What is new in post partum Haemorrage
Reading File
Finding Sources
Searching PubMed
"postpartum hemorrhage" management
Searching the Web
new updates postpartum hemorrhage management guidelines 2024 2025
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK619233
Reading Article
PMID: 40237648
Reading Article
PMID: 40743526
Reading Article
PMID: 41056961
Reading File
I now have comprehensive, high-quality data from WHO 2025 guidelines, Cochrane reviews, The Lancet, and ACOG. Here is the full answer:
What's New in Postpartum Haemorrhage (PPH) - 2025 Updates
Major Development: WHO Consolidated Guidelines (October 2025)
The WHO, FIGO, and International Confederation of Midwives released the first-ever consolidated guidelines specifically focused on PPH on October 5, 2025, launched at the FIGO World Congress in Cape Town. These include 51 recommendations (20 new or updated; 31 revalidated) across prevention, diagnosis, treatment, supportive care, and health systems.
1. Revised Definition of PPH
The threshold is no longer a simple volume-only rule. The new preferred definition is:
Blood loss ≥ 1,000 mL accompanied by signs of hypovolemia (rather than the older ≥500 mL cutoff)
A major Lancet meta-analysis by Gallos et al. (2025) of 312,151 women across 23 countries (PMID: 41056961) found that:
- The conventional 500 mL threshold has only 75.7% sensitivity for predicting mortality or severe morbidity
- Sensitivity improves to 87-88% when combining blood loss of 300-450 mL plus any abnormal haemodynamic sign (pulse >100, SBP <100, DBP <60, or shock index >1.0)
- This supports a combined clinical marker approach over volume alone for earlier diagnosis
2. New Guidance on Tranexamic Acid (TXA) - KEY UPDATE
Two new WHO recommendations (2025):
- Rec. 14 (NEW): TXA is NOT recommended for prevention of PPH at vaginal birth
- Rec. 15 (NEW): TXA is NOT recommended for prevention of PPH at caesarean birth
This is a significant shift - TXA remains recommended for treatment of established PPH, but prophylactic use is no longer supported. The Cochrane meta-analysis by Cheema et al. (2023) on TXA for prevention at C-section confirms lack of benefit to justify prophylactic use.
3. Uterotonic Rankings - Updated Cochrane Network Meta-Analysis (2025)
The landmark Cochrane network meta-analysis by Gallos et al. (2025) (PMID: 40237648) covering 122 trials, 121,931 women across 48 countries found:
| Rank | Agent | PPH ≥500 mL vs Oxytocin |
|---|---|---|
| 1st (tied) | Ergometrine + Oxytocin | RR 0.76 (high certainty) |
| 1st (tied) | Misoprostol + Oxytocin | RR 0.70 (moderate certainty) |
| Equivalent | Carbetocin | Similar (high certainty) |
- Combination agents outperform oxytocin alone, though with more side effects
- WHO still recommends oxytocin 10 IU (IM/IV) as the first-line standard (Rec. 24, revalidated), but combination therapy is preferred where feasible
- Carbetocin (heat-stable formulation) continues to be supported especially in low-resource settings without cold chains
4. Updated Diagnostic Approach
- Universal objective blood loss measurement (calibrated drapes, weighing) is now recommended - not visual estimation
- Standardized risk assessment tool before and after every delivery
- Early action at combined threshold of ≥300 mL + any haemodynamic sign, rather than waiting for 500 mL
5. ACOG Update: Nonsurgical Hemorrhage-Control Devices (October 2025)
ACOG released a focused Clinical Practice Update (PMID: 40743526) revising guidance on intrauterine balloon tamponade and other nonsurgical devices, updating Practice Bulletin 183 (2017). Key points include:
- Uterine balloon tamponade remains a core second-line intervention
- Newer devices (e.g. Jada system - intrauterine vacuum-induced hemorrhage control) are now addressed with revised guidance
- Devices should be used as part of a structured bundle, not in isolation
6. Structured Treatment Bundle (Revalidated & Reinforced)
The first-response care bundle (Rec. 29, revalidated) for all vaginal births includes:
- Objective assessment of blood loss
- Rapid uterine massage
- Uterotonic agent (oxytocin IV/IM)
- Tranexamic acid 1g IV (for treatment, within 3 hours of delivery)
- IV fluids
- Genital tract examination
- Clear escalation to second-line (balloon tamponade → surgical repair → embolization → hysterectomy)
7. Aetiology Confirmed by Global Data
The Lancet meta-analysis confirmed the relative proportions:
- Uterine atony: 70.6% of cases
- Genital tract trauma: 16.9%
- Retained placenta: 16.4%
- Coagulation disorders: less common
This reinforces targeting atony prevention as the primary strategy.
