Describe various stages of lung development , enumerate various congenital anomalies of lung
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here it is:
Stages of Lung Development
Human lung development is visible from approximately 4 post-conceptual weeks (PCW 4) and is classically divided into five stages. The lungs form from the laryngotracheal groove of the endoderm at the fourth pharyngeal arch; the splanchnic mesoderm provides muscular and cartilaginous coverings and forms the visceral pleura, while the somatic mesoderm forms the parietal pleura.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 64-65
- Fishman's Pulmonary Diseases, p. 1856
Stage 1 - Embryonic Stage (PCW 4 to 7)
- The respiratory diverticulum outpouches from the foregut; the common foregut tube divides into the trachea (ventral) and esophagus (dorsal).
- Two primary bronchi form; these divide into secondary (lobar) bronchi - three on the right and two on the left - by 5 weeks.
- The earliest respiratory epithelial marker is Nkx2-1 (also known as TTF-1), expressed in foregut endoderm-derived ventral progenitor cells.
- Left-right asymmetry of the lung buds is already specified at this stage, in concert with visceral organ lateralization.
- The lung buds elongate into surrounding mesenchyme and begin branching morphogenesis.
Stage 2 - Pseudoglandular Stage (5 to 16 weeks)
- The lung continues to grow laterally and caudally on exposure to the splanchnic mesoderm.
- Conducting airways branch progressively until terminal bronchioles (16th to 25th generation) are formed by 16 weeks.
- On cross-section, the lung resembles a developing exocrine gland - hence "pseudoglandular."
- Mesenchymal tissue differentiates into ciliated columnar epithelial cells, goblet cells, and eventually type II pneumocytes.
- This stage marks the transition zone between conducting and respiratory airways.
- No gas exchange is possible at this stage - fetuses born in this period cannot survive.
- Key molecular drivers: FGF10 (from mesenchyme) drives branching; WNT, BMP, and Sprouty signaling networks shape the branching pattern.
Stage 3 - Canalicular Stage (16 to 26 weeks)
- The epithelium differentiates into type I pneumocytes (alveolar cells), the primary structural cells for gas exchange.
- Extensive angiogenesis occurs - capillary networks form surrounding alveolar cells.
- Lamellar bodies begin forming within type II pneumocytes - these are the primary storage sites for surfactant (surfactant production begins around 24 weeks).
- Conducting airways continue to elongate and widen, creating the characteristic "canalicular" appearance.
- The air-blood barrier begins to form as capillaries approximate type I cells.
- Survival becomes marginally possible at the limits (~22-24 weeks) if intensive neonatal care is provided, owing to early surfactant production and minimal gas exchange capacity.
Stage 4 - Saccular Stage (26 weeks to term)
- Progressive maturation of type I and type II pneumocytes; interstitial tissue decreases.
- Air spaces called primary sacculi form - these are the future gas exchange units.
- Exponential growth in primary sacculi with formation of primary septa between each saccular unit (primary septa contain a double capillary loop).
- The terminal saccules are simpler and wider than mature alveoli; further maturation occurs postnatally.
- Surfactant production increases substantially; adequate surfactant is typically present by ~34-36 weeks.
- Premature birth at this stage risks respiratory distress syndrome (RDS) due to surfactant deficiency.
Stage 5 - Alveolar Stage (postnatal - continues through early childhood)
- True alveoli form by ingrowth of secondary crests from primary saccular walls, thinning the double capillary loop into a single loop.
- Secondary myofibroblasts (at the tips of secondary septa) produce elastin and elastin cross-linking enzymes critical for septum formation. They form a "fishnet-like" network that contracts to generate novel septa.
- Alveolar type 2 (AT2) cells produce surfactant and can differentiate into AT1 cells, which cover ~95% of the surface area.
- The conventional view holds that alveolarization is complete by 6-7 years; however, more recent evidence shows new alveoli continue to be added into the 20s.
- There are approximately 480 million alveoli in a mature lung, with a gas-exchange surface area of ~130 m².
Summary Table
| Stage | Gestational Age | Key Events |
|---|---|---|
| Embryonic | PCW 4-7 | Lung buds, trachea-esophagus separation, primary bronchi |
| Pseudoglandular | 5-16 wks | Branching to terminal bronchioles; glandular appearance |
| Canalicular | 16-26 wks | Type I & II pneumocyte differentiation, angiogenesis, surfactant begins |
| Saccular | 26 wks - term | Primary sacculi, double capillary loops, surfactant maturation |
| Alveolar | Birth - ~7+ yrs | Secondary septa, true alveoli, single capillary loops |
Congenital Anomalies of the Lung
Developmental disorders of the lung are classified into three broad categories: Airway, Parenchymal, and Vascular Disorders.
