Ecg reading from basic
Reading File
Finding Sources
Searching the Web
ECG reading basics systematic approach for beginners 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Searching Images
ECG waves P QRS T labeled diagram normal
Loading Image
Finding Sources
Reading File
I now have comprehensive content from Kaplan & Sadock's, Harrison's, Medical Physiology, and Braunwald's. Let me compile a thorough beginner's guide to ECG reading.
ECG Reading from Basics
What is an ECG?
An electrocardiogram (ECG/EKG) provides a direct measurement of the rate, rhythm, and time-dependent electrical vector of the heart. It records the electrical activity of the heart as it depolarizes and repolarizes, allowing us to identify arrhythmias, conduction defects, ischemia, and much more.
1. The ECG Paper
ECG paper has a grid of small and large boxes:
| Box Type | Time (x-axis) | Voltage (y-axis) |
|---|---|---|
| Small box (1 mm) | 0.04 seconds | 0.1 mV |
| Large box (5 mm) | 0.2 seconds | 0.5 mV |
| 5 large boxes | = 1.0 second | — |
A standard ECG runs for 10 seconds, containing 50 large boxes.
2. The 12 Leads
A standard ECG has 12 leads — each a different electrical "viewpoint" of the heart:
Limb leads (frontal plane):
- I, II, III — standard bipolar leads
- aVR, aVL, aVF — augmented unipolar leads
Precordial leads (horizontal plane):
- V1, V2, V3, V4, V5, V6 — chest leads
3. The Waves, Intervals & Segments
Each heartbeat produces a recognizable waveform:
R
|
P | T
/\ | /\
---/ \---+----/ \--- baseline
|QS
|
[P-R] [QRS] [ST][T]
Waves
| Wave | What it represents |
|---|---|
| P wave | Atrial depolarization |
| QRS complex | Ventricular depolarization |
| T wave | Ventricular repolarization |
| U wave | Small deflection after T wave (sometimes visible) |
QRS Nomenclature
- Q = first negative deflection before R
- R = first positive deflection
- S = negative wave following R
- R' = second positive deflection (e.g., RBBB)
- Capital letters (Q, R, S) = large amplitude; lowercase (q, r, s) = small amplitude
Intervals & Segments
| Interval/Segment | Normal Duration | Measured From → To |
|---|---|---|
| PR interval | 0.12–0.20 s (3–5 small boxes) | Start of P → Start of QRS |
| QRS interval | < 0.12 s (< 3 small boxes) | Start → End of QRS |
| QT interval | Rate-dependent | Start of QRS → End of T wave |
| ST segment | Isoelectric | End of QRS → Start of T wave |
| R-R interval | = 1 cardiac cycle | R peak to next R peak |
4. The 14-Parameter Systematic Approach (Harrison's)
Use this every time you read an ECG — never skip steps:
- Standardization & calibration — Is the gain set to 1 mV/10 mm? Any artifacts?
- Rhythm — Regular or irregular? Identify the pacemaker
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT / QTc interval
- Mean QRS electrical axis
- P waves
- QRS voltages
- Precordial R-wave progression
- Abnormal Q waves
- ST segments
- T waves
- U waves
Always compare with previous ECGs if available.
5. Heart Rate
Method 1 — Rate by Squares (regular rhythm)
Count large boxes between two consecutive R waves (R-R interval):
| Large boxes between R waves | Heart Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
Formula: HR = 300 ÷ (number of large boxes)
Method 2 — Count QRS complexes (irregular rhythm)
Count the number of QRS complexes on the full 10-second strip × 6 = bpm
Normal: 60–100 bpm | Bradycardia: < 60 bpm | Tachycardia: > 100 bpm
6. Rhythm
Ask three questions:
- Where is the pacemaker? (SA node → normal; AV node → junctional; ventricle → ventricular)
- What is the conduction path? (Normal: SA node → AV node → His-Purkinje → ventricles)
- Is it regular and at the correct rate?
