Sinus bradycardia under evaluation
Reading File
Finding Sources
Searching PubMed
"sinus bradycardia" AND evaluation
Searching the Web
sinus bradycardia evaluation diagnosis management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks plus the diagnostic algorithm and ECG images. Here is the full, structured response:
Sinus Bradycardia: Evaluation
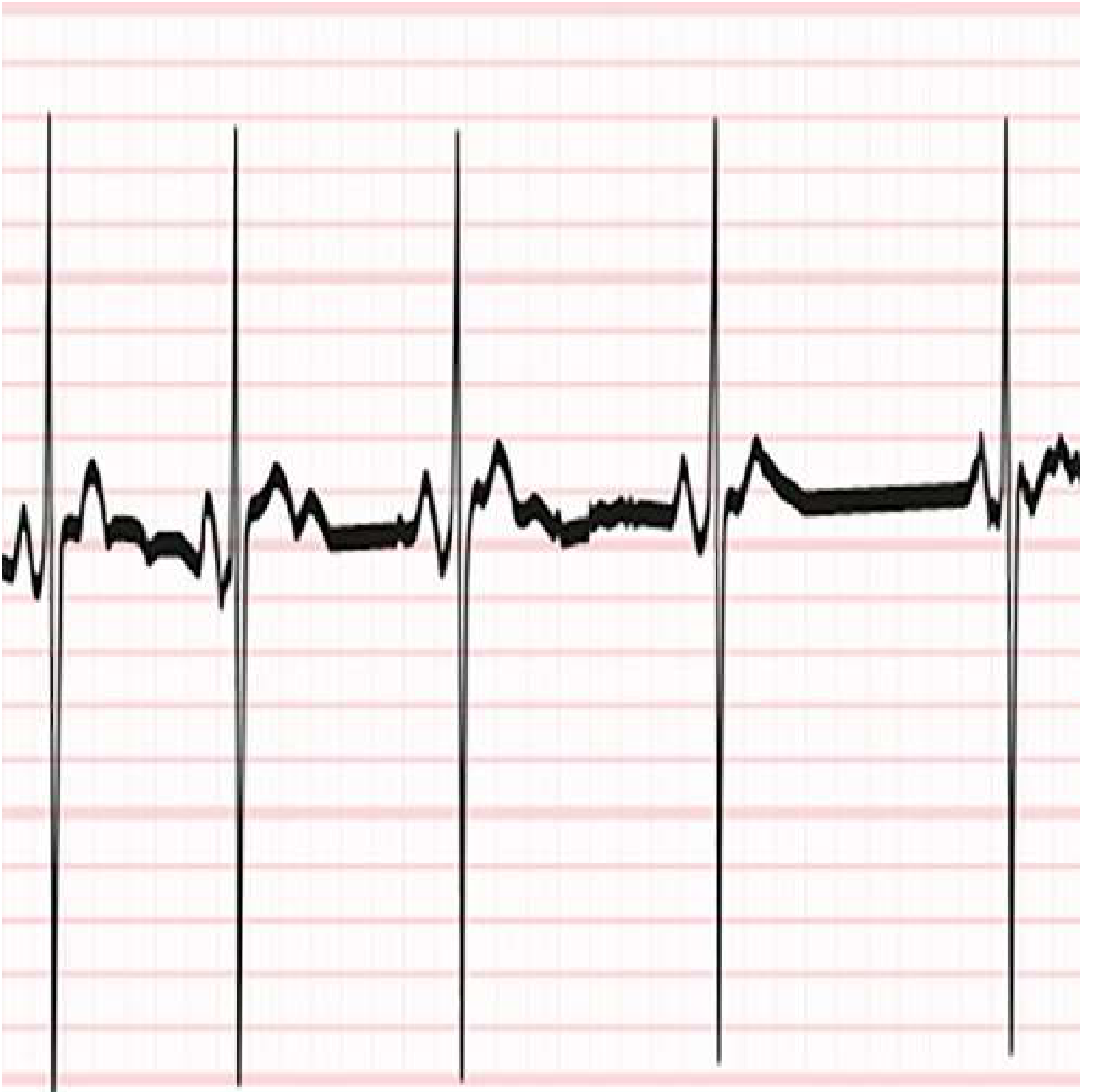
Definition & ECG Recognition
Sinus bradycardia is a cardiac rhythm originating from the sinoatrial (SA) node at a rate below 60 bpm. Braunwald's Heart Disease uses a threshold of <50 bpm in adults for diagnostic purposes; Goldman-Cecil and clinical practice generally use <60 bpm, with rates of 45-50 bpm at rest considered physiologically normal.