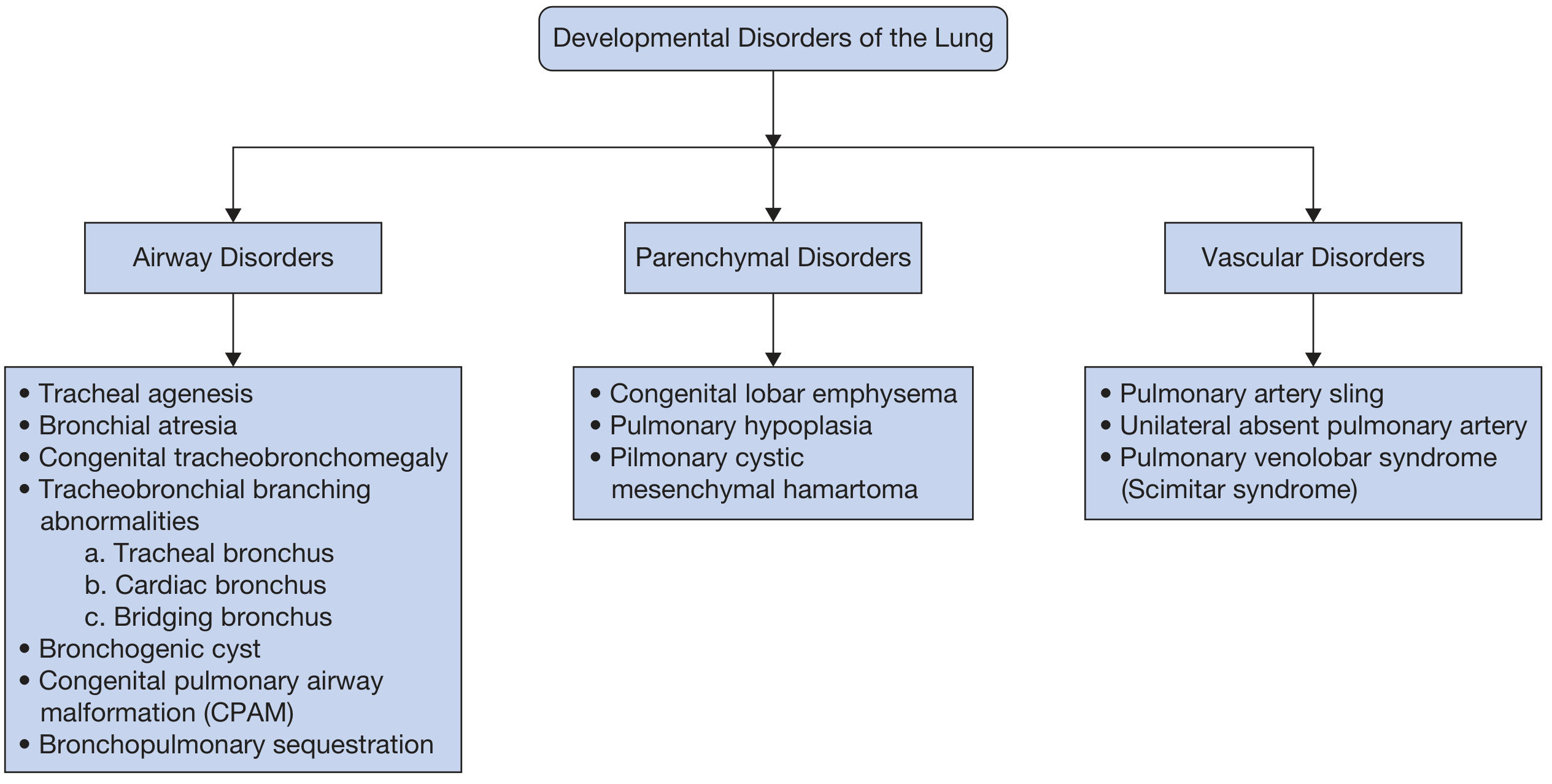
- Fishman's Pulmonary Diseases, Figure 105-1
A. Airway Disorders
1. Tracheal Agenesis
Rare and fatal anomaly where the trachea fails to form. Incompatible with sustained life.
2. Bronchial Atresia
Focal obliteration of a lobar, segmental, or subsegmental bronchus during development, leading to air trapping in the affected segment (via collateral ventilation) and a mucus-filled bronchocele. Often asymptomatic, discovered incidentally.
3. Congenital Tracheobronchomegaly (Mounier-Kuhn Syndrome - MKS)
Marked dilation of the trachea and central bronchi due to atrophy or absence of smooth muscle and elastic fibers. Associated with tracheobronchomalacia (TBM). Patients present with recurrent lower respiratory infections and productive cough. Chest CT shows dilated trachea and central bronchi with tracheal diverticula. Treatment is supportive (airway clearance, antibiotics); silicone stents or tracheobronchoplasty in severe cases.
