Sexual dysfunction and Infertility (male and female): 1.Order and interpret relevant investigations of Sexual dysfunction and Infertility 2. Describe differential diagnosis of Sexual dysfunction and Infertility Notes on male and female infertility including these points
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from the textbooks. Let me compile the full structured notes.
Sexual Dysfunction and Infertility: Clinical Notes
Part 1 - Sexual Dysfunction
Definition and Classification
Sexual functioning involves interactions among the physical, mental, and emotional aspects of an individual. The DSM-5 framework is used to classify sexual dysfunctions. To qualify as a "disorder," the condition must cause clinically significant distress. If an individual's sexual response is outside statistical norms but causes no distress, it is not classified as a disorder.
DSM-5 subtypes describe:
- Lifelong vs. Acquired onset
- Generalized vs. Situational (only with specific stimulation, partner, or context)
- Severity: Mild / Moderate / Severe (based on distress)
Factors to Consider in Evaluation
Before diagnosing sexual dysfunction, the clinician must evaluate:
- Partner factors - partner's sexual response or level of involvement
- Relationship factors - communication quality, emotional abuse
- Individual vulnerability - body image, psychiatric comorbidity (depression, anxiety), life stressors (unemployment)
- Cultural or religious factors
- Medical factors - physical disability, medications
Rule out that the dysfunction is not better explained by a non-sexual mental health disorder or by a medication/substance effect.
Female Sexual Dysfunction
Types (DSM-5)
1. Female Sexual Interest/Arousal Disorder (FSIAD)
Low sexual desire is the most common female sexual problem - 4 in 10 women report it.
| Diagnostic Criteria (at least 3 of 6 for ≥6 months) |
|---|
| Absent or reduced interest in sexual activity |
| Absent or reduced sexual/erotic thoughts or fantasies |
| No or reduced initiation; unreceptive to partner's attempts |
| Absent or reduced excitement/pleasure during activity |
| Absent or reduced interest in response to sexual/erotic cues |
| Absent or reduced genital or nongenital sensations during activity |
DSM-5 recognizes the interaction between desire and arousal as the trigger for a woman's sexual response.
2. Female Orgasmic Disorder
Difficulty or inability to achieve orgasm despite adequate stimulation.
3. Genito-Pelvic Pain/Penetration Disorder (GPPPD)
Prevalence: 12-21% in the United States. Presents as:
- Pain/difficulty with vaginal penetration (intercourse, digital stimulation, tampons, pelvic exam)
- Visible pelvic floor muscle contraction on anticipated speculum exam
- Anatomic abnormalities may be found (vaginal septa)
History clue: Pain on tampon insertion before sexual activity may be an early risk factor.
Investigations for Female Sexual Dysfunction
- Detailed psychosexual and medical history
- Physical examination - genitalia, pelvic floor muscle assessment
- Hormonal panel: FSH, LH, estradiol, prolactin, TSH, testosterone (especially in peri/postmenopausal women or those with low desire)
- Pelvic examination to exclude structural/infective causes
- Psychological screening: PHQ-9 (depression), GAD-7 (anxiety)
Differential Diagnosis - Female Sexual Dysfunction
| Condition | Key Feature |
|---|---|
| Hypothyroidism/hyperthyroidism | Low libido, fatigue, anovulation |
| Hyperprolactinemia | Low desire, galactorrhea, amenorrhea |
| Hypogonadism (estrogen deficiency) | Vaginal atrophy, dyspareunia, low libido |
| Depression | Global loss of desire, anhedonia |
| PTSD/sexual trauma | Situational pain/avoidance |
| Relationship dysfunction | Situational, partner-specific |
| Medication-induced (SSRIs) | Delayed or absent orgasm, low desire |
| Vaginitis / pelvic infection | Dyspareunia, discharge |
| Endometriosis | Deep dyspareunia, cyclical pain |
| Pelvic floor dysfunction / vaginismus | Penetration pain/spasm |
SSRIs delay or inhibit orgasm in women - an important medication side effect to recognize.
Male Sexual Dysfunction
Erectile Dysfunction (ED)
Definition: Inability for a male to achieve a penile erection sufficient for sexual function. DSM-5 requires clinically significant distress not explained by another mental health disorder or substance.
