Explain 10 most common heart disease in ecg with photos
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram atrial fibrillation
Searching Images
myocardial infarction STEMI ST elevation ECG
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
heart block complete third degree AV block ECG
Searching Images
left ventricular hypertrophy ECG voltage criteria
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG
Searching Images
bundle branch block left LBBB ECG morphology
Searching Images
ventricular fibrillation ECG chaotic rhythm cardiac arrest
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
Brugada syndrome ECG coved pattern right bundle
I now have excellent ECG images for all 10 conditions. Let me compile the comprehensive answer:
10 Most Common Heart Diseases on ECG
1. Atrial Fibrillation (AF)
Mechanism: Chaotic, disorganized atrial electrical activity from multiple reentrant circuits, abolishing coordinated atrial contraction.
Key ECG Features:
- Absent P waves — replaced by irregular fibrillatory (f) waves, best seen in V1 and lead II
- Irregularly irregular R-R intervals — no two R-R intervals are the same
- Narrow QRS complexes (unless aberrant conduction coexists)
- Rate varies: uncontrolled (>100 bpm), rate-controlled (60–100 bpm)

Associated conditions: Hypertension, valvular disease, heart failure, hyperthyroidism, alcohol excess.
2. ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery causes transmural ischemia and injury, with characteristic evolving ECG changes.
Key ECG Features:
- ST elevation ≥1 mm in ≥2 contiguous leads (≥2 mm in V1–V3)
- Hyperacute T waves — tall, peaked (earliest change)
- Reciprocal ST depression in mirror leads
- Pathological Q waves — develop within hours (necrosis marker)
- T-wave inversion — follows in hours to days
Lead localization:
| Territory | Leads with ST elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | V7–V9 (reciprocal depression V1–V3) | RCA/LCx |

3. Complete (Third-Degree) AV Block
Mechanism: Total failure of conduction between atria and ventricles at the AV node or His bundle. The ventricles are driven by a slow escape pacemaker.
Key ECG Features:
- AV dissociation — P waves and QRS complexes are completely independent
- Regular P-P intervals (atrial rate ~60–100 bpm)
- Regular but slow R-R intervals (ventricular escape rate: junctional 40–60 bpm with narrow QRS; ventricular <40 bpm with wide QRS)
- No fixed PR interval — P waves "march through" QRS complexes
- Wide QRS if infra-nodal block; narrow QRS if junctional escape

Causes: Inferior MI, Lyme disease, calcific degeneration, medication toxicity (digoxin, beta-blockers), post-surgical.
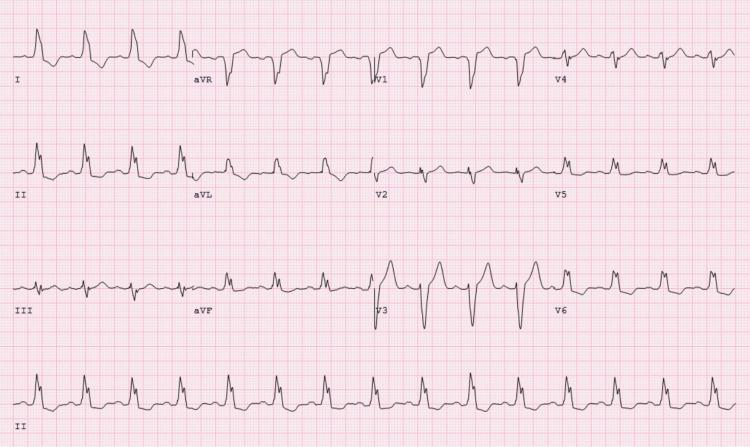
4. Ventricular Tachycardia (VT)
Mechanism: Rapid, life-threatening rhythm originating from ventricular ectopic focus, often in the context of structural heart disease or ischemia.
Key ECG Features:
- Wide QRS complexes (>120 ms), rate 100–250 bpm
- Regular rhythm (monomorphic VT)
- AV dissociation — P waves visible, unrelated to QRS (pathognomonic when present)
- Fusion beats and capture beats — confirm VT
- Concordance — all precordial QRS complexes pointing same direction
- Brugada criteria: absence of RS complex in any precordial lead, RS interval >100 ms

