Approach to pneumonia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have extensive, authoritative content from Goldman-Cecil and Fishman's to craft a thorough clinical approach to pneumonia. Let me compile the final answer.
Approach to Pneumonia
1. Definition
Pneumonia is an infection of the pulmonary parenchyma, from the respiratory bronchioles to the alveoli. Clinically it is recognized by a new lung infiltrate plus at least one of: new/increased cough, dyspnea, pleuritic chest pain, purulent sputum, confusion, fever, hypoxemia, rales, leukocytosis, or leukopenia. - Fishman's Pulmonary Diseases and Disorders, p. 2255
2. Classification by Setting
| Type | Definition |
|---|---|
| Community-Acquired Pneumonia (CAP) | Pneumonia in a community-dwelling individual |
| Hospital-Acquired Pneumonia (HAP) | Occurs ≥48 hours after hospital admission |
| Ventilator-Associated Pneumonia (VAP) | Occurs ≥48 hours after endotracheal intubation |
Note: The "HCAP" category has been removed from current IDSA-ATS guidelines due to poor specificity, which drove antibiotic overtreatment. - Fishman's, p. 2255
3. Epidemiology & Risk Factors
- CAP accounts for 1.5 million annual ED visits in the United States and is the 8th leading cause of death
- Hospitalization rates rise exponentially with age: ~1-2/1000 in young adults to ~40/1000 in those ≥85 years
- 30-day mortality for hospitalized CAP: ~6% in-hospital, ~15% at 1 month
- 1-year mortality post-hospitalization approaches one-third; rises to ~50% for ICU-level CAP
Risk factors:
-
Age (strongest risk factor), male sex, smoking, poor dental hygiene, crowded living
-
Comorbidities: malnutrition, alcohol use disorder, chronic immunosuppression, COPD, neurologic disease (impaired gag reflex)
-
Medications: opioids, proton pump inhibitors, corticosteroids, other immunosuppressants
-
Goldman-Cecil Medicine, p. 992
4. Pathobiology
The lung is not sterile - the normal microbiome (dominated by Prevotella, Veillonella, Streptococcus) maintains homeostasis. Pneumonia represents a disruption of this balance, allowing a pathogen to become dominant and trigger inflammation.
Routes of infection:
- Microaspiration - the primary mechanism for most bacterial pneumonias
- Inhalation of aerosols - e.g., TB, Legionella, anthrax
- Hematogenous spread - e.g., S. aureus right-sided endocarditis
Key defense mechanisms impaired in pneumonia:
- Mucociliary clearance
- Surfactant bacteriostasis
- Innate and adaptive immunity
- Cough reflex
5. Etiology
Common Pathogens in CAP
| Category | Pathogens |
|---|---|
| Typical bacteria | S. pneumoniae (most common), H. influenzae, S. aureus, gram-negative bacilli |
| Atypical bacteria | Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila |
| Respiratory viruses | Influenza, RSV, hMPV, SARS-CoV-2 (~20-30% of cases, higher during COVID era) |
| No pathogen identified | >50% of cases |
Pneumococcus, H. influenzae, S. aureus, and gram-negative bacilli together cause up to 30% of cases; atypicals (Mycoplasma, Chlamydia, Legionella) cause <5% each. - Goldman-Cecil, p. 992
Epidemiologic Clues to Unusual Pathogens
| Exposure/Context | Consider |
|---|---|
| SW United States | Coccidioides immitis |
| Mississippi River Valley, bats | Histoplasma capsulatum |
| Birds (parrots, parakeets) | Chlamydia psittaci |
| Pigeons | Cryptococcus neoformans |
| Rabbits | Francisella tularensis |
| Farm animals | Coxiella burnetii (Q fever) |
| Active influenza in community | Influenza virus, S. aureus, S. pneumoniae |
| Bronchiectasis / cystic fibrosis | Pseudomonas aeruginosa, Burkholderia, MRSA |
| Aspiration / poor dentition | Mouth anaerobes, Candida |
| Pandemic context | SARS-CoV-2 |
- Goldman-Cecil Medicine, p. 996
6. Clinical Manifestations
Typical (lobar) pneumonia:
- Abrupt onset fever, rigors, productive cough (rust-colored sputum suggests pneumococcus)
- Pleuritic chest pain, dyspnea
- Signs of consolidation: dullness to percussion, bronchial breath sounds, egophony, increased tactile fremitus
Atypical pneumonia:
- Gradual onset, dry cough, lower-grade fever
- "Walking pneumonia" - patient ambulatory