Physiology of Erection:
- Parasympathetic stimulation → nitric oxide (NO) release from noradrenergic, noncholinergic nerves and endothelial cells
- NO → increases intracellular cGMP → cavernosal smooth muscle relaxation → rapid blood flow → emissary vein occlusion → erection
- PDE-5 catalyzes cGMP breakdown; PDE-5 inhibitors (e.g., sildenafil) increase cGMP
- Four systems required: vascular, neurologic, endocrine, psychological
Prevalence increases with age:
- Ages 40-49: 2%
- Ages 50-59: 6%
- Ages 60-69: 17%
- Age ≥70: 39%
Investigations for ED
History (similar to cardiovascular risk assessment - "what is bad for the heart is bad for the penis"):
- Cardiovascular risk factors (diabetes, hypertension, dyslipidemia, smoking)
- Medication review (see table below)
- Psychosocial: depression, anxiety, relationship issues, alcohol, recreational drugs
- Neurologic symptoms, endocrine symptoms (hypogonadism signs)
Physical Examination:
- Peripheral pulses and carotid bruits (vascular)
- Thyroid examination
- Genitourinary exam - Peyronie's plaques, testicular atrophy
- Neurologic: anal sphincter tone, perianal sensation, bulbocavernosus reflex
- Signs of hypogonadism (reduced secondary sexual characteristics)
Laboratory Tests:
| Investigation | Reason |
|---|---|
| Fasting glucose | Diabetes screening |
| Fasting lipid profile | Vascular risk |
| BUN + Creatinine | Renal disease |
| LFTs (transaminases) | Hepatic disease |
| TSH | Thyroid dysfunction |
| Total testosterone | Hypogonadism (especially if young or signs present) |
| Free testosterone | If total T borderline - only ~2% of T is free/bioavailable |
| Prolactin | If low T found, to exclude hyperprolactinemia |
| PSA | If prostate symptoms |
Note: Low testosterone is present in only ~7% of men with ED. A low level alone is not definitive causation.
Medications Causing Sexual Dysfunction
| Drug Class | Examples |
|---|---|
| Antihypertensives | Beta-blockers, thiazides, clonidine, methyldopa, CCBs, ACE inhibitors |
| Antipsychotics | Multiple agents |
| Antidepressants | TCAs, SSRIs |
| Anxiolytics | Alprazolam, diazepam |
| Antiandrogens | Ketoconazole, spironolactone |
| 5-alpha reductase inhibitors | Finasteride, dutasteride |
| GnRH agonists | Leuprolide, buserelin |
| H2-blockers | Cimetidine |
| Opioids | Multiple |
| Statins | Atorvastatin, pravastatin, simvastatin |
| Digoxin, fibrates, cytotoxic agents | Methotrexate |
Differential Diagnosis - Male Sexual Dysfunction
| Diagnosis | Features |
|---|---|
| Psychogenic ED | Situational, nocturnal erections preserved |
| Vascular ED | Age-related, cardiovascular risk factors, no nocturnal erections |
| Neurogenic ED | Spinal cord injury, MS, diabetic neuropathy, pelvic surgery |
| Endocrine ED | Hypogonadism, hyperprolactinemia, thyroid disease |
| Drug-induced | Onset correlates with medication change |
| Peyronie's disease | Pain/curvature during erection, fibrous plaque |
| Depression/anxiety | Psychological overlay, global reduced desire |
| Premature ejaculation | <1 minute intravaginal ejaculatory latency (distinct from ED) |
Part 2 - Infertility
Definition: Failure to achieve pregnancy after 1 year of unprotected intercourse (evaluate sooner in women >35, history of pelvic disease, or known risk factors).