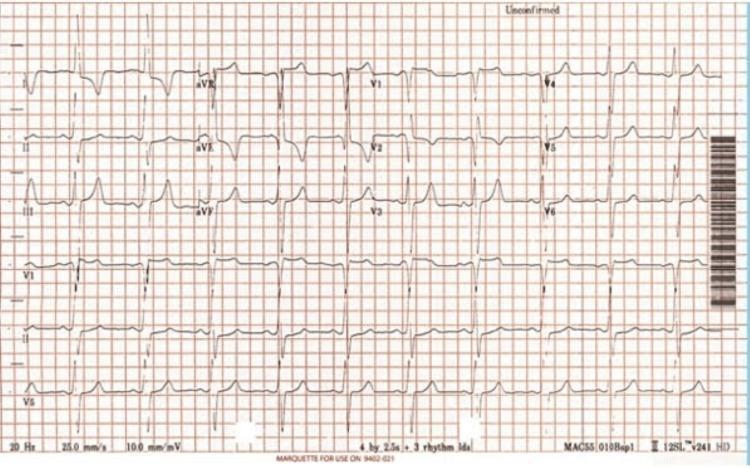
5. Left Bundle Branch Block (LBBB)
Mechanism: Failure of conduction down the left bundle branch forces the right ventricle to depolarize first, with abnormal spread to the left ventricle. New LBBB may indicate acute MI (Sgarbossa criteria apply).
Key ECG Features:
- QRS duration >120 ms
- Broad, notched (M-shaped) R wave in lateral leads I, aVL, V5, V6
- Deep QS complex in V1–V3 (no r wave)
- Discordant ST-T changes — ST/T in opposite direction to QRS
- Left axis deviation common
Causes: Hypertension, cardiomyopathy, aortic valve disease, coronary artery disease, acute anterior MI.
6. Left Ventricular Hypertrophy (LVH)
Mechanism: Increased ventricular muscle mass generates larger electrical voltages, producing tall QRS complexes and secondary repolarization abnormalities ("strain pattern").
Key ECG Features:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- Left axis deviation
- "Strain pattern": ST depression and T-wave inversion in lateral leads (I, aVL, V5–V6)
- Left atrial enlargement (broad, notched P wave in II; biphasic P in V1)
Causes: Chronic hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy.
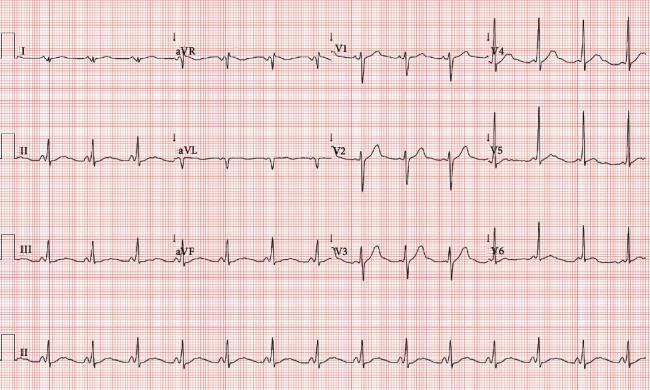
7. Wolff-Parkinson-White (WPW) Syndrome
Mechanism: An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle. This creates the classic "delta wave" and predisposes to re-entrant tachycardias (SVT, and dangerously, AF with rapid ventricular response).
Key ECG Features:
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke at start of QRS
- Wide QRS complex (>120 ms) due to fusion of pre-excited and normal conduction
- Secondary ST-T changes discordant to delta wave
- Pseudo-Q waves in inferior or lateral leads may mimic infarction
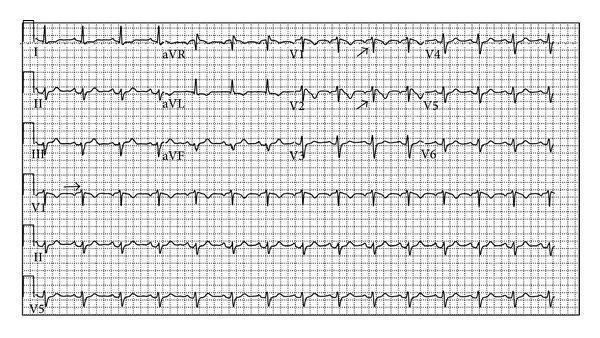
8. Pulmonary Embolism (PE)
Mechanism: Sudden obstruction of pulmonary vasculature causes acute right ventricular pressure overload (cor pulmonale), reflected on ECG as right heart strain.
Key ECG Features:
- Sinus tachycardia — most common finding (seen in ~70%)
- S1Q3T3 pattern — deep S in lead I + Q wave in lead III + T-wave inversion in lead III
- T-wave inversions in V1–V4 — right ventricular strain
- Incomplete or complete RBBB
- Right axis deviation
- P pulmonale (tall peaked P waves >2.5 mm in II) in severe cases
- New AF may occur

