Mi
It looks like your message got cut off! Could you complete your thought? What would you like help with?
Myocardial infarction
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"myocardial infarction" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have excellent material from multiple authoritative sources. Let me compile the full clinical review.
Myocardial Infarction - Comprehensive Clinical Review
1. Definition & Epidemiology
Myocardial infarction (MI) is the death of cardiac muscle due to prolonged ischemia, most commonly from acute coronary arterial occlusion superimposed on atherosclerosis. In the United States, approximately 800,000 individuals experience an MI each year (nearly one every 40 seconds), causing close to 400,000 deaths annually.
-
10% occur in people under 40; 45% in people under 65
-
Male sex is a risk factor through middle age; postmenopausal women lose estrogen-related protection and IHD becomes the leading cause of death in older females
-
STEMI accounts for ~25-30% of ACS cases; its incidence is declining
-
Out-of-hospital mortality from STEMI remains ~30%, with one-third of deaths from arrhythmia within the first hour
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 511
-
Washington Manual of Medical Therapeutics, p. 146
2. Pathogenesis
Typical Atherothrombotic Mechanism (~90% of cases)
The sequence underlying most MIs:
- Plaque disruption - an atheromatous plaque is eroded or suddenly ruptured by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic plaque contents
- Platelet activation - platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin, causing further aggregation and vasospasm
- Coagulation cascade - activation by tissue factor adds to the growing thrombus
- Complete occlusion - within minutes the thrombus can fully occlude the lumen
Importantly, the culprit lesion is usually not at a site of critical (>70%) pre-existing stenosis - most ruptures occur at previously non-flow-limiting plaques.
STEMI vs. NSTEMI
- STEMI: Complete, total occlusion of an epicardial coronary artery → full transmural ischemia
- NSTEMI/UA: Partial occlusion or complete occlusion with good collaterals → subendocardial ischemia
Atypical Mechanisms (~10% of cases)
-
Vasospasm (cocaine, ephedrine)
-
Embolism (from LV mural thrombus, AF, endocarditis, PFO)
-
Vasculitis, sickle cell disease, amyloid deposition
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 511-512
3. Anatomy of Infarction
The territory involved depends on the vessel occluded (in a right-dominant heart):
| Vessel | Frequency | Infarct Territory |
|---|---|---|
| LAD | 40-50% | Anterior LV wall, anterior septum, apex |
| RCA | 30-40% | Inferior/posterior LV wall, posterior septum, may involve RV |
| LCx | 15-20% | Lateral LV wall (except apex) |
-
Isolated RV infarction is unusual (1-3% of cases)
-
RCA occlusion extends into the RV in 15-30% of posterior MI cases
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 512
4. Morphologic Evolution (Pathology)
The temporal sequence of gross and histologic changes is highly predictable:
| Time | Gross Appearance | Histology |
|---|---|---|
| < 12 hours | Usually not visible grossly (TTC stain shows pale/unstained zone) | Wavy fibers; subtle nuclear/cytoplasmic changes |
| 12-24 hours | Reddish-blue discoloration (congestion, extravasated blood) | Early coagulative necrosis, neutrophil infiltration begins |
| 3-7 days | Rimmed by hyperemic granulation tissue; soft, yellow-tan | Brisk neutrophil infiltration; myocyte ghosts |
| 1-3 weeks | Progressive yellow-tan softening; defined margins | Macrophage/monocyte infiltration; removal of necrotic debris; granulation tissue forms |
| Weeks-months | Fibrotic scar (gray-white) | Dense collagen scar; electrically silent |
Key point: The dead scar is electrically silent. The infarcted zone is negative relative to normal myocardium during systole - this produces the pathological Q wave.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 513
5. Electrocardiographic Changes
Based on three concurrent membrane abnormalities in infarcted cells:
| Defect | Current Flow | ECG Change (lead over infarct) |
|---|---|---|
| Rapid repolarization (accelerated K+ channel opening) | Out of infarct | ST segment elevation |
| Decreased resting membrane potential (K+ loss) | Into infarct | TQ depression (manifests as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
Evolution:
-
Hyperacute T waves - very earliest finding (minutes)
-
ST elevation - hallmark of acute transmural injury; leads opposite the infarct show reciprocal ST depression
-
Q wave development - days to weeks; pathological Q = >40 ms wide or >25% of R wave height
-
Non-Q-wave infarcts - tend to be less transmural but carry a high risk of re-infarction
-
Ganong's Review of Medical Physiology, p. 534
6. Clinical Presentation & Diagnosis
Typical Presentation
- Severe, crushing/pressure chest pain, often radiating to left arm, jaw, or back
- Diaphoresis, nausea, vomiting
- Dyspnea
- Sense of impending doom
Atypical Presentation (high-risk groups)
Women, elderly, diabetics, patients with CKD, and postoperative patients may present with:
- No chest pain (silent MI)
- Confusion, unexplained hypotension, or heart failure as the presenting feature
Always consider STEMI when any patient is hemodynamically compromised.