Distribution of causes:
- 1/3 male factors alone
- 1/3 female factors alone
- 1/3 combination
- ~20% unexplained (idiopathic)
Male Infertility
Causes (Classification)
Endocrine Disorders:
- Hypothalamic dysfunction (Kallmann syndrome - GnRH deficiency + anosmia)
- Pituitary failure (tumor, radiation, surgery)
- Hyperprolactinemia (drugs, prolactinoma) - impairs GnRH release → hypogonadism → low T + ED
- Androgen insensitivity syndrome (AIS)
- Exogenous androgens (anabolic steroid abuse)
- Thyroid disorders (both hyper- and hypothyroidism impair spermatogenesis)
- Adrenal hyperplasia
- Testicular failure
Anatomic Disorders:
- Congenital absence of vas deferens (associated with CFTR mutations - cystic fibrosis)
- Obstructed vas deferens
- Congenital ejaculatory system abnormalities
- Varicocele (most common identifiable cause, 15-35%)
- Retrograde ejaculation
Abnormal Spermatogenesis:
- Chromosomal abnormalities (e.g., Klinefelter syndrome 47,XXY)
- Y chromosome microdeletions
- Mumps orchitis
- Cryptorchidism (undescended testis)
- Chemical/radiation exposure
Abnormal Motility:
- Kartagener syndrome (absent dynein arms → immotile cilia)
- Antisperm antibody formation
Psychosocial:
- Unexplained impotence
- Decreased libido
Differential Diagnosis - Male Infertility
| Diagnostic Category | Incidence (%) |
|---|---|
| Idiopathic infertility | 50-60% |
| Varicocele | 15-35% |
| Primary testicular failure (Klinefelter, Y microdeletions, cryptorchidism, irradiation, orchitis, drugs) | 10-20% |
| Genital tract obstruction (congenital absence of vas, vasectomy, epididymal obstruction) | ~5% |
| Hypogonadotropic hypogonadism (pituitary adenoma, panhypopituitarism, idiopathic HH, hyperprolactinemia) | 3-4% |
| Other (sperm autoimmunity, drugs, toxins, systemic illness) | ~5% |
| Coital disorders | <1% |
(From Williams' Textbook of Endocrinology, via Textbook of Family Medicine 9e)
Investigations for Male Infertility
History focuses on:
- Reproductive history (previous pregnancies, miscarriages)
- Prescribed and recreational medications (including anabolic steroids, alcohol)
- Systemic illness
- Toxin and radiation exposure
- Sexual history: technique, frequency, lubricants
- STI history
- Family history of genetic diseases
Physical Examination:
- External genitalia - androgenization
- Hair pattern - virilization
- Breasts - gynecomastia
- Neurologic - sense of smell (Kallmann), visual fields (pituitary mass)
- Testicular volume and consistency
Step 1 - Semen Analysis (most important single test):
| Parameter | Normal Value (WHO) |
|---|---|
| Ejaculate volume | >1.5 mL |
| Sperm density | >15 million/mL |
| Total sperm count | >39 million/ejaculate |
| Progressive motility | >32% |
| Total motility | >40% |
| Morphology (Kruger strict) | >4% normal forms |
| pH | 7.2-8.0 |
| Liquefaction | Within 40 minutes |
| Fructose | >1200 μg/mL |
(Tietz Textbook of Laboratory Medicine, 7th ed.)
Semen should be analyzed within 1 hour of collection. If abnormal, repeat in 6 weeks before proceeding further.
