Explain abdomen and pelvis anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, well-sourced content from Gray's Anatomy for Students. Let me compile the comprehensive answer.
Abdomen and Pelvis Anatomy
Primary source: Gray's Anatomy for Students
1. Overview and Surface Boundaries
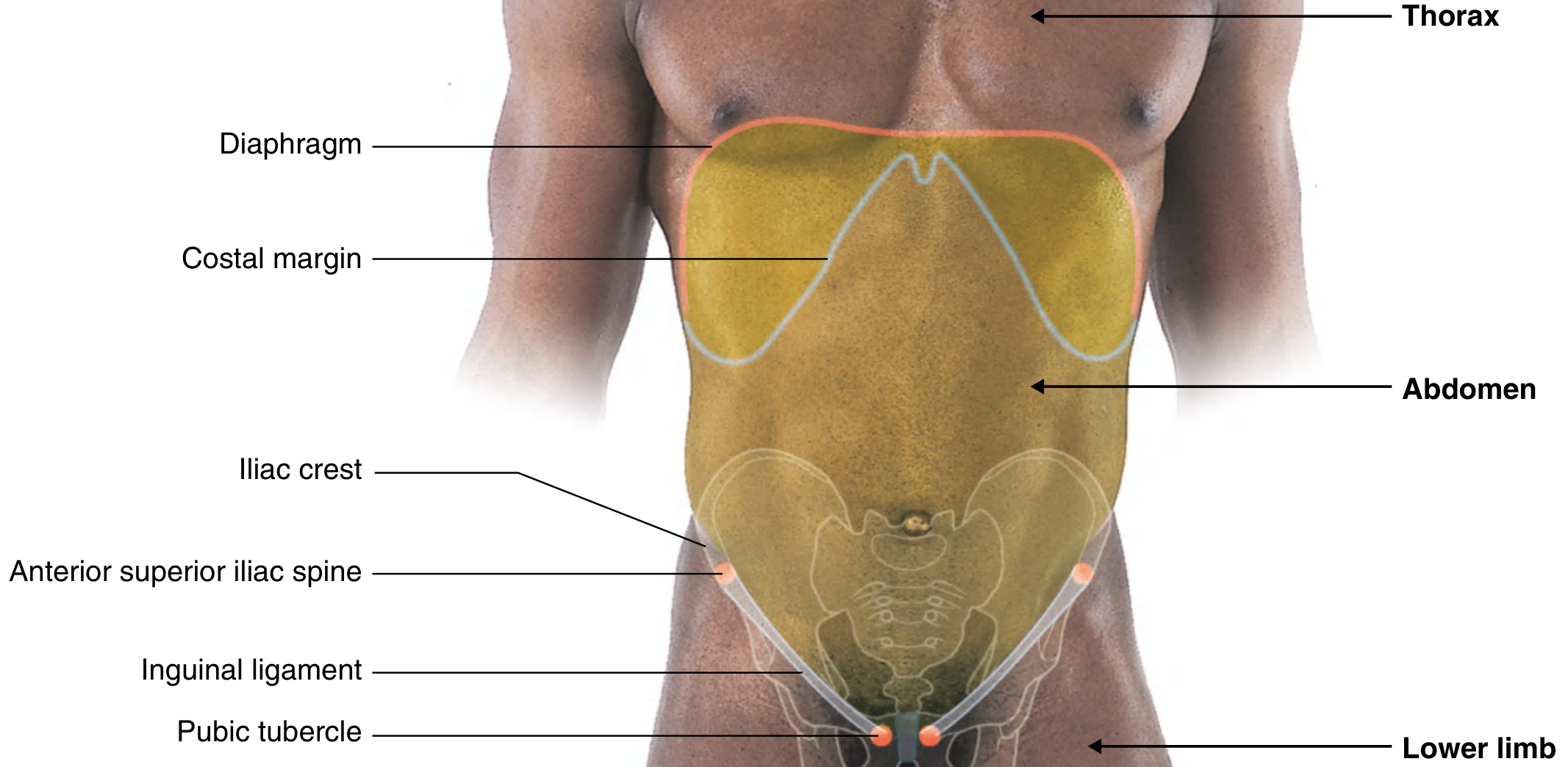
The abdomen is the region of the trunk between the thorax and the pelvis. Its surface extent is defined by palpable bony landmarks:
- Superiorly: xiphoid process and costal margins (the costal margin separates the abdominal wall from the thoracic wall)
- Inferiorly: pubic tubercle, anterior superior iliac spine (ASIS), and iliac crest
- Laterally: the iliac crest separates the posterolateral abdominal wall from the gluteal region
A key clinical point: the upper abdominal cavity projects above the costal margin up to the diaphragm, meaning abdominal viscera there (liver, spleen, stomach) are protected by the lower thoracic cage. The dome of the right diaphragm can reach as high as the 4th costal cartilage during forced expiration.