- Extrapulmonary features (headache, myalgia, rash, GI symptoms) common with Mycoplasma, Chlamydia, Legionella
Important: Neither history nor physical examination alone is sufficient to reliably confirm or exclude CAP, or to reliably distinguish typical from atypical organisms. - Fishman's, p. 2258
7. Diagnostic Approach
Step 1: Confirm the Diagnosis
- Chest X-ray (PA and lateral): New infiltrate is the radiographic cornerstone. Patterns:
- Lobar consolidation - typical bacterial (pneumococcal)
- Interstitial/bilateral - viral or atypical
- Cavitation - S. aureus, anaerobes, gram-negatives, TB, fungi
- CT chest: more sensitive; useful when CXR is equivocal, immunocompromised host, or suspected complication
Step 2: Assess Severity
CURB-65 Score (simple, quick bedside tool)
| Feature | Points |
|---|---|
| Confusion | 1 |
| Urea >7 mmol/L (BUN >19 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure <90 systolic or ≤60 diastolic | 1 |
| Age ≥65 years | 1 |
- Score 0-1: Outpatient treatment
- Score 2: Consider inpatient
- Score ≥3: Hospitalize; consider ICU if ≥4-5
Pneumonia Severity Index (PSI / PORT Score) - more detailed risk stratification
| PSI Class | 30-day Mortality |
|---|---|
| Class II (≤70 points) | <1-3% |
| Class III (71-90 points) | 3-4% |
| Class IV (91-130 points) | 8% |
| Class V (>130 points) | 25% |
Key PSI variables include: demographics, nursing home residence, comorbidities (neoplasm, liver/renal/heart disease, stroke), physical findings (altered mentation, RR ≥30, temp extremes, HR ≥125), and labs (pH <7.35, BUN ≥30 mg/dL, Na <130, glucose ≥250, Hct <30%, PaO2 <60 mmHg, pleural effusion). - Goldman-Cecil, p. 996
IDSA/ATS Criteria for Severe CAP (ICU admission):
- 1 major criterion: Mechanical ventilation or septic shock requiring vasopressors
- OR ≥3 minor criteria: RR ≥30, PaO2/FiO2 ≤250, multilobar infiltrates, confusion, BUN ≥20 mg/dL, leukopenia (WBC <4000), thrombocytopenia (<100,000), hypothermia (<36°C), hypotension requiring aggressive fluid resuscitation
Step 3: Laboratory Investigations
| Test | When / Purpose |
|---|---|
| CBC with differential | Leukocytosis (typical) or leukopenia (severe/viral) |
| BMP (BUN, creatinine, electrolytes, glucose) | Severity scoring; assess organ dysfunction |
| Liver function tests | Comorbidity assessment |
| Blood cultures (x2) | All hospitalized patients; positive in ~5-10% |
| Sputum Gram stain + culture | Hospitalized patients, especially severe CAP; requires good specimen (>25 PMNs, <10 squamous cells/LPF) |
| Procalcitonin | Helps distinguish bacterial from viral; guides antibiotic stewardship |
| Blood gas (ABG) | Assess oxygenation/ventilation in severe disease |
| HIV test | All patients 15-54 years (IDSA recommendation) |
| Urinary antigens | Severe CAP: both Legionella (serogroup 1, sensitivity 74%, specificity 99%) and S. pneumoniae (sensitivity 74%, specificity 97%) |
| Influenza PCR/NAAT | When influenza circulating in community |
| Multiplex respiratory PCR | Growing utility for viral and atypical pathogen detection |
- Fishman's, p. 2258
8. Differential Diagnosis
Always consider non-infectious causes, especially when patient does not respond to antibiotics (~15-20% of hospital admissions for "pneumonia" have non-infectious etiology):
- Acute heart failure (most common non-infectious mimic in elderly; check BNP)
- Pulmonary embolism with infarction (pleuritic pain + infiltrate)
- Lung cancer (post-obstructive pneumonia)
- ARDS (from any cause)
- Acute bronchitis (fever + cough but NO infiltrate)
- Organizing pneumonia (COP/BOOP) - responds to steroids not antibiotics
- Eosinophilic pneumonia, vasculitis, sarcoidosis
9. Treatment
Outpatient CAP
| Patient Type | Preferred Regimen |
|---|---|
| No comorbidities, no recent antibiotics | Amoxicillin 1g TID OR Doxycycline 100 mg BID OR Azithromycin (if macrolide resistance <25% locally) |
| With comorbidities (DM, heart/lung/liver/renal disease, alcoholism, immunocompromise) | Respiratory fluoroquinolone (levofloxacin 750 mg OD or moxifloxacin 400 mg OD) OR β-lactam + macrolide combination |