Step 2 - Endocrine Evaluation (if oligospermia/azoospermia confirmed):
| Hormone | Interpretation |
|---|---|
| ↓LH, ↓FSH, ↓Testosterone | Hypothalamic or pituitary failure (hypogonadotropic hypogonadism) |
| ↑LH, ↑FSH, ↓Testosterone | Primary gonadal failure (hypergonadotropic hypogonadism) |
| Normal LH, ↑FSH, Normal T | Germinal compartment failure (spermatogenic failure) |
| ↑LH, Normal FSH, Normal/↑T | Androgen resistance |
| Normal LH, FSH, T | Idiopathic |
| Elevated Prolactin | Hyperprolactinemia - check TRH/hypothyroid as cause |
Step 3 - Additional Tests:
- Genetic testing: Karyotype (Klinefelter), Y chromosome microdeletion analysis
- Testicular biopsy: If azoospermic with normal FSH (to distinguish obstruction from spermatogenic failure)
- Scrotal ultrasound: For varicocele assessment
- CFTR mutation analysis: If congenital bilateral absence of vas deferens (CBAVD)
- hCG stimulation test: 5000 IU IM → measure testosterone at 72h. Doubling indicates normal Leydig cell function. Failure to rise >150 ng/dL = primary hypogonadism
- Seminal biochemical markers: Absence of fructose/prostaglandins (seminal vesicle block); low acid phosphatase/citric acid (prostatic obstruction); low glucosidase (epididymal obstruction or CBAVD)
Male Infertility Evaluation Algorithm
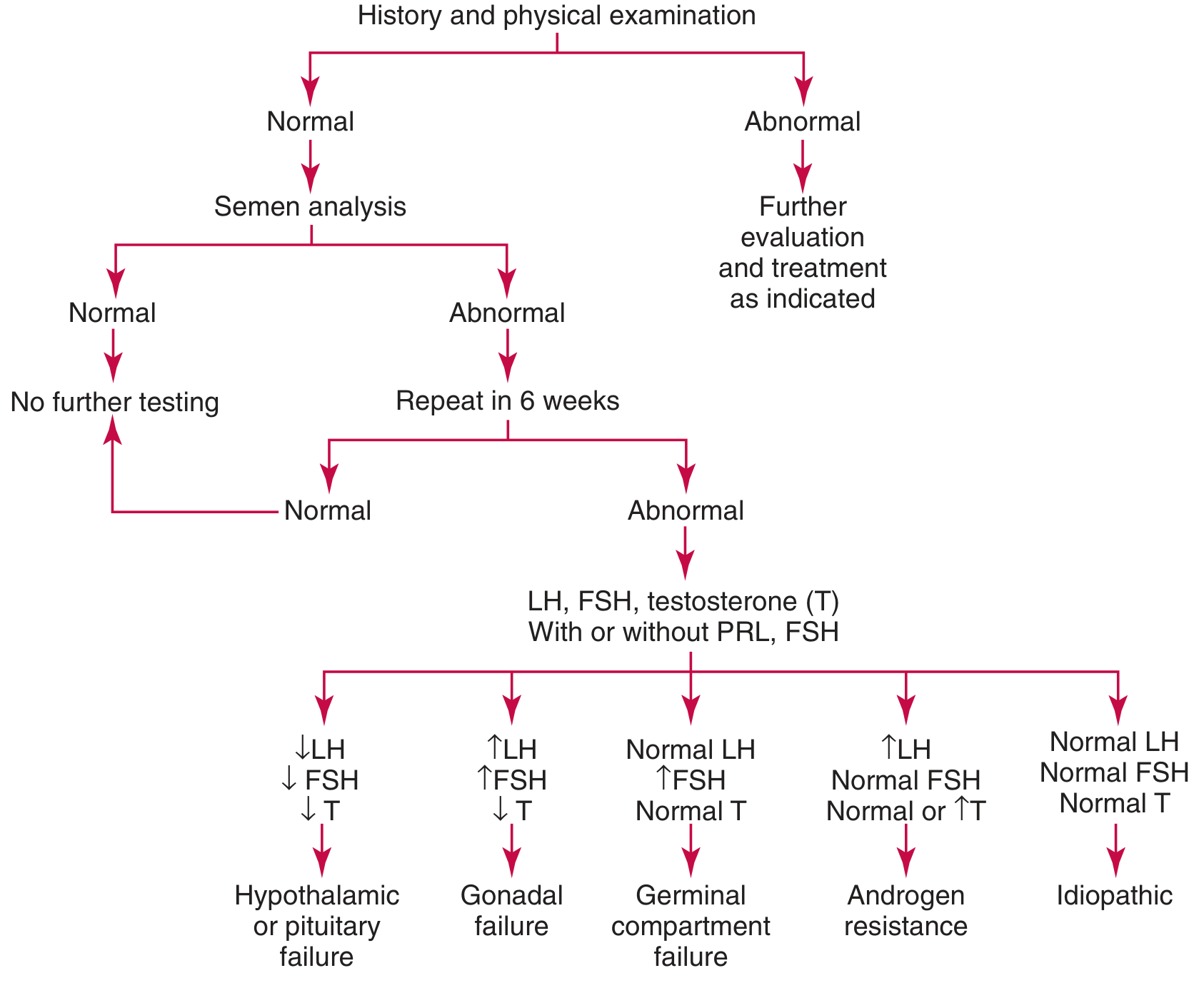
Starting with history and physical exam → semen analysis → if abnormal, repeat in 6 weeks → if still abnormal → LH, FSH, Testosterone (± Prolactin, TSH) → interpretation leads to: hypothalamic/pituitary failure, gonadal failure, germinal compartment failure, androgen resistance, or idiopathic.