2. Abdominal Wall Layers
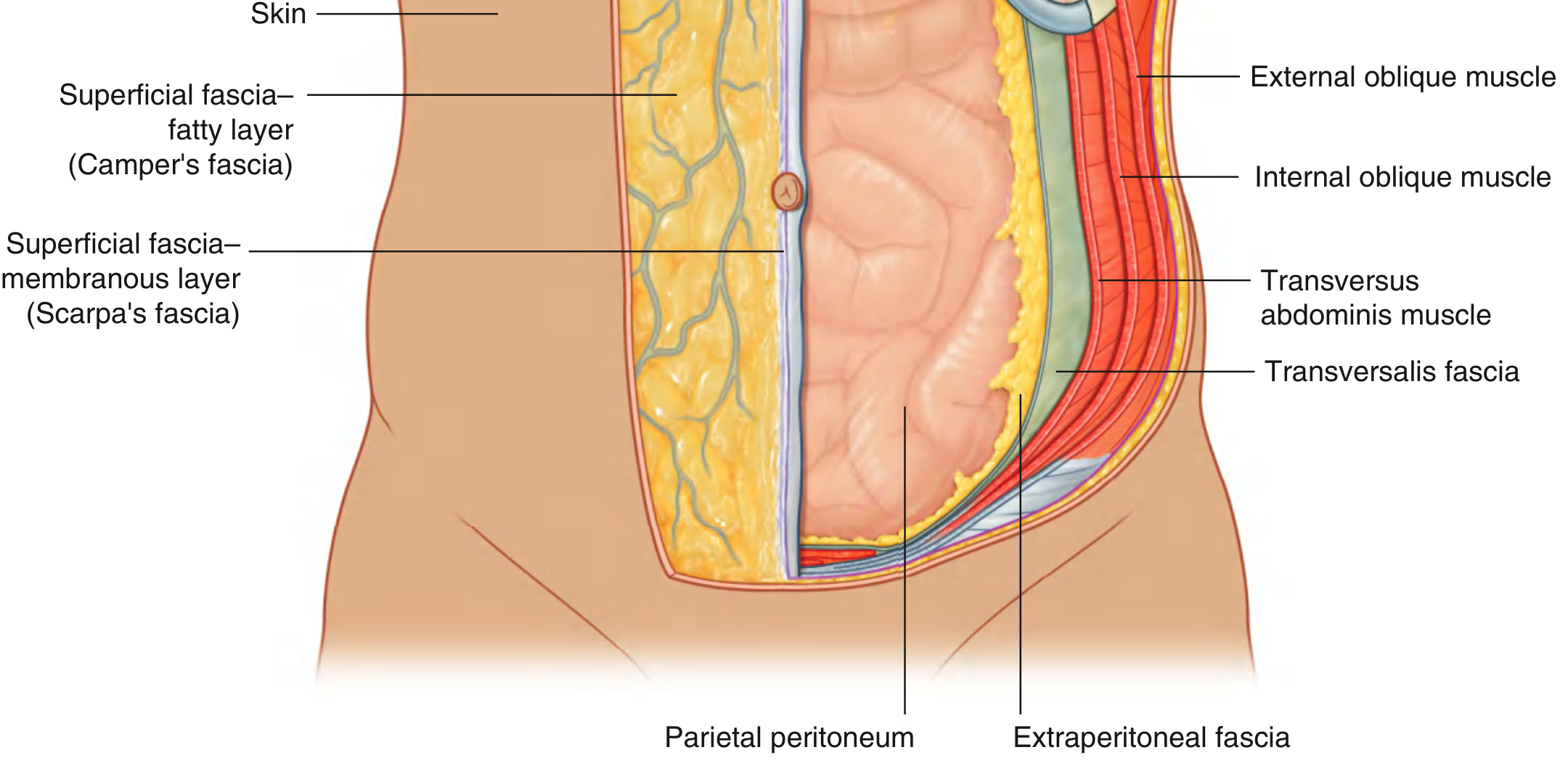
From superficial to deep, the anterior abdominal wall consists of:
- Skin
- Superficial fascia (subcutaneous tissue)
- Muscles and their deep fascias
- Transversalis fascia (extraperitoneal fascia)
- Parietal peritoneum
Superficial Fascia
Below the umbilicus, the superficial fascia splits into two distinct layers:
- Camper's fascia (superficial fatty layer): contains fat, varies in thickness; continuous over the inguinal ligament with the superficial fascia of the thigh. In men, it continues into the scrotum forming dartos fascia. In women, it contributes to the labia majora.
- Scarpa's fascia (deep membranous layer): thin, membranous, little or no fat; fuses with fascia lata of the thigh just below the inguinal ligament; continues into the perineum as Colles' fascia (superficial perineal fascia).
Muscles of the Anterolateral Wall
There are two groups:
Flat muscles (3 layers):