Caution: Fluoroquinolones carry risks of tendinopathy, aortopathy, neuropathy, hypoglycemia, psychiatric effects, and may mask/delay TB diagnosis. Stewardship programs increasingly restrict their use. - Fishman's, p. 2258
Hospitalized CAP (Non-Severe)
| Regimen | Details |
|---|---|
| β-lactam + macrolide | Ampicillin-sulbactam or ceftriaxone PLUS azithromycin (preferred IDSA-ATS) |
| Respiratory fluoroquinolone monotherapy | Levofloxacin or moxifloxacin |
Severe CAP / ICU
| Regimen | Details |
|---|---|
| Standard | Antipseudomonal β-lactam (piperacillin-tazobactam, cefepime, or carbapenems) PLUS respiratory fluoroquinolone OR azithromycin |
| If MRSA suspected | Add vancomycin or linezolid |
| Adjunctive corticosteroids | Dexamethasone or methylprednisolone - shown to improve outcomes in severe CAP; also benefit in severe COVID-19 requiring supplemental O2/ventilation |
A 2025 network meta-analysis (PMID: 40602496) evaluated empiric antibiotic regimens for moderate-to-severe CAP. A 2025 meta-analysis in Lancet Respiratory Medicine (PMID: 39892408) provides updated data on predicting benefit from adjunctive corticosteroids.
Aspiration Pneumonia
- Anaerobic coverage is NOT routinely recommended in the absence of lung abscess or empyema (IDSA-ATS 2019 guideline update)
- Standard β-lactam coverage is generally adequate
Drug-Resistant Pathogens (MRSA / Pseudomonas)
Risk factors for MRSA CAP:
- Previous MRSA infection/colonization
- Recurrent skin infections
- Severe disease
Risk factors for Pseudomonas CAP:
- Prior Pseudomonas infection/colonization
- Tracheostomy
- Bronchiectasis, cystic fibrosis
- Invasive respiratory support
- Very severe COPD
A 2025 systematic review and meta-analysis (PMID: 40107661) updated risk factor profiles for drug-resistant pathogens in CAP.
10. Duration of Therapy
- Minimum 5 days for most uncomplicated CAP (IDSA-ATS)
- Clinical stability criteria for stopping: afebrile for ≥48h, HR <100, RR <24, SBP >90, SpO2 ≥90% on room air, tolerating oral intake, normal mental status
- Procalcitonin-guided therapy can safely reduce duration
11. Supportive Care & Monitoring
- Supplemental oxygen to maintain SpO2 ≥94% (≥90% in COPD)
- IV fluids if dehydrated or hypotensive
- Chest physiotherapy, incentive spirometry
- DVT prophylaxis in hospitalized patients
- Monitor for complications: empyema (3-5%), atrial fibrillation and cardiac events (20-25% of hospitalized CAP), parapneumonic effusion
- Repeat CXR not needed in uncomplicated cases with good clinical response; radiographic clearance may lag 6-8 weeks in elderly
12. Complications
| Complication | Notes |
|---|---|
| Empyema | 3-5% of hospitalized CAP; requires drainage + extended antibiotics |
| Parapneumonic effusion | Thoracentesis if moderate/large or patient not improving |
| Lung abscess | Cavitation; prolonged antibiotics 4-6 weeks |
| Respiratory failure / ARDS | ICU, mechanical ventilation |
| Sepsis | Multi-organ dysfunction |
| Cardiac events | AF, new/worsening heart failure, myocardial ischemia in 20-25% of hospitalized patients |
13. Prevention
| Vaccine | Target Population |
|---|---|
| Pneumococcal vaccines (PCV15, PCV20, PPSV23) | All adults ≥65; high-risk adults ≥19 |
| Influenza vaccine | Annual for all ≥6 months of age |
| COVID-19 vaccine | Universal (updated booster recommendations) |
Smoking cessation, good oral hygiene, and minimizing aspiration risk (especially in elderly and neurologically impaired patients) are important non-pharmacological preventive measures. - Goldman-Cecil, p. 992
Key Sources:
- Goldman-Cecil Medicine (International Edition, 2-Vol Set), Chapter 85 - Community-Acquired Pneumonia, pp. 992-996
- Fishman's Pulmonary Diseases and Disorders (2-Volume Set), CAP chapter, pp. 2255-2260
- IDSA/ATS Consensus Guidelines on the Management of CAP (2019 update)
Tuberculosis
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive TB content. I have the full picture - pathogen, pathobiology, spectrum of infection, clinical manifestations, diagnosis, treatment of latent TB, active TB, drug-resistant TB, HIV-TB coinfection. Let me now compile the complete response.