4. Tracheobronchial Branching Abnormalities
Anomalous bronchi are classified by their anatomic relationship to the ipsilateral pulmonary artery (eparterial/hyparterial):
- Tracheal bronchus: Abnormal bronchus arising directly from the trachea (88% are displaced upper lobe bronchi; 12% are supernumerary). Right-sided prevalence 0.1-2%, left-sided 0.3-1%. Usually asymptomatic; may cause recurrent infections or atelectasis.
- Cardiac bronchus: Accessory bronchus arising from the medial wall of the right main or intermediate bronchus, directed toward the pericardium. Most are blind-ending; may cause recurrent infections.
- Bridging bronchus: Rare; the right lower lobe bronchus anomalously originates from the left main bronchus. Associated with pulmonary artery sling.
5. Bronchogenic Cyst
-
A congenital anomaly derived from the lung bud of the foregut during the embryonic stage.
-
Characterized by a fluid-filled blind cystic pouch - location depends on timing of the defect:
- Early defect → mediastinal cysts (paratracheal, subcarinal, paraesophageal, hilar)
- Later defect → intrapulmonary cysts (predominantly lower lobes)
-
Incidence: ~1 in 42,000-68,000 admissions; male predilection.
-
Often asymptomatic; may cause superior vena cava syndrome, dyspnea, dysphagia, or recurrent infections (postobstructive pneumonia in 82% of symptomatic cases).
-
Histology (diagnostic): respiratory ciliated pseudostratified columnar epithelium with bronchial glands, smooth muscle, and cartilage in the cyst wall.
-
CT imaging: well-defined ovoid cyst that does not enhance with contrast; content variable (water to soft-tissue density), may show "milk of calcium."
-
Management: symptomatic cysts are surgically resected; asymptomatic cysts managed conservatively.
-
Fishman's Pulmonary Diseases, p. 1861
6. Congenital Pulmonary Airway Malformation (CPAM)
Formerly called congenital cystic adenomatoid malformation (CCAM).
- Pathogenesis: abnormal branching of primitive bronchioles with arrested development, primarily during the pseudoglandular stage (but may occur as late as the alveolarization stage).
- Prevalence: ~9 cases per 100,000 total births.
- Up to 70% present as cystic lesions in distal bronchi; a subset presents as solid masses.
- Overexpression of Hoxb5 (beyond pseudoglandular stage), KGF/FGF7, and PDGFB has been implicated.
Stocker Classification - 5 Types:
| Type | Site of Origin | Characteristics | Frequency |
|---|---|---|---|
| Type 0 | Trachea/primary bronchus | Often lethal | Rare |
| Type 1 | Distal bronchus | Single large cyst (3-10 cm), most common, 50-70% of cases | Most common |
| Type 2 | Terminal bronchioles | Small evenly-spaced cysts, 15-30% | 2nd most common |
| Type 3 | Bronchioles/alveolar ducts | Microcystic, large solid-appearing mass | Less common |
| Type 4 | Distal acinus/alveoli | Large peripheral cysts, risk of malignant transformation | Less common |
-
Prenatal: Detected on ultrasound as macrocystic (>5 mm) or microcystic (<5 mm); CVR (cyst volume ratio) >1.6 associated with hydrops fetalis risk.
-
Large lesions cause mediastinal shift, pulmonary hypoplasia, cardiac compression, and hydrops.
-
Most small lesions regress in the 3rd trimester.
-
Management: Surgical resection (usually lobectomy) postnatal for symptomatic or large lesions.
-
Fishman's Pulmonary Diseases, p. 1862; Miller's Anesthesia, p. 9036
7. Bronchopulmonary Sequestration (BPS)
- Second most common developmental lung disorder; accounts for ~6.4% of all congenital pulmonary malformations.
- A lung mass with no communication with the tracheobronchial tree - does not participate in respiration.
- Pathogenesis: originates from a supernumerary lung bud; supplied by systemic arterial circulation (thoracic aorta 75%, abdominal aorta 25%) - this systemic arterial supply is its hallmark.
- Hypothesized to originate as a supernumerary lung bud; the relationship to pleural formation determines type.
Two Types:
| Feature | Intralobar BPS | Extralobar BPS |
|---|---|---|
| Pleura | Shares lung's pleura | Own visceral pleura |
| Origin timing | Before pleural formation | After pleural formation |
| Location | Left lower lobe (60%), right lower lobe (38%) | Left hemithorax (48%), subdiaphragmatic (18%) |
| Venous drainage | Usually pulmonary veins | Usually systemic veins |
| Associated anomalies | Less common | More common (50% co-exist with CPAM type 2) |
| Recurrent infections | 71% | 31% |
-
Imaging: Color Doppler US identifies systemic feeding artery; CT chest angiography is the modality of choice in adults (shows consolidation/mass with feeding artery in left lower hemithorax).