Diagnostic Triad
- History - clinical symptoms
- ECG - ST elevation in ≥2 contiguous leads, or new LBBB
- Biomarkers - troponin I or T (most sensitive/specific); CK-MB (rises in 4-6 hours, peaks 18-24 hours, normalizes in 3-4 days - useful for re-infarction)
- Washington Manual of Medical Therapeutics, p. 146
7. Management
Immediate General Measures (MONA + anticoagulation)
- O2 - if SpO2 < 90% or respiratory distress
- Nitrates - vasodilation, reverse vasospasm (avoid in RV infarction, hypotension, or recent PDE5 inhibitor use)
- Antiplatelet therapy - aspirin (loading dose immediately), plus a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel)
- Anticoagulation - unfractionated heparin, LMWH, fondaparinux, or bivalirudin (direct thrombin inhibitor)
- Beta blockers - reduce myocardial O2 demand and arrhythmia risk (avoid if acute HF, cardiogenic shock, bradycardia, or bronchospasm)
- Pain control - morphine (use judiciously; observational data suggest possible harm with opioids in NSTEMI)
Reperfusion - The Central Priority
"Mortality is directly related to total ischemia time."
| Strategy | Preferred When |
|---|---|
| Primary PCI (preferred) | Available within 90 min of first medical contact (120 min if transfer required) |
| Fibrinolysis | PCI not available within time targets, no contraindications; give within 12 hours of symptom onset |
| CABG | Multi-vessel disease identified at angiography, or failed PCI with ongoing ischemia |
Secondary Prevention
-
High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg)
-
Dual antiplatelet therapy (DAPT) for 12 months post-PCI
-
ACE inhibitor/ARB (especially with reduced EF, anterior MI, or diabetes)
-
Beta blocker (long-term for reduced EF)
-
Aldosterone antagonist (eplerenone/spironolactone) if EF ≤ 40% with HF symptoms
-
Cardiac rehabilitation
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 514
-
Washington Manual of Medical Therapeutics, p. 147
8. Complications
Nearly three-quarters of patients experience one or more complications:
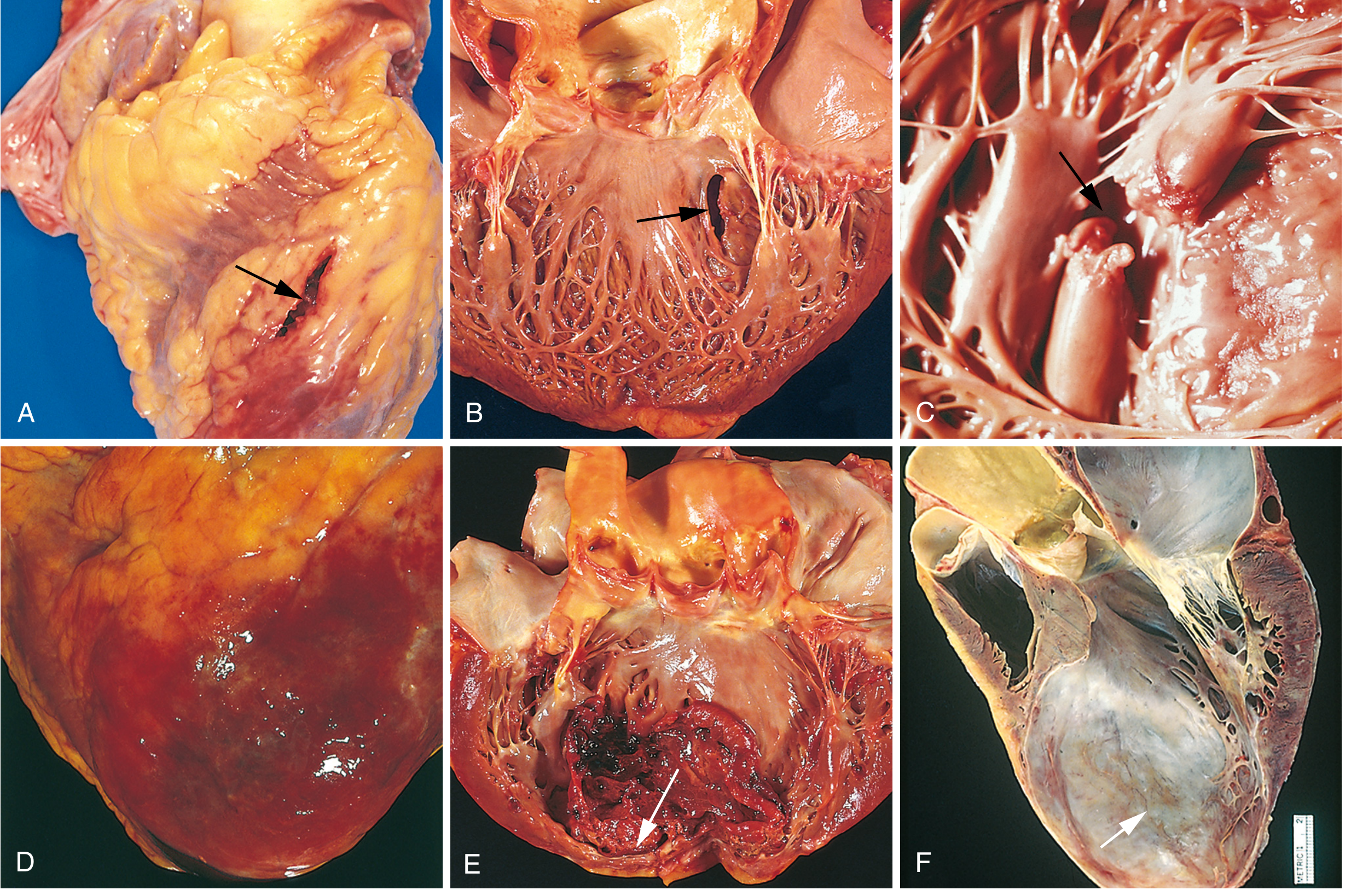
Fig. 12.17 from Robbins, Cotran & Kumar - Complications of MI: (A) Anterior free wall rupture, (B) Ventricular septal rupture, (C) Papillary muscle (complete rupture), (D) Fibrinous pericarditis, (E) Mural thrombus in LV, (F) LV aneurysm
Mechanical Complications (Early, within days)
| Complication | Timing | Features |
|---|---|---|
| Free wall rupture | 3-7 days | Sudden hemopericardium → cardiac tamponade → death; more common in women, elderly, first MI, anterior location |
| Ventricular septal defect (VSD) | 3-7 days | New harsh holosystolic murmur, step-up in O2 saturation RV vs. RA on right heart cath |
| Papillary muscle rupture | 2-7 days | Acute severe mitral regurgitation, pulmonary edema |
| Cardiogenic shock | Hours-days | Infarct involves ≥40% of LV; ~10% of transmural MIs; mortality 90% if mechanical complication present |