Tuberculosis - Clinical Approach
Spectrum of TB Infection
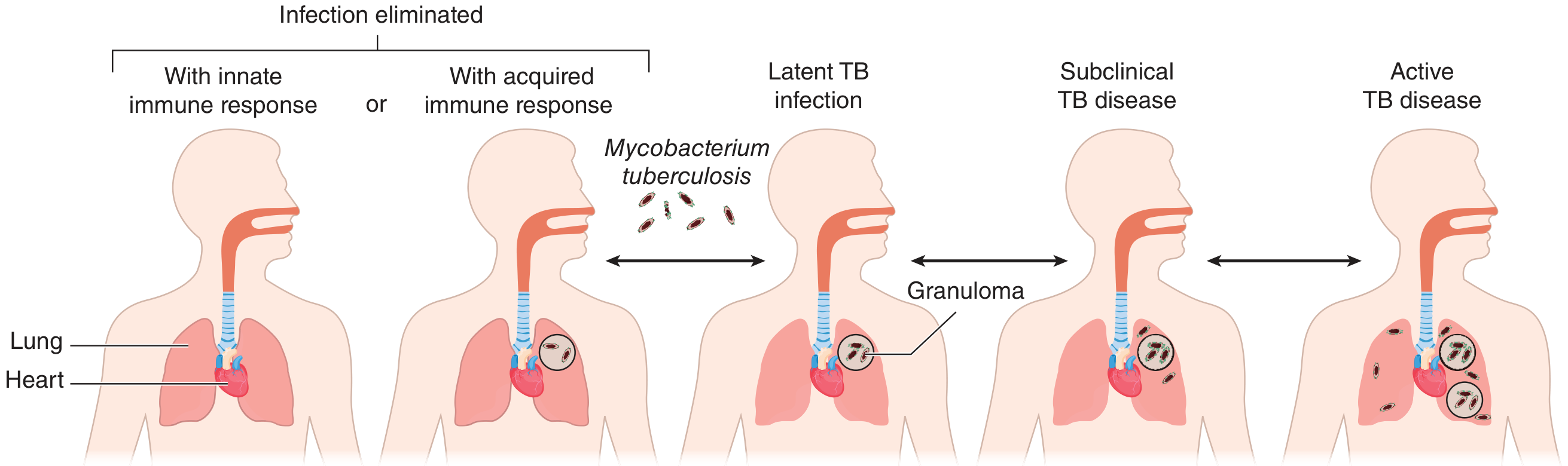
Spectrum of outcomes after M. tuberculosis infection. Granuloma formation is central to containment. States are dynamic and can shift in either direction. - Goldman-Cecil Medicine, p. 3252
1. Definition & The Pathogen
Tuberculosis is a granulomatous disease caused by Mycobacterium tuberculosis, a slow-growing acid-fast bacillus (AFB). Before COVID-19, TB was the leading infectious cause of death worldwide.
Key microbiological features of M. tuberculosis:
- Rod-shaped, ~2-4 μm; obligate human pathogen, no environmental reservoir
- Doubles every 18-24 hours (extremely slow - cultures take weeks)
- "Waxy" cell envelope: contains mycolic acids, arabinogalactan, peptidoglycan - creates barrier to antibiotics and causes acid-fast staining (carbol fuchsin retained after acid wash)
- Facultative anaerobe; replicates intracellularly within macrophages
- Staining: Ziehl-Neelsen (ZN) stain - appears as red bacilli on blue background; Auramine-rhodamine fluorescent stain (more sensitive)
M. bovis (from infected cattle/unpasteurized dairy) can infect humans but human-to-human spread is rare. - Goldman-Cecil Medicine, p. 3246
2. Epidemiology & Transmission
- TB remains a major global health problem - ~10 million new cases/year worldwide
- Transmitted exclusively by aerosol from a person with active pulmonary/laryngeal TB
- Droplet nuclei (1-5 μm) remain suspended in air for hours; single-celled particles can reach the alveoli
- Risk of infection after exposure depends on: infectiousness of source case (smear-positive > smear-negative), duration and proximity of contact, ventilation of environment
Risk factors for progression from infection to active disease:
| Risk Factor | Approximate Relative Risk |
|---|---|
| HIV infection (CD4 <200) | 50-100x |
| Recent infection (<2 years) | 10-15x |
| TNF-α inhibitors (biologics) | 10-25x |
| Silicosis | 10x |
| Solid organ transplant | 5-10x |
| Diabetes mellitus | 2-3x |
| Malnutrition, underweight | 2-3x |
| Chronic renal failure / hemodialysis | 3-5x |
| Smoking | 2-3x |
| Alcohol use disorder | 3x |
A 2024 Cochrane meta-analysis (PMID: 39177079) confirmed diabetes as a significant independent risk factor for TB disease.