-
Management: Asymptomatic small BPS - conservative; larger or symptomatic lesions - surgical resection (VATS) at 6-12 months.
-
Fishman's Pulmonary Diseases, p. 1863
B. Parenchymal Disorders
8. Congenital Lobar Emphysema (CLE) / Congenital Lobar Overinflation
-
Rare (1 in 20,000 live births); accounts for ~10.5% of developmental lung disorders; more common in males.
-
Pathogenic mechanisms:
- Focal cartilage defect: absent or deficient bronchial cartilage → dynamic airway collapse → air trapping (25% of cases)
- Polyalveolar lobe: fivefold increase in number of normal alveoli (alveolar giantism) without over-distension - described by Hislop and Reid (1970)
-
Sites (in order of frequency): left upper lobe (42-57%) > right middle lobe (27-35%) > right upper lobe (14-30%).
-
Associated with cardiac anomalies (VSD, ASD, tetralogy of Fallot) in some cases.
-
Imaging: Chest X-ray shows focal lobar hyperlucency with contralateral mediastinal shift; bronchovascular markings are preserved within the hyperlucent area (distinguishes from pneumothorax). CT confirms lobar overdistension with compression of adjacent lung.
-
Management: Most cases identified in early neonatal period; symptomatic cases require lobectomy. Asymptomatic adults - observation.
-
Fishman's Pulmonary Diseases, p. 1864
9. Pulmonary Hypoplasia
- Underdevelopment of one or both lungs; may result from extrinsic compression (diaphragmatic hernia), oligohydramnios (reducing fetal breathing movements and lung fluid), or intrinsic developmental defects.
- Oligohydramnios impairs lung development since fetal breathing movements and lung fluid distension are required for normal lung growth.
- Unilateral hypoplasia presents with mediastinal shift toward the affected side; CT shows marked volume loss with bronchiectasis in the hypoplastic lung.
10. Pulmonary Cystic Mesenchymal Hamartoma
- Rare condition involving inappropriate mesenchymal tissue in the lung arising from disordered mesoderm during development.
- Slow-growing nodules that cavitate into cystic structures >1 cm; most often diagnosed in adults (chronic cough, hemoptysis, pneumothorax).
- Histology: normal respiratory epithelium surrounding cysts with a layer of primitive mesenchymal cells with dark nuclei (low mitotic activity distinguishes from malignancy).
- Rare malignant transformation to rhabdomyosarcoma reported.
C. Vascular Disorders
11. Pulmonary Artery Sling (PAS)
- The left main pulmonary artery anomalously originates from the right main pulmonary artery and traverses between the trachea and esophagus to reach the left lung.
- Associated with tracheal stenosis due to complete tracheal rings in up to 80% of patients.
- Type I: Sling above the carina - compresses right main bronchus and distal trachea, causing hyperinflation of right lung; often associated with tracheal bronchus.
- Type II: Sling at T5-T6 level, associated with complete tracheal rings and more severe stenosis.
12. Unilateral Absent Pulmonary Artery (UAPA)
- Failure of development of one pulmonary artery, typically the right.
- Presents with recurrent pulmonary infections, hemoptysis, or pulmonary hypertension.
- The affected lung is hypoplastic and supplied by bronchial/systemic collaterals.
13. Scimitar Syndrome (Pulmonary Venolobar Syndrome)
- A complex syndrome where the right pulmonary vein drains anomalously into the inferior vena cava instead of the left atrium, creating a "scimitar sign" on chest X-ray (curved opaque line resembling a Turkish sword).
- Associated with hypoplasia of the right lung, dextroposition of the heart, and systemic arterial supply to the right lower lobe.
- Often presents in infancy with heart failure or recurrently as an incidental finding in adults.
Quick Reference Summary
| Category | Anomaly |
|---|---|
| Airway | Tracheal agenesis, bronchial atresia, congenital tracheobronchomegaly (MKS), tracheal/cardiac/bridging bronchus, bronchogenic cyst, CPAM, bronchopulmonary sequestration |
| Parenchymal | Congenital lobar emphysema, pulmonary hypoplasia, pulmonary cystic mesenchymal hamartoma |
| Vascular | Pulmonary artery sling, unilateral absent pulmonary artery, scimitar syndrome |
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Miller's Anesthesia | Mulholland and Greenfield's Surgery
This is a shared conversation. Sign in to Orris to start your own chat.