Normal Sinus Rhythm (NSR) criteria:
- P wave before every QRS ✓
- QRS after every P wave ✓
- P waves upright in leads I and II ✓
- Regular R-R intervals ✓
- Rate 60–100 bpm ✓
7. Axis
The electrical axis represents the net direction of ventricular depolarization. Use Lead I (0°) and aVF (90°):
| Lead I | aVF | Axis |
|---|---|---|
| Positive (↑) | Positive (↑) | Normal (0° to +90°) |
| Positive (↑) | Negative (↓) | Left axis deviation (LAD) |
| Negative (↓) | Positive (↑) | Right axis deviation (RAD) |
| Negative (↓) | Negative (↓) | Extreme/indeterminate axis |
Normal axis: −30° to +90°
Causes of axis deviation:
- LAD: Left ventricular hypertrophy, left bundle branch block, inferior MI
- RAD: Right ventricular hypertrophy, right bundle branch block, lateral MI, COPD
8. Intervals in Detail
PR Interval
- Normal: 0.12–0.20 s
- Short PR (< 0.12 s): Pre-excitation (WPW syndrome), junctional rhythm
- Long PR (> 0.20 s): First-degree AV block
QRS Duration
- Normal: < 0.12 s (< 3 small boxes)
- Wide QRS (≥ 0.12 s): Bundle branch block, ventricular rhythm, hyperkalemia, drug toxicity
QT Interval
- Rate-dependent — use corrected QTc (Bazett formula: QTc = QT ÷ √R-R)
- Normal QTc: < 440 ms in men, < 460 ms in women
- Prolonged QT: Risk of Torsades de Pointes; caused by drugs (antipsychotics, antibiotics), electrolyte disturbances, congenital long QT syndrome
9. P Waves
- Normal: rounded, upright in I and II, inverted in aVR
- Tall & peaked P (> 2.5 mm in II): Right atrial enlargement ("P pulmonale")
- Broad & notched P (> 0.12 s in II): Left atrial enlargement ("P mitrale")
- Absent P waves: Atrial fibrillation (irregular baseline), junctional rhythm
10. QRS Complex — Key Abnormalities
Bundle Branch Blocks
| Feature | RBBB | LBBB |
|---|---|---|
| QRS duration | ≥ 0.12 s | ≥ 0.12 s |
| Pattern in V1 | rSR' ("M" shape) | Broad negative (QS) |
| Pattern in V6 | Wide S wave | Broad R, no Q or S |