Female Infertility
Epidemiology
- 15-20% of all couples are infertile
- Fertility peaks at ages 20-24, declines progressively after 32, steep decline after 40
- Evaluate at 1 year unprotected intercourse; sooner if age >35, irregular menses, history of PID/STI, or gonadotoxin exposure
Causes (Classification)
Ovarian/Hormonal Factors (40%):
- Polycystic ovary syndrome (PCOS) - single most common endocrine abnormality in reproductive-age women
- Hypergonadotropic hypogonadism (primary ovarian insufficiency, menopause, gonadal dysgenesis)
- Hypogonadotropic hypogonadism (Kallmann syndrome, pituitary insufficiency from tumor/necrosis/thrombosis/stress/exercise/anorexia)
- Hyperprolactinemia (drugs, prolactinoma)
- Luteal phase deficiency
- Metabolic disease (thyroid, liver, obesity, adrenal hyperplasia with androgen excess)
- Resistant ovary syndrome
Tubal Factors (20%):
- Tubal occlusion or scarring (post-PID, post-surgery)
- Salpingitis isthmica nodosa
- Infectious salpingitis
Cervical Factors:
- Stenosis
- Inflammation/infection
- Abnormal mucus viscosity
Uterine Factors:
- Leiomyomata (fibroids)
- Congenital malformations (Müllerian defects)
- Intrauterine adhesions (Asherman syndrome)
- Endometritis/abnormal endometrium
Peritoneal/Other Factors:
- Endometriosis
- Pelvic adhesions
Psychosocial:
- Decreased libido
- Anorgasmia
Immunologic:
- Antisperm antibodies
Differential Diagnosis - Female Infertility
| Diagnosis | Key Features |
|---|---|
| PCOS | Oligomenorrhea, hyperandrogenism, polycystic ovaries on USS |
| Primary ovarian insufficiency | FSH >25 IU/L before age 40, amenorrhea |
| Hypothyroidism | Weight gain, fatigue, low TSH, anovulation |
| Hyperprolactinemia | Galactorrhea, amenorrhea, elevated prolactin |
| Hypogonadotropic hypogonadism | Low FSH/LH, low estrogen, anosmia (Kallmann) |
| Endometriosis | Dysmenorrhea, deep dyspareunia, raised CA-125 |
| Tubal factor (post-PID) | History of STI/PID, abnormal HSG |
| Asherman syndrome | Prior uterine instrumentation, oligomenorrhea |
| Uterine fibroids | Menorrhagia, pelvic pressure, uterine enlargement |
| Luteal phase defect | Low midluteal progesterone |
| Unexplained infertility | All tests normal (~20% of couples) |
Investigations for Female Infertility
Step 1 - Assessment of Ovulation
| Method | Details |
|---|---|
| Urinary LH kit (OPK) | Detects LH surge 24-36h before ovulation; guides timing of intercourse |
| Midluteal serum progesterone | Checked day 21-23 (7 days before expected menses). >300 ng/dL (9.5 nmol/L) confirms ovulation |
| Basal body temperature | Temperature rises 0.2-0.5°F at ovulation (due to progesterone). Only retrospective; no longer recommended routinely |
| Transvaginal ultrasound | Confirms follicular development and collapse |
Note: No test confirms actual ovum release; progesterone confirms corpus luteum formation only.
