In Adults
The radial, brachial, and femoral arteries are the three sites routinely used for ABG sampling in adults, in order of preference.
1. Radial Artery (Most Preferred)
- Located at the distal wrist, over the volar (palmar) aspect of the radius
- Why preferred:
- Easily palpable and accessible
- Good collateral circulation from the ulnar artery (confirmed by the Modified Allen Test)
- Readily compressible - reduces bleeding risk
- Fewer serious complications compared to other sites
- Needle: 22-gauge, 1.25-inch for adults
- Modified Allen Test must be performed first: occlude both radial and ulnar arteries, have the patient open a fist, then release ulnar artery pressure - the palm should flush pink within seconds, confirming adequate collateral flow. Blood should not be drawn if the test is negative.
- In neonates requiring preductal blood gas values, the right radial artery specifically is used (preductal position relative to the ductus arteriosus)
2. Brachial Artery (Second Choice)
- Located in the antecubital fossa
- Less preferred because:
- It is an end artery in some patients - limited collateral flow
- Deeper and less compressible than radial
- Higher risk of median nerve injury
- Used when radial access is not feasible
3. Femoral Artery (Third Choice / Alternative)
- Located in the femoral triangle, just below the inguinal ligament
- Needle: 20-gauge, 2.5-inch for adults (larger needle due to deeper vessel)
- Drawbacks:
- Hidden by bedcovers - can bleed significantly without being noticed until massive
- Difficult to compress effectively
- Higher infection risk
- Not suitable for ambulatory patients
- Used in emergencies when other sites are inaccessible (e.g., shock, peripheral vascular disease)
In Pediatric Patients
Sites used include: radial, ulnar, femoral, dorsalis pedis, and posterior tibial arteries
- Same gauge range (22-24 gauge), slightly shorter needles than adults
Unacceptable Sites
Avoid sites that are:
- Irritated, edematous, or near a wound
- Over an arteriovenous (AV) shunt or fistula
- Distal to a surgical shunt
- Overlying skin infection, burn, or cutaneous damage
- Areas with absent or diminished collateral flow (e.g., Raynaud's syndrome, abnormal Allen test)
Summary Table
| Site | Preference | Key Advantage | Key Limitation |
|---|---|---|---|
| Radial artery | 1st (most preferred) | Collateral flow (ulnar), compressible | Requires Allen test |
| Brachial artery | 2nd | Accessible at antecubital fossa | End artery, median nerve risk |
| Femoral artery | 3rd (emergency) | Large, palpable in shock | Compressibility poor, hidden bleeding |
| Dorsalis pedis / posterior tibial | Pediatric / alternative | Accessible in infants | Small caliber |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - Site Selection & Arterial Puncture
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Arterial Puncture Technique
- Pfenninger and Fowler's Procedures for Primary Care - Technique
What test to be done before collecting sample
Finding Sources
Reading File
Reading File
Loading Image
Modified Allen Test - Pre-ABG Collection
The Modified Allen Test is the key bedside assessment performed before collecting an ABG sample from the radial artery. It evaluates the adequacy of collateral circulation to the hand via the ulnar artery, ensuring the hand remains perfused even if the radial artery is damaged during puncture.
Why It's Needed
The hand receives blood from both the radial and ulnar arteries, which communicate via the superficial and deep palmar arches. If the radial artery goes into spasm or thromboses post-puncture, the ulnar artery must be able to compensate. The Allen Test checks this collateral reserve.