9. Ventricular Fibrillation (VF)
Mechanism: Completely disorganized ventricular electrical activity with no coordinated contraction. Immediately fatal without defibrillation. Often preceded by VT or ischemia.
Key ECG Features:
- Chaotic, disorganized baseline with no identifiable P waves, QRS complexes, or T waves
- Irregular, rapidly undulating waveforms of variable amplitude and frequency
- Coarse VF: larger amplitude oscillations (more amenable to defibrillation)
- Fine VF: lower amplitude, may resemble asystole — indicates prolonged arrest or deteriorating myocardium
- Heart rate not measurable

Management: Immediate defibrillation (200 J biphasic), CPR, epinephrine, amiodarone per ACLS protocol.
10. Brugada Syndrome
Mechanism: Autosomal dominant sodium channelopathy (SCN5A mutation most common) causing abnormal cardiac conduction, predominantly in the right ventricle's epicardium. Causes sudden cardiac death in structurally normal hearts, classically in young Asian males at rest or during sleep.
Key ECG Features (Type 1 — diagnostic):
- Coved-type ST elevation ≥2 mm in ≥1 right precordial lead (V1–V3)
- Downsloping ST segment descending directly into a negative (inverted) T wave
- Incomplete or complete RBBB pattern in V1
- May be concealed and unmasked by fever, sodium channel blockers (ajmaline, flecainide), cocaine, or vagotonia
- Type 2 (saddle-back pattern): not diagnostic without drug challenge
Management: ICD for survivors of cardiac arrest or symptomatic patients; quinidine for recurrent VF storms.
Quick Reference Summary
| # | Condition | Key ECG Finding | Rate |
|---|---|---|---|
| 1 | Atrial Fibrillation | Absent P waves, irregular R-R | Variable |
| 2 | STEMI | ST elevation ± reciprocal depression | Variable |
| 3 | Complete AV Block | AV dissociation, slow escape rhythm | Atria fast, ventricles slow |
| 4 | Ventricular Tachycardia | Wide complex, regular, AV dissociation | 100–250 bpm |
| 5 | LBBB | Wide QRS, M-shaped R in I/V6, QS in V1 | Variable |
| 6 | LVH | High voltage, strain pattern | Normal |
| 7 | WPW | Short PR, delta wave, wide QRS | Variable |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, T inv V1–V4 | Tachycardia |
| 9 | Ventricular Fibrillation | Chaotic baseline, no QRS | Not measurable |
| 10 | Brugada Syndrome | Coved ST elevation V1–V3 | Normal (at baseline) |
This is a shared conversation. Sign in to Orris to start your own chat.