Step 2 - Ovarian Reserve Testing
| Test | Indication / Interpretation |
|---|---|
| Day 3 FSH | >12 IU/L = poor ovarian response; women >35 should be checked; referral to reproductive endocrinologist if elevated |
| Day 3 Estradiol (E2) | Elevated E2 despite normal FSH = poor reserve |
| Anti-Müllerian hormone (AMH) | Best marker of ovarian reserve; low = diminished reserve |
| Antral follicle count (USS) | <5-7 follicles = diminished reserve |
Step 3 - Hormonal Panel (if menses absent, irregular, or signs of galactorrhea/thyroid disease)
| Hormone | Purpose |
|---|---|
| TSH | Thyroid disease causing anovulation |
| Prolactin | Hyperprolactinemia; if elevated, check for hypothyroidism (elevated TRH → elevated PRL) |
| Testosterone | Androgen excess (PCOS, adrenal hyperplasia) |
| FSH + LH | Ovarian vs. central hypogonadism; progestin challenge if amenorrhoeic |
| Estradiol | Ovarian function |
| DHEAS, 17-OHP | Adrenal hyperplasia workup |
Step 4 - Assessment of Tubal Patency and Uterine Anatomy
| Test | Details |
|---|---|
| Hysterosalpingography (HSG) | First choice for tubal patency; outlines uterine cavity and tubal architecture |
| Laparoscopy + chromotubation | Gold standard; used if HSG abnormal or strong clinical suspicion of tubal disease |
| Transvaginal ultrasound | Ovarian pathology, fibroids |
| Sonohysterography | Submucosal myomas and endometrial polyps |
| Hysteroscopy | Direct visualization; therapeutic as well as diagnostic |
| MRI | Complex Müllerian anomalies |
| Laparoscopy | Peritoneal factors (endometriosis, adhesions) |
Tests no longer recommended as routine:
- Postcoital test (not sensitive)
- Endometrial biopsy
- Basal body temperature charts as routine initial test
Summary Table - Investigations for Female Infertility
| Category | Tests |
|---|---|
| Ovulatory factors | Urinary LH kit; midluteal progesterone; transvaginal USS; TSH, FSH, PRL, androgens |
| Cervical factors | Cervical mucus evaluation; postcoital test (low sensitivity, no longer routine) |