3. Pathobiology
Primary Infection
- Inhaled droplet nuclei reach alveoli → engulfed by alveolar macrophages
- M. tuberculosis survives intracellularly by inhibiting phagosome-lysosome fusion
- Bacilli replicate within macrophages → local spread → regional lymph node involvement
- Ghon focus = initial parenchymal focus (usually mid-lung zone)
- Ghon complex = Ghon focus + ipsilateral hilar lymphadenopathy
- Ranke complex = calcified Ghon focus + calcified hilar node (healed primary TB)
Immune Response & Granuloma Formation
- T-lymphocytes (CD4+) arrive ~3-8 weeks after infection
- Macrophages and T cells form granulomas - organized structures that wall off bacilli
- Granuloma center: caseous necrosis (cheese-like), surrounded by epithelioid macrophages, Langhans giant cells, lymphocytes, fibrous capsule
- Tuberculin skin test (TST) and IGRA become positive ~3-8 weeks post-infection
- In most immunocompetent hosts, granulomas contain infection → latent TB infection (LTBI)
Reactivation
- Latent bacilli can survive for decades within granulomas
- When immunity wanes (see risk factors above), granulomas break down → reactivation TB
- Typically involves upper lobes (high O₂ tension favors bacterial growth)
- Caseous material liquefies → cavity formation → aerosolization → transmission
4. Spectrum of TB Disease
| State | TST/IGRA | Culture | Smear | Infectious | Symptoms | Treatment |
|---|---|---|---|---|---|---|
| No infection | Negative | Negative | Negative | No | None | None |
| LTBI (early) | Positive | Negative | Negative | No | None | Preventive therapy |
| Subclinical TB | Positive | Intermittently + | Usually negative | Sporadically | Mild/none | Multi-drug therapy |
| Active TB | Usually positive | Positive | + or - | Yes | Mild to severe | Multi-drug therapy |
- Goldman-Cecil Medicine, p. 3252
5. Clinical Manifestations
Pulmonary TB (most common - ~85% of cases)
Symptoms (classic triad):
- Productive cough >3 weeks (most common; may be blood-stained → hemoptysis)
- Constitutional symptoms: fever (low-grade, often evening), night sweats, weight loss, anorexia, fatigue
- Chest pain (pleuritic if pleural involvement)
Signs:
- Often minimal early
- Dullness to percussion, bronchial breath sounds over consolidation
- Amphoric breathing over cavities
- Post-tussive crepitations in upper lobes
- Signs of pleural effusion if present
Radiographic patterns:
| Phase | CXR Finding |
|---|---|
| Primary TB | Mid/lower lung consolidation ± hilar lymphadenopathy (in children) |
| Latent/healed | Calcified Ghon/Ranke complex, calcified hilar nodes |
| Reactivation | Upper lobe infiltrates, fibronodular shadows, cavitation |
| Miliary TB | Diffuse 1-2mm nodules throughout both lungs ("millet seed" pattern) |
| Progressive primary | Lobar consolidation, large effusions |
Extrapulmonary TB
| Site | Clinical Features |
|---|---|
| Lymph nodes (most common extra-pulmonary) | Painless cervical/supraclavicular lymphadenopathy; nodes matted, may suppurate (scrofula) |
| Pleura | Pleuritic chest pain, serofibrinous effusion; lymphocyte-predominant exudate, ADA elevated |
| Spine (Pott disease) | Back pain, lower thoracic/upper lumbar vertebrae; anterior disc + two adjacent vertebrae involved; gibbus deformity, paravertebral abscess, spinal cord compression |
| CNS / Meningitis | Subacute meningitis with CSF: lymphocytes, high protein, low glucose; cranial nerve palsies; hydrocephalus; high mortality |
| Intestinal TB | Ileocaecal region most common; strictures, ulcers, malabsorption; mimics Crohn disease |
| Genitourinary | "Sterile pyuria" (WBC in urine, negative standard cultures); renal calcification; infertility |
| Pericardial | Constrictive pericarditis; pericardial effusion (lymphocytic exudate) |