| Muscle | Orientation | Action |
|---|---|---|
| External oblique | Fibers run inferomedially | Compression, rotation |
| Internal oblique | Fibers run superomedially | Compression, rotation |
| Transversus abdominis | Horizontal fibers | Compresses abdomen |
Vertical muscles (2):
- Rectus abdominis: long, flat, paired muscle extending the full length of the anterior wall; separated by the linea alba; enclosed in the rectus sheath
- Pyramidalis: small, triangular; lies in the rectus sheath inferior to rectus abdominis; tenses the linea alba
Transversalis Fascia
The deepest layer of deep fascia, lining the entire abdominal cavity. It is continuous with the fascia on the inferior surface of the diaphragm, and inferiorly it blends with fascia over the pelvic muscles to become the parietal pelvic (endopelvic) fascia.
Innervation of the Abdominal Wall
The skin, muscles, and parietal peritoneum of the anterolateral wall are innervated by T7-T12 and L1 spinal nerves:
- T7-T9: supply skin above the umbilicus
- T10: supplies the umbilical region
- T11, T12, L1: supply skin from just below the umbilicus to the pubic region
- The ilio-inguinal nerve (L1) also supplies the anterior scrotum or labia majora
Blood Supply
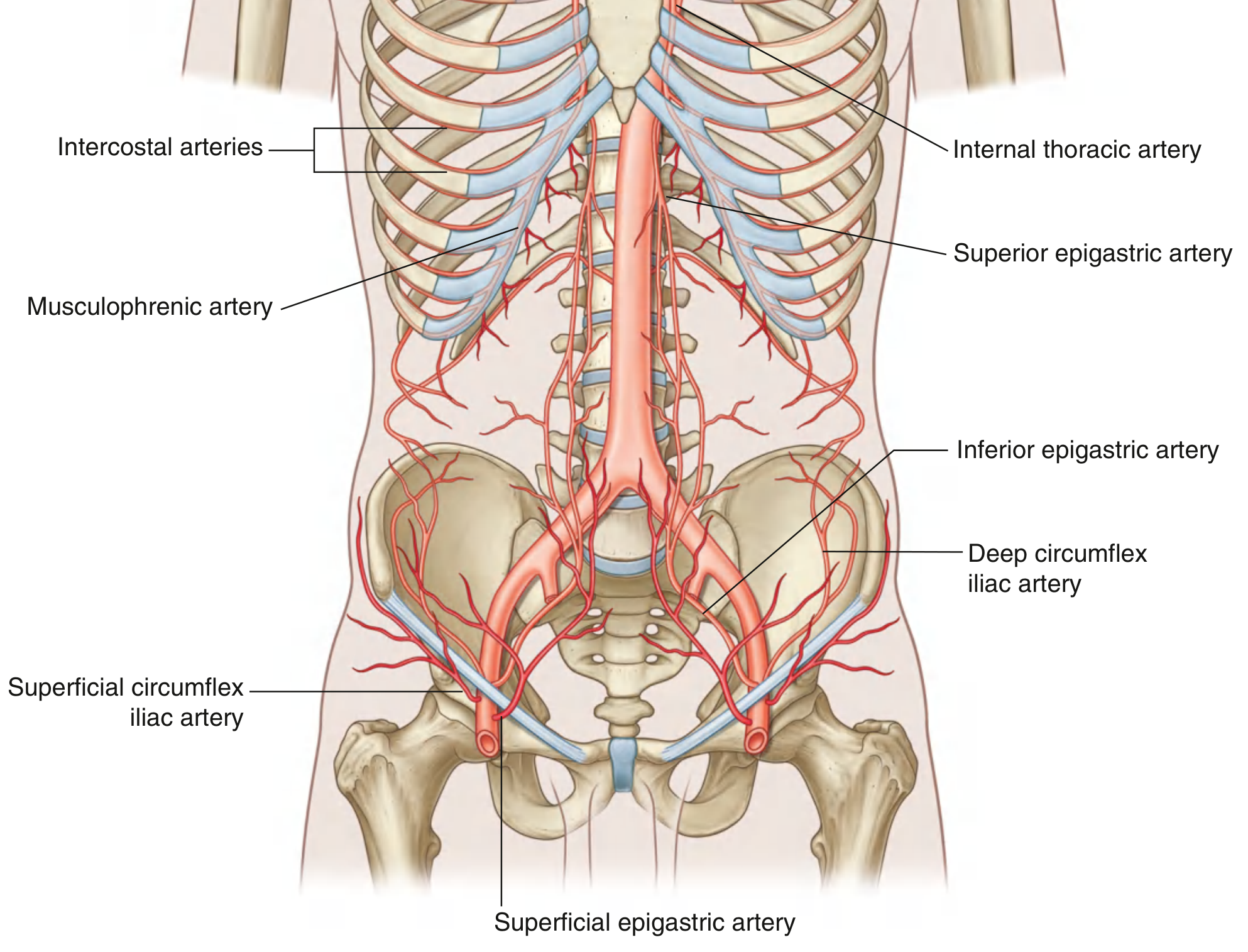
Superficial supply:
- Superior part: branches from the musculophrenic artery (branch of internal thoracic)
- Inferior part: superficial epigastric and superficial circumflex iliac arteries (branches of femoral artery)
Deep supply:
- Superior: superior epigastric artery (terminal branch of internal thoracic)
- Lateral: branches of 10th and 11th intercostal arteries and the subcostal artery
- Inferior: inferior epigastric and deep circumflex iliac arteries (branches of external iliac artery)
The superior and inferior epigastric arteries both enter the rectus sheath, passing posterior to rectus abdominis, and anastomose with each other - a clinically important anastomosis.