| T wave | Opposite to terminal QRS | Opposite to QRS |
R-Wave Progression (precordial leads)
- Normal: R wave grows from V1 → V5 (transition zone V3–V4)
- Poor R-wave progression: Anterior MI, LBBB, COPD
Pathological Q waves
- Significant Q wave: width ≥ 0.04 s OR depth ≥ 1/4 of R wave height
- Indicates prior myocardial infarction (dead tissue produces no electrical activity)
11. ST Segment & T Wave
ST Segment
| Finding | Significance |
|---|---|
| ST elevation ≥ 1 mm (≥ 2 mm in V1–V3) | STEMI (acute MI), pericarditis (diffuse, saddle-shaped), Prinzmetal angina |
| ST depression | NSTEMI/unstable angina, subendocardial ischemia, digoxin effect |
| J-point elevation | Early repolarization (normal variant in young adults) |
T Waves
- Normal: upright in I, II, V3–V6; inverted in aVR; variable in III and V1
- Hyperacute T waves (tall, peaked): Earliest sign of acute STEMI; also hyperkalemia
- Inverted T waves: Ischemia, ventricular strain, bundle branch blocks, pulmonary embolism (V1–V4)
- Flattened T waves: Electrolyte disturbance, ischemia
12. Summary: Quick Reading Sequence
RRAQQST — a simple memory aid:
- Rate
- Rhythm
- Axis
- QRS width + morphology
- QT interval
- ST segment
- T waves (+ P waves + PR interval)
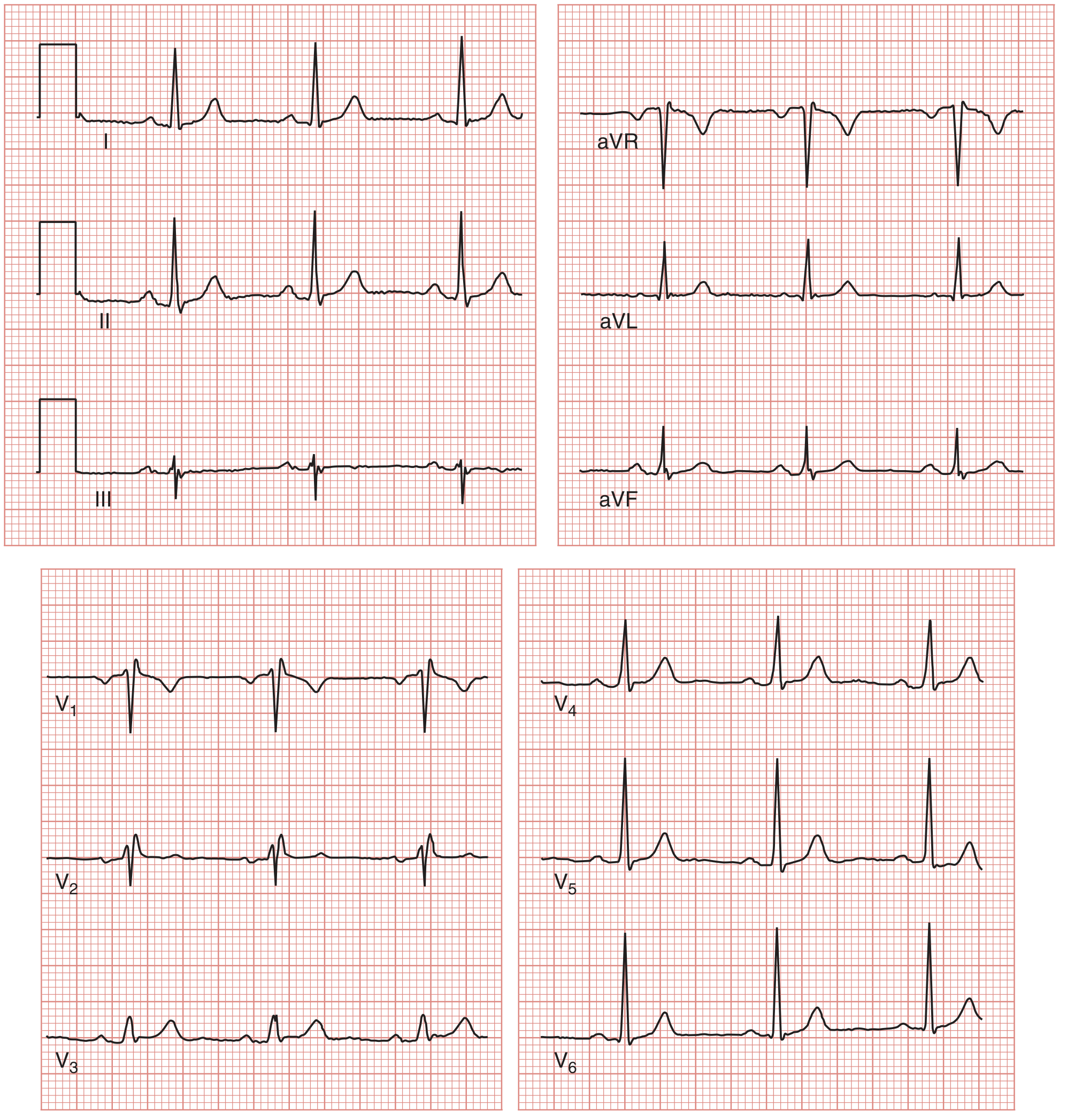
Example: Normal ECG
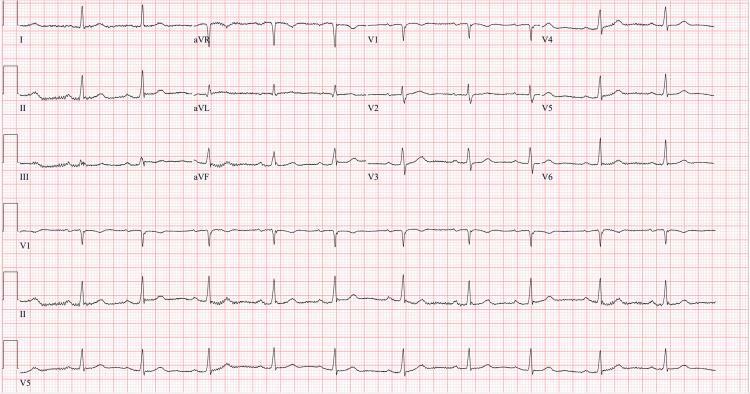
Normal sinus rhythm at ~64 bpm — upright P waves before every QRS, isoelectric ST segments, normal R-wave progression V1→V6, upright T waves V3–V6.
Key Normal Values — Quick Reference
| Parameter | Normal Value |
|---|---|
| Heart rate | 60–100 bpm |
| PR interval | 0.12–0.20 s |
| QRS duration | < 0.12 s |
| QTc (men / women) | < 440 ms / < 460 ms |
| Axis | −30° to +90° |
| P wave amplitude | < 2.5 mm |
| P wave duration | < 0.12 s |
Sources: Medical Physiology (Boron & Boulpaep), Harrison's Principles of Internal Medicine 22e, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.