| Miliary TB | Hematogenous dissemination; hepatosplenomegaly, choroidal tubercles, ARDS; very high mortality |
| Adrenal | Bilateral adrenal enlargement → Addison disease |
Immunologic/Hypersensitivity Manifestations
- Erythema nodosum - tender subcutaneous nodules (lower limbs)
- Erythema induratum (Bazin disease) - deeper vasculitic nodules, posterior calves
- Poncet disease - reactive arthritis + erythema nodosum
- TB-IRIS - immune reconstitution inflammatory syndrome (after starting ART in HIV-TB co-infection): paradoxical worsening; 5-50% incidence
6. Diagnostic Approach
Step 1: Suspect TB
- Cough >2-3 weeks + any constitutional symptoms, especially in:
- High-risk groups (HIV, immunosuppressed, contacts of known TB)
- Immigrants from high-burden countries
- Homeless, incarcerated populations
Step 2: Imaging
- Chest X-ray (PA view): first-line; upper lobe infiltrates/cavitation highly suggestive
- CT chest: more sensitive; detects early disease, miliary pattern, lymphadenopathy, cavities not visible on CXR
Step 3: Microbiological Confirmation
| Test | Specimen | Details |
|---|---|---|
| Sputum AFB smear (ZN or auramine) | 3 early morning samples | Fast (hours); sensitivity 50-80% in smear-positive; low sensitivity in HIV |
| Sputum culture (gold standard) | Sputum / BAL / tissue | Liquid media (MGIT): results in 1-6 weeks; solid (LJ): 4-8 weeks; enables DST |
| Xpert MTB/RIF (GeneXpert) | Sputum / CSF / tissue | WHO-endorsed; detects M. tuberculosis AND rifampicin resistance simultaneously within 2 hours; sensitivity ~88%, specificity ~99% |
| Xpert Ultra | Sputum | More sensitive than standard Xpert, especially in smear-negative/HIV disease |
| Drug susceptibility testing (DST) | Culture isolate | Phenotypic (MGIT) and/or molecular (line probe assay); mandatory for all patients |
| Line probe assay (LPA) | Smear-positive sputum | Rapid detection of INH/RIF resistance mutations within 1-2 days |
| Whole genome sequencing (WGS) | Culture / direct | Comprehensive resistance profiling; increasingly available |
For extrapulmonary TB:
- CSF: lymphocytosis, elevated protein, low glucose, ADA elevated; ZN smear low sensitivity; Xpert MTB/RIF recommended
- Pleural fluid: exudate, lymphocyte-predominant; ADA >40 U/L strongly suggestive; pleural biopsy has higher yield
- Lymph node: FNA (cytology + ZN stain + culture) or excision biopsy (caseating granulomas)
- Urine: early morning urine x3 for AFB culture in genitourinary TB
Step 4: Immunological Tests (for LTBI)
Tuberculin Skin Test (TST / Mantoux):
- Intradermal injection of 5 TU PPD; read at 48-72 hours
- Measure induration (not erythema)
| Induration Cutoff | Population |
|---|---|
| ≥5 mm | HIV-positive; recent close contacts; immunosuppressed; CXR with old TB changes |
| ≥10 mm | High-risk groups (immigrants, healthcare workers, prisoners, diabetes, renal failure) |
| ≥15 mm | Low-risk general population |
Limitations: False positives with BCG vaccination and non-tuberculous mycobacteria; false negatives in severe immunosuppression, recent infection (<8 weeks), miliary TB, sarcoidosis, malnutrition.
Interferon-Gamma Release Assay (IGRA):
- QuantiFERON-TB Gold Plus or T-SPOT.TB
- Detects IFN-γ release to ESAT-6 and CFP-10 antigens (specific to M. tuberculosis complex, absent from BCG and most NTM)
- Advantages over TST: Not affected by BCG, single visit, more specific
- Preferred in BCG-vaccinated individuals; not validated in children <5 years
- Results: Positive / Negative / Indeterminate
Note: Both TST and IGRA test for immunological response to M. tuberculosis antigens - they cannot distinguish LTBI from active disease. A positive TST/IGRA in someone with symptoms should prompt workup for active disease.