Lymphatic Drainage
- Superficial lymphatics above the umbilicus drain superiorly to axillary nodes
- Superficial lymphatics below the umbilicus drain inferiorly to superficial inguinal nodes
3. Peritoneum and Peritoneal Cavity
The peritoneum is a thin serous membrane lining the abdominal cavity walls and covering abdominal viscera:
- Parietal peritoneum: lines the walls
- Visceral peritoneum: covers the viscera
The space between the two layers is the peritoneal cavity - normally a potential space containing only a small volume of fluid for lubrication. The peritoneal sac is:
- Closed in men
- Semi-closed in women (the uterine tubes provide two small openings to the outside)
Innervation of the Peritoneum
- Parietal peritoneum: innervated by somatic afferents (spinal nerves) - sensitive to well-localized pain
- Visceral peritoneum: innervated by visceral afferents with autonomic nerves - produces poorly-localized, referred discomfort
Intraperitoneal vs. Retroperitoneal
- Intraperitoneal organs: suspended in the peritoneal cavity by folds of peritoneum (mesenteries), e.g., stomach, jejunum, ileum, transverse colon, liver, spleen
- Retroperitoneal organs: outside the peritoneal cavity, only partially covered by peritoneum on one surface, e.g., kidneys, aorta, IVC, pancreas, ascending/descending colon, duodenum (most parts)
Clinical: Ascites and Peritoneal Dialysis
When peritoneal fluid volume increases abnormally (ascites - from liver cirrhosis, pancreatitis, heart failure), marked abdominal distension results. The large surface area of the peritoneum also makes it useful as a dialysis membrane in peritoneal dialysis, where dialysis fluid is infused into the peritoneal cavity.
4. The Pelvis
Bony Framework
The pelvis consists of:
- Two hip bones (each formed by ilium, ischium, pubis fused at the acetabulum)
- Sacrum
- Coccyx
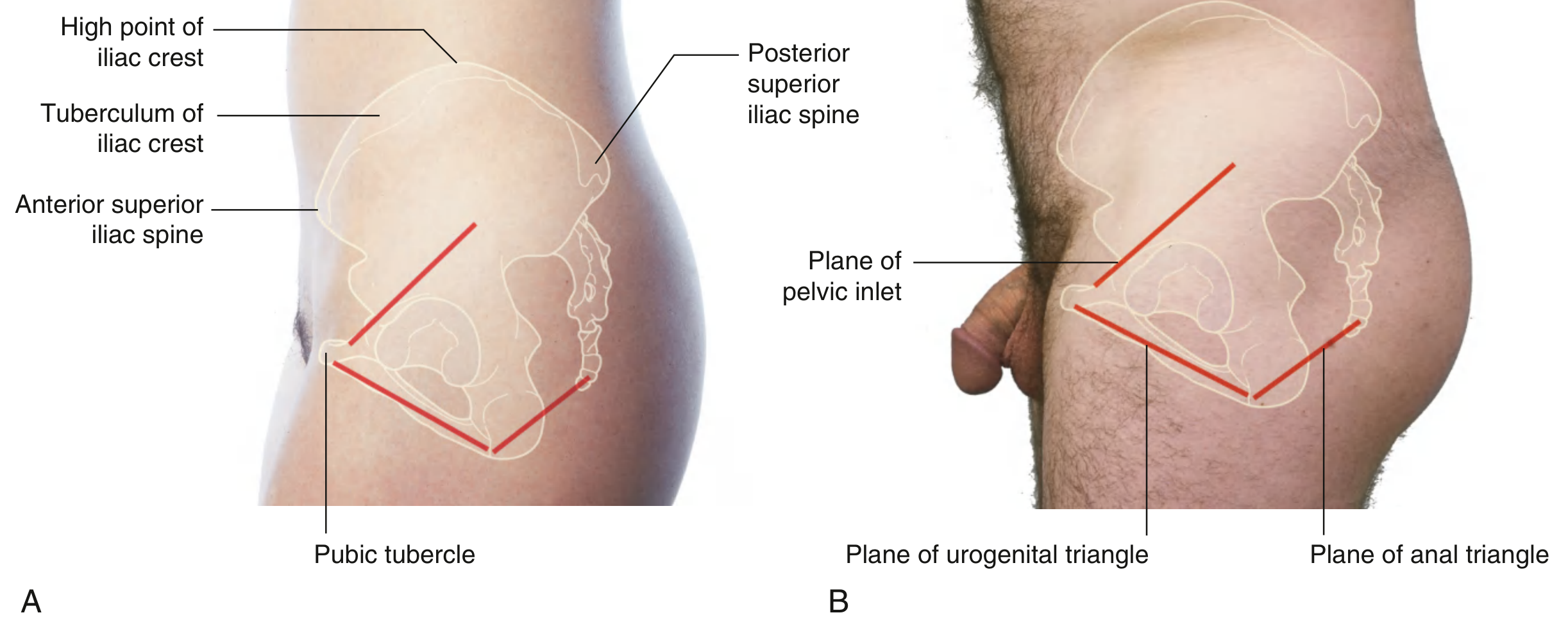
Key bony landmarks:
- Iliac crest: separates the lateral abdominal wall from the gluteal region
- ASIS (anterior superior iliac spine): attachment of the inguinal ligament
- Pubic tubercle: medial attachment of the inguinal ligament
- Ischial tuberosities: define the lateral corners of the diamond-shaped perineum
- Pubic symphysis: anterior midline articulation
The inguinal ligament runs from the ASIS to the pubic tubercle and separates the anterior abdominal wall from the thigh of the lower limb.