ECG criteria:
- Normal P wave morphology (upright in leads I, II, aVF)
- Fixed P-P interval = R-R interval
- P wave precedes every QRS complex
- PR interval >120 ms (constant)
- Sinus arrhythmia may coexist
ECG example - progressive sinus bradycardia due to heightened vagal tone during sleep (Goldman-Cecil Medicine):
Physiologic vs. Pathologic
| Context | Interpretation |
|---|---|
| Well-conditioned athlete, resting | Physiologic (high vagal tone) |
| Young adults during sleep | Physiologic |
| Rate <40 bpm | Junctional escape rhythm may emerge |
| Symptomatic (syncope, presyncope, fatigue, HF worsening) | Pathologic - requires workup |
Causes
Medical Conditions (Harrison's 22E, 2025)
- Hypothyroidism
- Sleep apnea
- Hypoxia
- Hypothermia
- Increased intracranial pressure
- Lyme disease
- Myocarditis
- COVID-19
- Vagal reflex (cough, pain, hemoperitoneum, inferior wall MI)
- Carotid sinus hypersensitivity / vasovagal syncope
- Intrinsic sinus node disease (sick sinus syndrome - age-related fibrosis)
- Post-cardiac surgery / heart transplantation
- Spinal cord injury (autonomic dysreflexia)
Medications (Goldman-Cecil Medicine / Harrison's 22E)
Cardiac drugs:
- Beta-blockers (including ophthalmic beta-blocker eye drops)
- Non-dihydropyridine calcium channel blockers (diltiazem, verapamil)
- Digoxin, ivabradine
Antiarrhythmics:
- Amiodarone, dronedarone, sotalol, flecainide, propafenone
Psychoactive / other:
- SSRIs, tricyclic antidepressants, lithium
- Opioid analgesics
- Phenothiazines (antiemetics / antipsychotics)
- Phenytoin
- Cholinesterase inhibitors (donepezil)
- Cannabis
- Clonidine, methyldopa, propofol, remdesivir
Evaluation
History & Physical (most important first step)
- Symptom correlation: fatigue, dizziness, near-syncope/syncope, exertional intolerance, worsening heart failure
- Medication review (above list)
- Contextual factors: athletic training, sleep state, acute illness
Initial Testing
- 12-lead ECG - confirm sinus bradycardia, look for AV block, ischemic changes
- Basic labs: TSH (hypothyroidism), electrolytes (hyperkalemia), Lyme serology if appropriate, troponin if ischemia suspected, toxicology if drug ingestion suspected
ACC/AHA/HRS Evaluation Algorithm (FIGURE 251-3, Harrison's 22E)
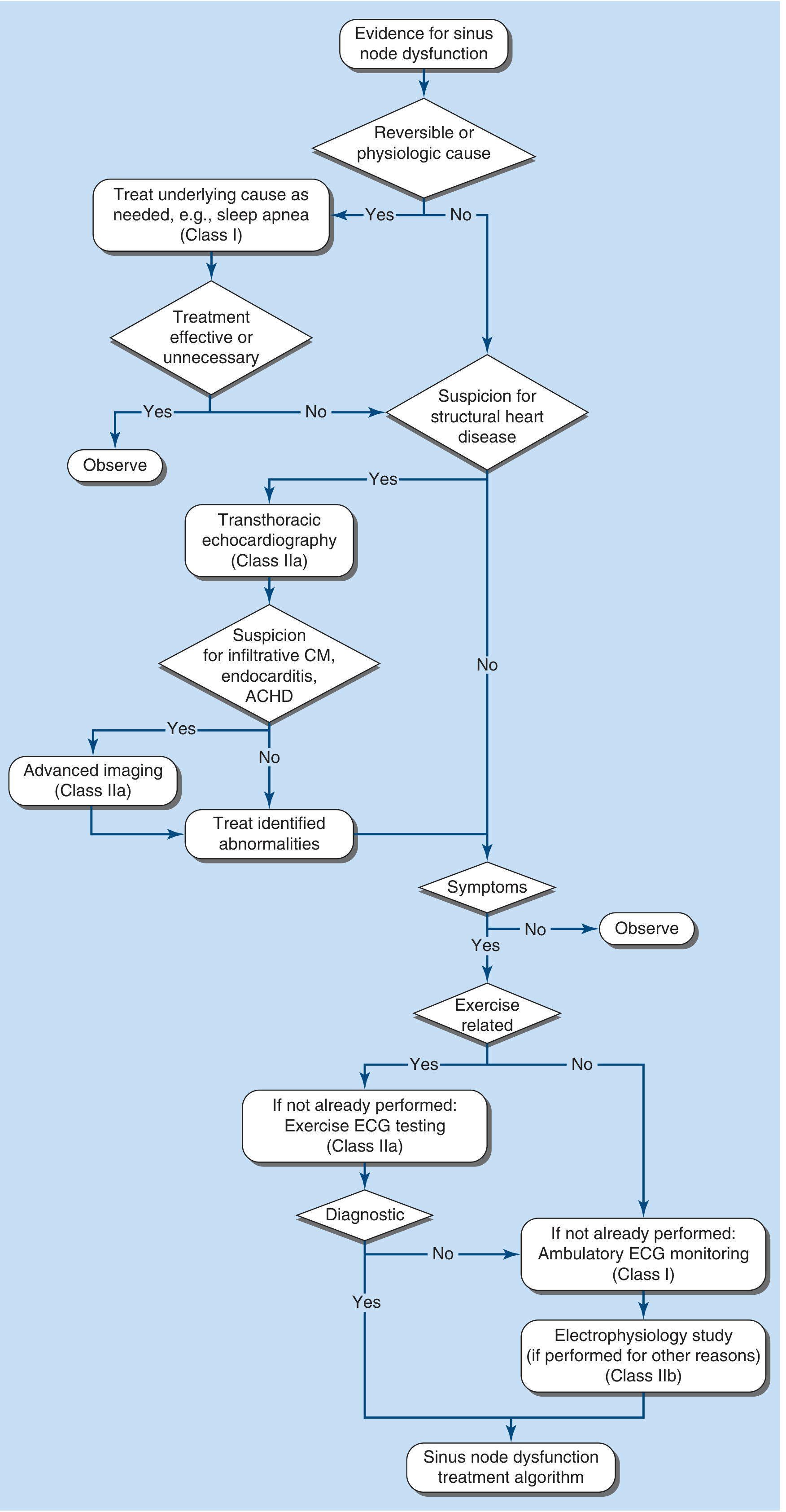
Algorithm steps (2018 ACC/AHA/HRS Guideline):
-
Identify reversible/physiologic cause?