7. Treatment
A. Latent TB Infection (LTBI) - Preventive Therapy
All individuals with LTBI should be offered treatment after active TB is excluded.
| Regimen | Duration | Key Notes |
|---|---|---|
| 3HP - Rifapentine + Isoniazid weekly | 3 months (12 doses) | Preferred; strongly recommended; comparable efficacy to 9H; better completion; requires DOT or self-administration |
| 4R - Rifampicin daily | 4 months | Second preferred; HIV-negative adults; less hepatotoxic than INH; beware drug interactions |
| 3RH - Rifampicin + Isoniazid daily | 3 months | Third preferred; comparable to 6H |
| 6H - Isoniazid daily | 6 months | Alternative; effective; add pyridoxine 25-50 mg/day to prevent neuropathy |
| 9H - Isoniazid daily | 9 months | Alternative; highest efficacy; most hepatotoxicity |
In HIV-positive persons in high TB burden areas, 6 months of daily INH is complementary to ART regardless of IGRA result. - Goldman-Cecil, p. 3259
B. Active Pulmonary TB (Drug-Susceptible)
Standard 6-month regimen:
| Phase | Drugs | Duration | Acronym |
|---|---|---|---|
| Intensive phase | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2 months | 2HRZE |
| Continuation phase | Isoniazid (H) + Rifampicin (R) | 4 months | 4HR |
Daily doses (adults):
| Drug | Dose | Key Side Effects | Monitoring |
|---|---|---|---|
| Isoniazid (H) | 5 mg/kg (max 300 mg) daily | Hepatotoxicity, peripheral neuropathy (add B6/pyridoxine), lupus-like reaction | LFTs if risk factors; pyridoxine 25-50 mg/day |
| Rifampicin (R) | 10 mg/kg (max 600 mg) daily | Hepatotoxicity, orange discolouration of secretions, drug interactions (CYP3A4 inducer), thrombocytopenia | LFTs; warn about discolouration |
| Pyrazinamide (Z) | 25 mg/kg (max 2g) daily | Hepatotoxicity, hyperuricaemia, arthralgia, gout | LFTs, uric acid |
| Ethambutol (E) | 15-20 mg/kg daily | Optic neuritis (visual acuity, colour vision) - dose-dependent | Monthly visual acuity and colour vision testing; avoid in young children unable to report visual changes |
Extension of therapy:
- 7-10 month continuation phase (total 9 months) for: cavitary disease with positive culture at 2 months, TB meningitis, bone/joint/spine TB, HIV-positive not on ART
- HIV on ART: Standard 6-month regimen effective; use daily dosing (not intermittent)
Directly Observed Therapy (DOT):
- WHO-recommended strategy where a health worker watches each dose being taken
- Improves adherence and treatment completion; detects adverse events early
- Especially important in resource-limited settings and for drug-resistant TB
C. Extrapulmonary TB Treatment Duration
| Site | Duration |
|---|---|
| Lymph node, pleural | 6 months (standard) |
| Bone/joint/spine (Pott) | 9-12 months |
| CNS (meningitis) | 9-12 months + corticosteroids (dexamethasone) |
| Pericardial | 6 months + corticosteroids |
| Miliary | 6-9 months |
Corticosteroids are recommended adjunctive therapy for TB meningitis and pericarditis (reduce mortality and neurological sequelae).
D. Drug-Resistant Tuberculosis
Definitions:
| Type | Definition |
|---|---|
| Mono-resistance | Resistant to one first-line drug |
| Poly-resistance | Resistant to >1 first-line drug (not INH + RIF together) |
| MDR-TB | Resistant to at least INH + RIF |
| Pre-XDR-TB | MDR-TB + resistance to any fluoroquinolone |
| XDR-TB | MDR-TB + resistance to a fluoroquinolone + bedaquiline or linezolid |
INH mono-resistance: Replace INH with moxifloxacin (400 mg) or levofloxacin (750 mg) → 6 months of R + E + Z + fluoroquinolone.