Orientation
In the anatomical position, the ASIS and the anterior superior edge of the pubic symphysis lie in the same vertical plane. The pelvic inlet faces anterosuperiorly. The urogenital triangle of the perineum is oriented nearly horizontally and faces inferiorly, while the anal triangle is more vertical and faces posteriorly.
Pelvic Inlet and Outlet
- Pelvic inlet (brim): bounded by the sacral promontory, ala of sacrum, arcuate lines, pectineal lines, and symphysis pubis
- Pelvic outlet: bounded by the pubic symphysis anteriorly, ischial tuberosities laterally, and the tip of the coccyx posteriorly
- Greater (false) pelvis: above the pelvic inlet; contains lower abdominal viscera
- Lesser (true) pelvis: below the pelvic inlet; contains pelvic organs (bladder, rectum, uterus/prostate)
5. Pelvic Floor (Pelvic Diaphragm)
The pelvic floor is formed primarily by the levator ani muscle group and the coccygeus muscle, together forming the pelvic diaphragm. Levator ani includes:
- Pubococcygeus (with the pubovaginalis in women / puboprostaticus in men)
- Puborectalis: forms a sling around the anorectal junction
- Iliococcygeus
All levator ani muscles are innervated by branches of S3-S4 (pelvic splanchnic nerves and the nerve to levator ani).
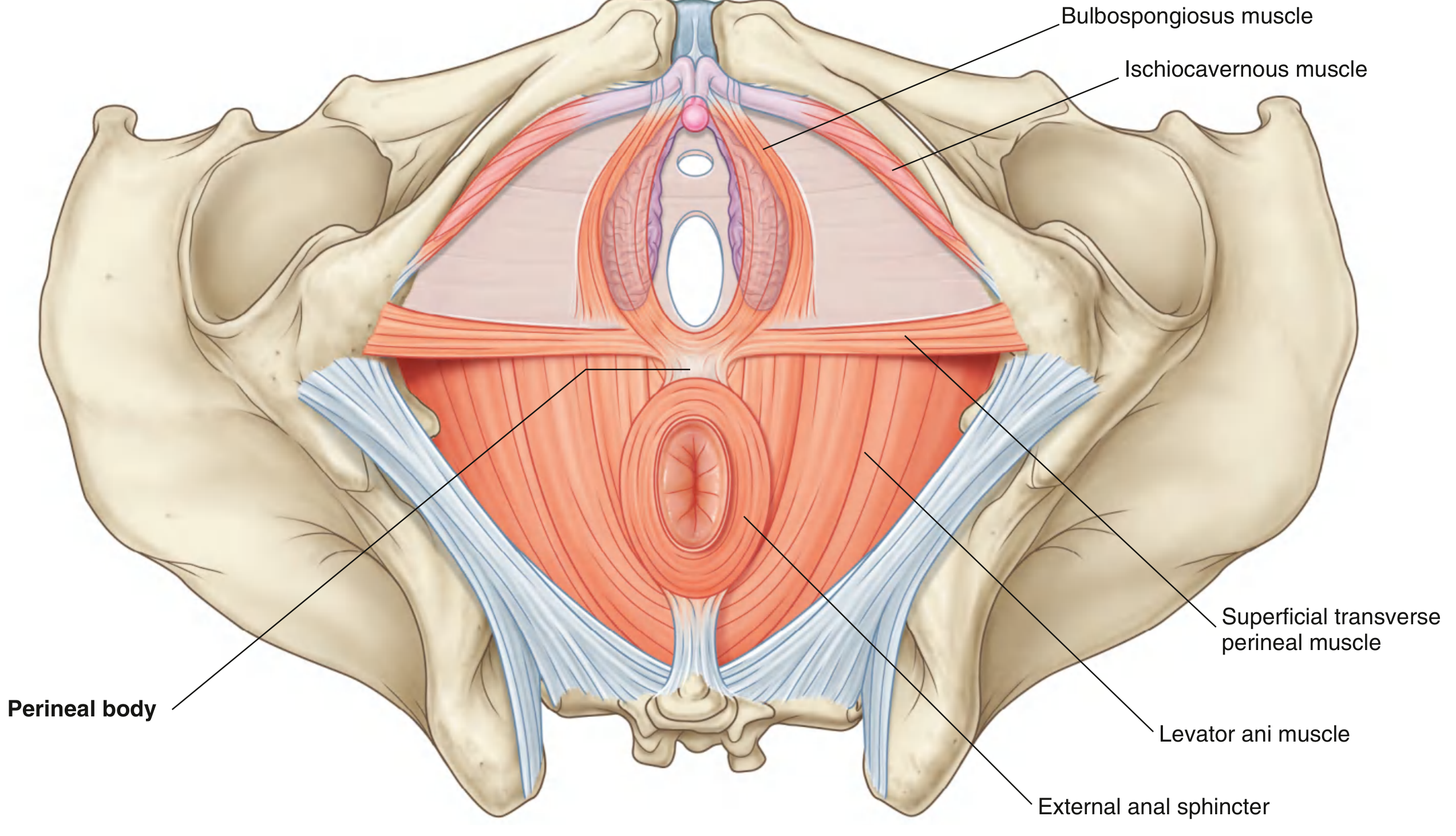
6. Perineum
The perineum is the diamond-shaped region inferior to the pelvic floor, bounded by:
- Anteriorly: pubic symphysis
- Laterally: ischial tuberosities
- Posteriorly: tip of coccyx
A transverse line between the ischial tuberosities divides it into:
- Urogenital triangle (anterior): contains external genitalia and urethral opening