| Uterine factors | USS; HSG; hysteroscopy; sonohysterography; MRI |
| Tubal factors | HSG (first choice); laparoscopy + chromotubation; fluoroscopic or hysteroscopic tubal cannulation |
| Peritoneal factors | USS; laparoscopy |
(Modified from Brassard et al., Med Clin North Am 2008; via Textbook of Family Medicine 9e)
Female Infertility Evaluation Algorithm
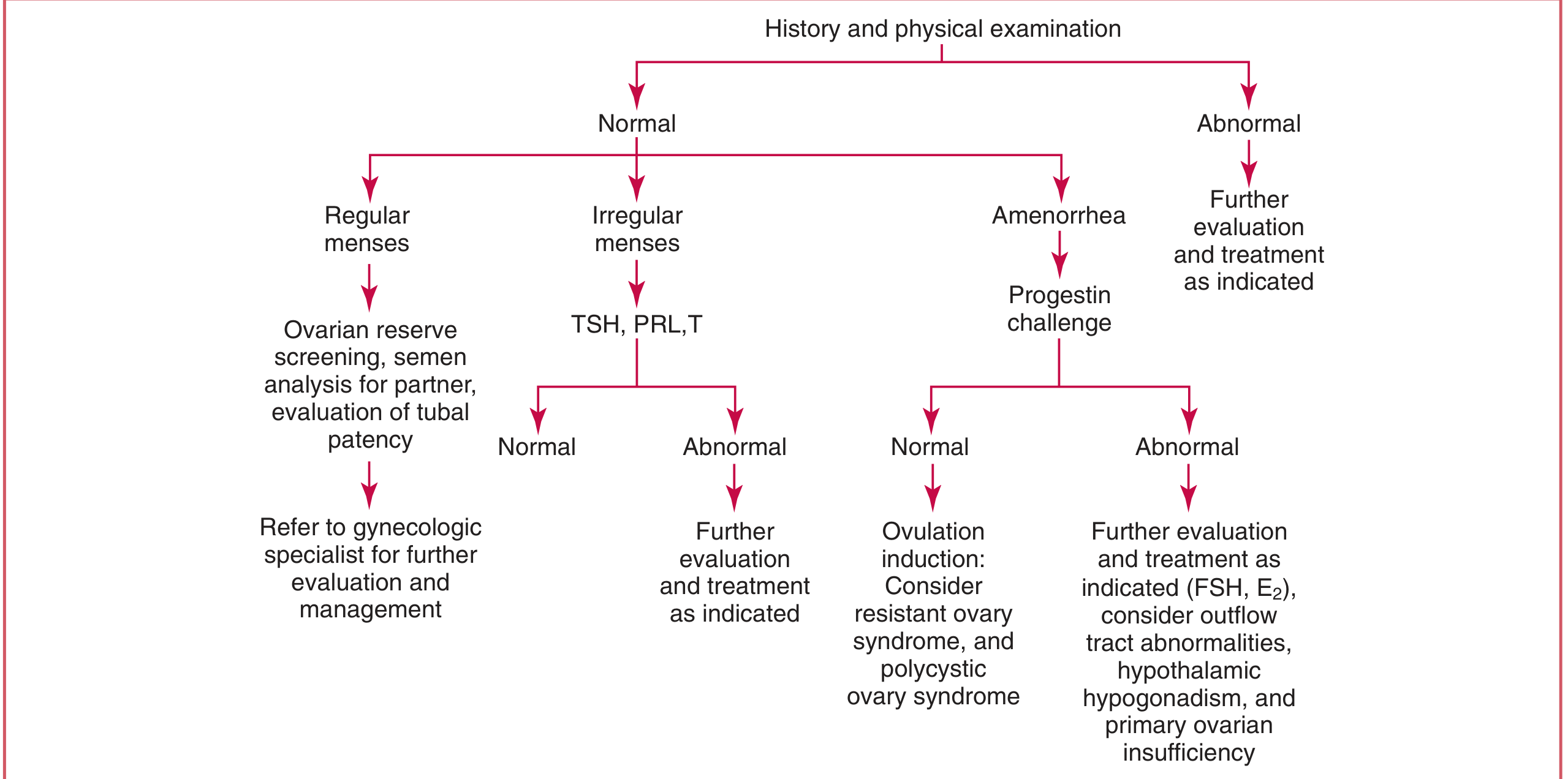
Starting with history and physical exam → if normal: branch by menstrual pattern (regular/irregular/amenorrhea) → regular menses: ovarian reserve screen, partner semen analysis, tubal patency evaluation → irregular menses: TSH, PRL, T → amenorrhea: progestin challenge → guides toward diagnosis and treatment
Management Overview
Male Infertility
- Infection: targeted antibiotics
- Varicocele: varicocelectomy
- Hypogonadotropic HH: pulsatile GnRH or exogenous gonadotropins (FSH + hCG)
- Hyperprolactinemia: dopamine agonists (cabergoline, bromocriptine)
- Obstruction: surgical correction or sperm retrieval + IVF/ICSI
- Idiopathic/severe oligospermia: intrauterine insemination (IUI) or assisted reproductive technology (ART/IVF/ICSI)
- Exogenous androgens: cessation and allow recovery
Female Infertility
- Anovulation (PCOS): clomiphene citrate, metformin (if insulin resistant)
- Hyperprolactinemia: bromocriptine
- Hypothyroidism: levothyroxine
- Hypogonadotropic HH: pulsatile GnRH or exogenous FSH + LH
- Adrenal hyperplasia with androgen excess: glucocorticoids + clomiphene
- Tubal factor: surgical repair or IVF
- Endometriosis: laparoscopic ablation ± IVF
- Uterine factors: hysteroscopic correction (fibroids, polyps, adhesions)
- Unexplained: empirical clomiphene, IUI, or IVF
Sources
- Textbook of Family Medicine, 9th ed. (pp. 1044-1052, 1261)
- Tietz Textbook of Laboratory Medicine, 7th ed. (pp. 2378-2382, 2807-2826)
- DSM-5 framework (as cited in Family Medicine and Neurology texts)
This is a shared conversation. Sign in to Orris to start your own chat.