MDR-TB Treatment - BPaLM regimen (current WHO-preferred):
- B - Bedaquiline
- Pa - Pretomanid
- L - Linezolid
- M - Moxifloxacin (if susceptible)
- Duration: 6 months
A 2025 systematic review (PMID: 39813501) confirms BPaLM as effective for MDR/RR-TB with acceptable safety profile.
Rifampin mono-resistance can also be treated successfully with oral antibiotics (treat as MDR-TB until DST clarifies).
8. HIV-TB Co-infection
- HIV is the single most important risk factor for TB reactivation
- TB is the leading cause of death in people living with HIV worldwide
- All HIV patients should be screened for TB; all TB patients should be tested for HIV
Management principles:
- Start TB treatment first (before ART in most cases)
- Start ART within 2-8 weeks of TB treatment (earlier for severe immunosuppression CD4 <50)
- Drug interactions: Rifamycins are potent CYP3A4 inducers → reduce levels of many ARTs
- Rifampicin + efavirenz: no dose adjustment
- Rifampicin + dolutegravir: double dolutegravir dose (50 mg BD)
- Rifabutin (fewer interactions) preferred with ritonavir-boosted protease inhibitors (half-dose rifabutin)
- Avoid tenofovir alafenamide with rifamycins
- TB-IRIS: Watch for paradoxical worsening (fever, lymphadenopathy) after starting ART; treat with NSAIDs or corticosteroids if severe
- Continuation phase extended to 7 months (total 9 months) if not on ART at start of TB treatment
9. Drug Monitoring & Adverse Effects
| Situation | Action |
|---|---|
| Hepatotoxicity (ALT >3x ULN with symptoms or >5x ULN) | Stop hepatotoxic drugs (INH, RIF, PZA); restart sequentially when LFTs normalise |
| Peripheral neuropathy (INH) | Add/increase pyridoxine; consider dose reduction |
| Visual changes (Ethambutol) | Stop ethambutol immediately; ophthalmology review |
| Orange secretions (Rifampicin) | Reassure patient - harmless but warn contacts |
| Hyperuricaemia/gout (PZA) | Uric acid monitoring; allopurinol if symptomatic |
| Severe skin reaction | Stop all drugs; restart one at a time |
Renal failure dosing adjustments (CrCl <30 mL/min or hemodialysis):
- INH: 300 mg OD or 900 mg 3x/week
- RIF: 600 mg OD (no change)
- PZA: 25-35 mg/kg 3x/week (after dialysis)
- EMB: 20-25 mg/kg 3x/week (after dialysis)
10. Prevention & Public Health
| Intervention | Details |
|---|---|
| BCG vaccine | Protects against severe childhood TB (miliary, meningitis); less effective for pulmonary TB in adults; given at birth in high-burden countries |
| Infection control | Airborne precautions (N95 mask, negative-pressure room), natural ventilation, UV germicidal irradiation |
| Contact tracing | All close contacts of smear-positive index case; test with TST/IGRA; offer LTBI treatment if positive |
| LTBI treatment | See above - treat all with positive IGRA/TST after excluding active disease |
| Notification | TB is a notifiable disease in most countries; mandatory public health reporting |
Infectiousness & Isolation:
- Patients with pulmonary TB are considered infectious until:
- 2 weeks of effective treatment, AND
- Clinical improvement, AND
- 3 consecutive negative sputum smears (some guidelines require negative cultures)
- Smear-negative pulmonary TB is still potentially infectious (lower risk)
11. Special Populations
Children
- More likely to develop primary progressive TB and extrapulmonary disease (especially miliary TB and meningitis)
- TST preferred; IGRA not validated <5 years
- Avoid ethambutol in young children unable to report visual symptoms
Pregnancy
- TB must be treated - risk of untreated TB to mother and fetus far exceeds drug risks
- 2HRZE/4HR is used; pyridoxine supplementation essential
- Streptomycin is contraindicated (ototoxicity to fetus)
Long-Term Outcomes
- A 2025 systematic review in Lancet Global Health (PMID: 40412395) found that post-TB lung function impairment is common even after successful treatment, with significant long-term morbidity including obstructive and restrictive patterns.
Key Sources:
- Goldman-Cecil Medicine (International Edition), Chapter 299 - Tuberculosis, pp. 3246-3262
- Fishman's Pulmonary Diseases and Disorders, CAP & TB sections
- Murray & Nadel's Textbook of Respiratory Medicine
- WHO Guidelines for Treatment of Drug-Susceptible and Drug-Resistant TB (2022)
This is a shared conversation. Sign in to Orris to start your own chat.