- Anal triangle (posterior): contains the anal canal and external anal sphincter
The Perineal Body
The perineal body is a poorly defined fibromuscular node at the center of the perineum, approximately midway between the two ischial tuberosities. Converging at the perineal body are:
- Levator ani muscles of the pelvic diaphragm
- Muscles of both perineal triangles - including sphincters of the urethra, vagina, and anus
The Urethra
- Female urethra: short, passes inferiorly from the bladder directly through the pelvic floor to open in the perineum
- Male urethra: passes through the prostate, then through the deep perineal pouch and perineal membrane, then becomes enclosed in the erectile tissues of the penis; has a fixed anterior bend at the root of the penis after exiting the perineal membrane (clinically relevant for catheterization)
7. Key Clinical Correlations
| Condition | Anatomical Basis |
|---|---|
| Inguinal hernia | Weakness at the inguinal canal (indirect = through deep ring; direct = through Hesselbach's triangle) |
| Umbilical hernia | Incomplete closure of the umbilicus/linea alba |
| Incisional hernia | Defect through a surgical scar |
| Referred pain from viscera | Visceral peritoneum innervated by autonomic afferents; poorly localized |
| Ascites | Excess fluid in the peritoneal cavity - detectable by percussion and shifting dullness |
| Peritonitis | Somatic innervation of parietal peritoneum = severe, well-localized pain + guarding |
| Catheterization difficulty in males | Fixed anterior bend of urethra at root of penis |
Source: Gray's Anatomy for Students (ISBN 9780323934237)
This is a shared conversation. Sign in to Orris to start your own chat.