Without mechanical complications, mortality from STEMI if untreated can exceed 30%; with mechanical complications mortality rises to ~90%.
Arrhythmias
- VF - most common cause of death (~50% of mortality), usually within first hour
- VT, heart block (especially inferior MI involving RCA and AV nodal artery), atrial fibrillation, accelerated idioventricular rhythm (reperfusion arrhythmia - generally benign)
Heart Failure
- LV pump failure proportional to mass of damaged myocardium
- Killip classification grades severity (I = no HF → IV = cardiogenic shock)
- Pulmonary edema in severe cases
Later Complications
| Complication | Timing | Notes |
|---|---|---|
| Pericarditis (Dressler syndrome) | 1-8 weeks | Autoimmune; fever, pleuritic chest pain, friction rub; treat with NSAIDs/colchicine |
| LV aneurysm | Weeks | Persistent ST elevation, mural thrombus risk, refractory HF |
| Mural thrombus | Days-weeks | Risk of systemic embolism; anticoagulate |
| RV infarction | Acute | Hypotension + clear lungs + elevated JVP (Kussmaul's sign); avoid nitrates and diuretics; aggressive fluid resuscitation |
| Sudden cardiac death | Long-term | Risk highest in those with reduced EF post-MI |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 514-515
- Washington Manual of Medical Therapeutics, p. 146-147
9. Recent Evidence Updates (2024-2025)
A few recent high-level studies are worth noting:
- Antiplatelet secondary prevention - A 2025 individual-patient data meta-analysis in The Lancet compared clopidogrel vs. aspirin for secondary prevention of CAD, finding clopidogrel superior to aspirin in several outcomes (PMID 40902613)
- Anticoagulation in AF + stable CAD - A 2025 JACC meta-analysis found that OAC alone (without antiplatelet) may be sufficient in stable coronary disease with AF, avoiding excess bleeding of triple therapy (PMID 39918465)
- Sudden cardiac death post-MI - A 2024 European Heart Journal pooled cohort study found that SCD risk post-MI is highest in the first year, with reduced EF being the dominant predictor (PMID 39378245)
Summary Table
| Domain | Key Point |
|---|---|
| Pathogenesis | Plaque rupture → thrombus → complete occlusion (STEMI) or partial occlusion (NSTEMI) |
| Vessel | LAD most common (40-50%); RCA 30-40%; LCx 15-20% |
| ECG | Hyperacute T → ST elevation → Q waves; reciprocal changes opposite |
| Biomarkers | Troponin (most sensitive); CK-MB useful for re-infarction |
| Management | Time = myocardium: Primary PCI < 90 min; fibrinolysis if PCI delayed |
| Complications | VF (most common cause of death), free wall rupture (3-7 days), VSD, papillary rupture, cardiogenic shock, Dressler syndrome |
| Secondary prevention | Statin + DAPT + ACEi/ARB + beta blocker + cardiac rehab |
This is a shared conversation. Sign in to Orris to start your own chat.