Step-by-Step Procedure
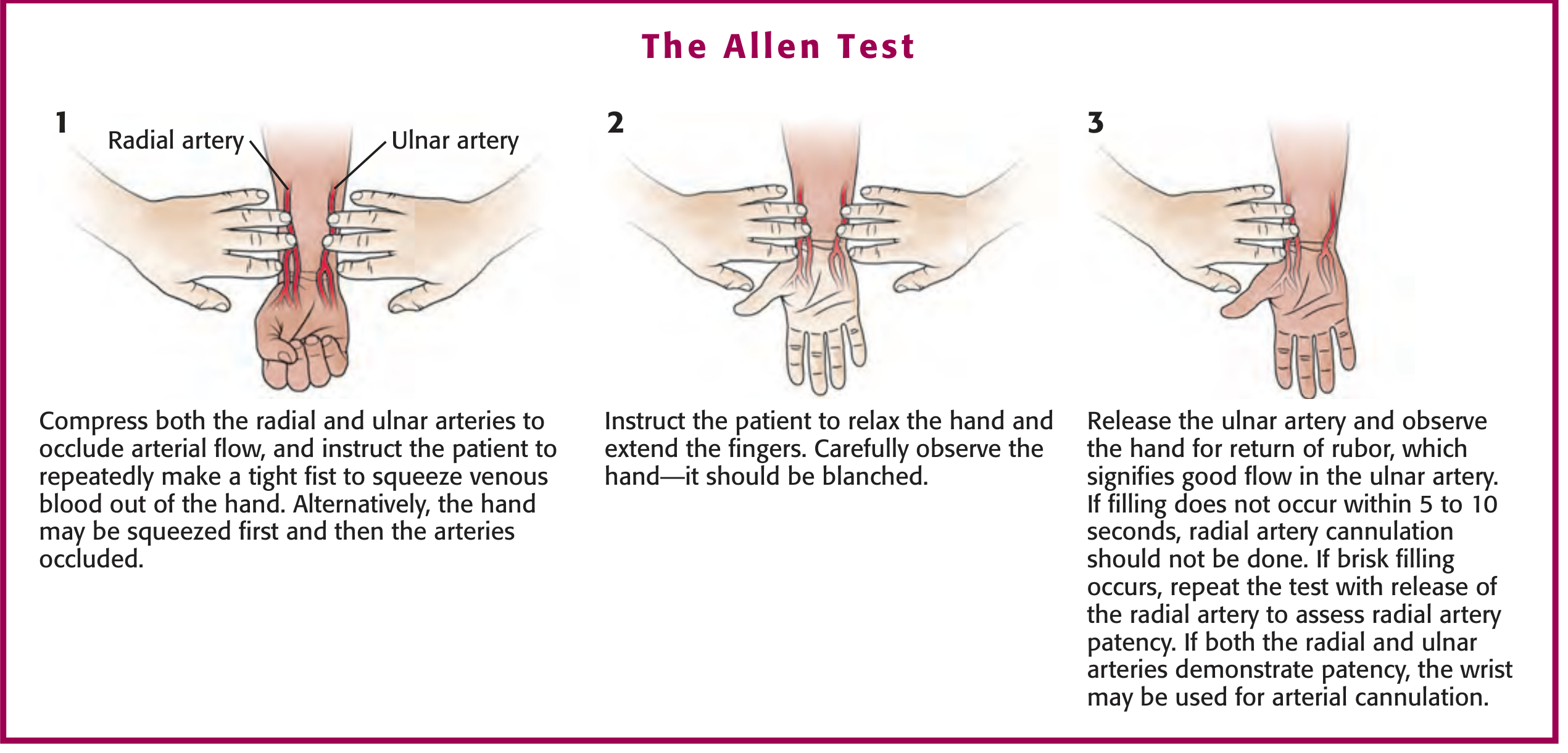
Step 1: Compress both the radial and ulnar arteries simultaneously with your fingers to occlude arterial flow. Ask the patient to repeatedly clench their fist tightly to squeeze blood out of the hand (exsanguinate it).
Step 2: Ask the patient to open and relax the hand. Observe the palm - it should be blanched/pale (confirming occlusion is effective).
Step 3: Release pressure on the ulnar artery only (keep radial compressed). Watch the palm for return of color (rubor/flushing).
Interpretation
| Result | Timing | Interpretation | Action |
|---|---|---|---|
| Normal (Negative test) | Color returns within 5-10 seconds | Adequate ulnar collateral flow | Proceed with radial puncture |
| Abnormal (Positive test) | Pallor persists beyond 5-15 seconds | Inadequate collateral circulation | Do NOT puncture radial artery - choose alternate site |
Important Points
- False positive can occur if the hand is overextended with wide finger separation - this compresses the palmar arches between fascial planes. Avoid this positioning.
- The test is considered mandatory before arterial cannulation (indwelling line), but is not strictly mandatory for a single one-time puncture for blood gas sampling - though it is strongly recommended.