- Yes → Treat underlying cause (sleep apnea, hypothyroidism, drug discontinuation) - Class I
- If treatment effective or unnecessary → Observe
-
Suspicion for structural heart disease?
- Yes → Transthoracic echocardiography (Class IIa)
- If suspicion for infiltrative cardiomyopathy, endocarditis, or adult congenital heart disease (ACHD) → Advanced imaging (Class IIa) (cardiac CT or cardiac MRI)
-
Symptomatic?
- No → Observe
- Yes → Proceed
-
Exercise-related symptoms?
- Yes → Exercise ECG testing (Class IIa)
- Not diagnostic / No → Ambulatory ECG monitoring (Class I) (Holter, event monitor, implantable loop recorder)
- If electrophysiology study performed for other reasons → EPS (Class IIb)
-
→ Proceed to sinus node dysfunction treatment algorithm
Sinus Node Dysfunction Spectrum
Sinus bradycardia is part of the broader sinus node dysfunction (SND) spectrum, which includes:
- Sinus bradycardia
- Sinoatrial exit block (1st, 2nd [Type I/II], 3rd degree)
- Sinus arrest (pause >2-3 seconds)
- Chronotropic incompetence (max HR <100 bpm on exercise)
- Tachycardia-bradycardia (tachy-brady) syndrome - alternating bradyarrhythmia and tachyarrhythmia (typically AF); identified by prolonged sinus node recovery after AF termination
- Sick sinus syndrome = SND + symptoms (fatigue, dizziness, syncope, HF worsening)
Acute Management
Per Rosen's Emergency Medicine and 2025 AHA ACLS Algorithm:
| Situation | Treatment |
|---|---|
| Asymptomatic | No treatment, identify cause |
| Symptomatic (hemodynamically stable) | Treat reversible cause; atropine 1 mg IV q3-5 min (max 3 mg) |
| Symptomatic (refractory to atropine) | Dopamine 5-20 mcg/kg/min IV or epinephrine 2-10 mcg/min IV |
| Severe/unstable | Transcutaneous pacing |
| Post-cardiac transplant | Isoproterenol 2-10 mcg/min (atropine is ineffective due to denervation) |
| Hypothermia with confirmed sinus bradycardia + pulse | Atropine and pacing usually NOT recommended (myocardial irritability) |
| Spinal cord injury | Theophylline/aminophylline (adenosine blockade) |
Long-Term Management / Pacemaker Indications
- Asymptomatic sinus bradycardia - NOT an indication for permanent pacing; not associated with adverse outcomes
- Sleep-related pauses from high vagal tone without other symptoms - pacemaker generally not indicated
- Symptomatic SND where symptom-rhythm correlation is established - permanent pacemaker is indicated
- Tachy-brady syndrome - treat the tachyarrhythmia first (antiarrhythmics or catheter ablation); if pharmacologic AV nodal agents cannot be avoided, permanent pacing may be required
- Reversible causes first - eliminate offending medications, treat hypothyroidism, revascularize if ischemia is driving bradycardia
- Temporary pharmacologic options (when pacemaker must be delayed due to active infection, etc.): methylxanthines (theophylline) or beta agonists (terbutaline)
Key principle: There is no established heart rate below which pacemaker implantation is automatically indicated. The decision is symptom-driven and requires demonstrated symptom-rhythm correlation. - Harrison's Principles of Internal Medicine, 22E (2025)
Sources:
- Harrison's Principles of Internal Medicine, 22E (2025, McGraw Hill) - p. 1963-1965
- Goldman-Cecil Medicine, International Edition - p. 562
- Braunwald's Heart Disease, 2-Vol Set - Chapter 68
- Rosen's Emergency Medicine, 9e - Chapter 65
- 2018 ACC/AHA/HRS Guideline on Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay (via Harrison's Fig. 251-3)
- 2025 AHA Adult Bradycardia With a Pulse Algorithm
This is a shared conversation. Sign in to Orris to start your own chat.