- Even a normal Allen test does not guarantee against ischemic complications after cannulation - cases of ischemia have been reported despite normal results.
- Conversely, some studies show no ischemic complications even with an abnormal Allen test after radial artery catheterization.
- If the test is abnormal, document the finding and select an alternative artery (brachial or femoral).
In Unconscious/Uncooperative Patients
The patient cannot make a fist voluntarily. In this case:
-
The hand can be squeezed manually by the examiner to exsanguinate it before occluding both arteries.
-
Doppler ultrasound or pulse oximetry on the thumb can be used as an objective alternative to assess ulnar perfusion.
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine - Radial and Ulnar Arteries, Allen Test
-
Henry's Clinical Diagnosis and Management by Laboratory Methods - Modified Allen Test, Box 3.4
How will you transport the sample to the lab
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive answer on ABG sample transport, drawn directly from the Tietz Textbook of Laboratory Medicine (7th Ed.) and Pfenninger & Fowler's Procedures for Primary Care.
ABG Sample Transport to the Lab
Immediately After Collection - Pre-Transport Steps
Before transporting, these steps must be done at the bedside:
- Expel all air bubbles - Inspect visually, hold syringe tip up, and eject any air or froth immediately. Even a 100 µL air bubble can raise pO2 by ~4 mmHg and lower pCO2 by ~4 mmHg within just 2 minutes.
- Cap/seal the syringe - Use a rubber stopper or syringe cap to prevent atmospheric air contamination.
- Mix gently - Roll the syringe gently between the palms to mix the heparin and achieve a homogeneous sample. Do NOT shake or mix vigorously - this causes hemolysis.
Storage and Temperature During Transport
| Condition | Effect |
|---|---|
| Room temperature (37°C) | pH drops 0.04-0.08 units/hour; pCO2 rises ~5 mmHg/hour; pO2 changes unpredictably |
| 22°C (room air) | pH drops 0.02-0.03/hour; pCO2 rises ~1 mmHg/hour |
| On ice slurry (1-5°C) | pCO2 rises only ~0.5 mmHg/hour; glycolysis inhibited; changes negligible |
The cause of these changes is ongoing cellular metabolism (leukocytes and erythrocytes continue consuming O2 and producing CO2 after collection).
The Ice Slurry Rule
- Analyze within 15-30 minutes at room temperature - minimal changes occur up to 15 min for pO2/SaO2, and up to 30 min for other analytes (pH, pCO2).
- If analysis will be delayed beyond 30 minutes, immerse the syringe in an ice-water slurry (1-5°C) to inhibit metabolism and preserve values.
- Use ice slurry (crushed ice + water), NOT dry ice or ice cubes directly. Direct contact with ice cubes can cause localized freezing and hemolysis, which falsely lowers pO2 and raises pCO2 and K+.
- Even on ice, samples should be analyzed within 1-2 hours maximum.
Pneumatic Tube Transport - NOT Recommended
Pneumatic tubes create turbulence and agitation during transit. If air bubbles are present in the sample, this dramatically accelerates the exchange of O2 between the blood and any trapped air, causing a disproportionate and unpredictable rise in pO2. Pneumatic tube transport is not recommended for ABG samples.
Hemolysis Prevention During Transport
Hemolysis (which can affect up to 4% of arterial samples) cannot be visually detected in ABG syringes. It falsely lowers pO2 and raises pCO2 and K+. Prevent it by:
- Avoiding vigorous mixing or shaking
- Avoiding pneumatic tubes
- Using ice slurry (not direct ice cubes)
- Avoiding excessive force during aspiration
Summary Checklist
| Step | Action |
|---|---|
| 1 | Expel air bubbles immediately |
| 2 | Cap/seal the syringe |
| 3 | Mix gently (roll between palms) |
| 4 | Label the sample (patient ID, time, FiO2, temperature) |
| 5 | Transport on ice slurry if delay >15-30 min expected |
| 6 | Carry by hand - avoid pneumatic tubes |
| 7 | Analyze within 30 min (room temp) or within 1-2 hr (on ice) |
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Sample Contamination, Hemolysis sections
- Pfenninger & Fowler's Procedures for Primary Care - Technique & Equipment sections
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Arterial Puncture Procedure
This is a shared conversation. Sign in to Orris to start your own chat.