8. Health Systems & Global Implementation
The 2025 WHO guidelines place major emphasis on:
- Supply chain strengthening for heat-stable uterotonics in low-resource settings
- Training modules and simulation-based emergency drills for frontline workers
- National implementation guides, developed with UNFPA
- Equity lens - most of the 70,000 annual deaths occur in low- and middle-income countries
Summary Table: What Changed in 2025
| Area | Old Guidance | New/Updated 2025 |
|---|---|---|
| Definition | ≥500 mL | ≥1,000 mL with haemodynamic signs OR ≥300-450 mL + abnormal vitals |
| TXA prophylaxis | Debated/used by some | NOT recommended (vaginal or C-section) |
| TXA treatment | Recommended | Confirmed - within 3 hours |
| Best uterotonic | Oxytocin alone | Oxytocin + ergometrine OR oxytocin + misoprostol superior |
| Diagnosis threshold | Volume-only | Volume + haemodynamic signs combined |
| Nonsurgical devices | ACOG 2017 guidance | Updated 2025 (includes Jada system) |
Key sources:
- WHO Consolidated PPH Guidelines 2025, executive summary
- Gallos et al., Lancet 2025 - prognostic markers meta-analysis (PMID: 41056961)
- Gallos et al., Cochrane 2025 - uterotonic network meta-analysis (PMID: 40237648)
- ACOG Clinical Practice Update 2025 on nonsurgical hemorrhage-control devices
Massive transfusion b protocol what is it
Reading File
Finding Sources
Finding Sources
Searching PubMed
"massive transfusion protocol" hemorrhage ratio
Searching the Web
massive transfusion protocol MTP blood product ratios 1:1:1 definition activation criteria 2024 2025
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I have the MTP flowchart from Schwartz's Surgery and rich textbook content. Here is the comprehensive answer:
Massive Transfusion Protocol (MTP) - Complete Overview
What Is It?
A Massive Transfusion Protocol (MTP) is a pre-activated, institutional, multidisciplinary algorithm that coordinates the rapid delivery of blood products in fixed ratios to patients with life-threatening hemorrhage. It exists because massive blood loss involves more than just red cell loss - it depletes clotting factors, fibrinogen, and platelets simultaneously, making ratio-based replacement superior to packing red cells alone.
- Rosen's Emergency Medicine, p. 2429
- Henry's Clinical Diagnosis, p. 881
Definition of Massive Transfusion (Trigger Volume)
| Setting | Definition |
|---|---|
| Adults | > 10 units PRBCs in 24 hours OR ≥3 units in 1 hour OR ≥150 mL/min blood loss |
| Adults (volume) | Loss of 1 complete blood volume (~5L/70 mL/kg) in 24h |
| Children | ≥80 mL/kg in 24h OR ≥40 mL/kg in 3 hours |
These volume-based definitions have limited real-world utility because transfusion must often begin before such thresholds are reached.
Activation Criteria - The ABC Score
The Assessment of Blood Consumption (ABC) Score is the most commonly used validated trigger. Activate MTP if 2 or more of the following are present:
| Criterion | Score |
|---|---|
| Penetrating mechanism | 1 |
| SBP ≤ 90 mmHg | 1 |
| Heart rate > 120 bpm | 1 |
| Positive FAST exam | 1 |
ABC score ≥ 2 = Activate MTP
Other activation triggers used clinically:
- Blood loss > 150 mL/min
- Blood loss > 50% of blood volume within 3 hours
- Anticipated need for ≥3 units in 1 hour
The Core Concept: Damage Control Resuscitation (DCR)
MTP is the clinical implementation of Damage Control Resuscitation, which arose from military experience in Iraq and Afghanistan. The rationale:
- Massive hemorrhage depletes all blood components - red cells, plasma, platelets, and clotting factors
- Replacing only red cells (old strategy) worsens the lethal triad: coagulopathy + hypothermia + acidosis
- Reconstituting whole blood by giving components in a ratio approximating whole blood is the solution
The 1:1:1 Ratio - The Standard of Care
The landmark PROPPR trial (Pragmatic Randomized Optimal Platelet and Plasma Ratios) compared:
| Ratio (PRBCs : FFP : Platelets) | Outcome |
|---|---|
| 1:1:1 | Fewer deaths from exsanguination at 24h |
| 2:1:1 | No difference in overall 30-day mortality |
The 1:1:1 ratio is now the standard in most MTPs, despite no difference in 30-day mortality - the reduction in exsanguination death at 24h is the key benefit.
- Rosen's Emergency Medicine, p. 2430
- Bailey & Love's Surgery, 28th Ed.
MTP Protocol - Step-by-Step (Denver Health/Schwartz's Surgery Model)
Here is the MTP flowchart from Schwartz's Principles of Surgery:
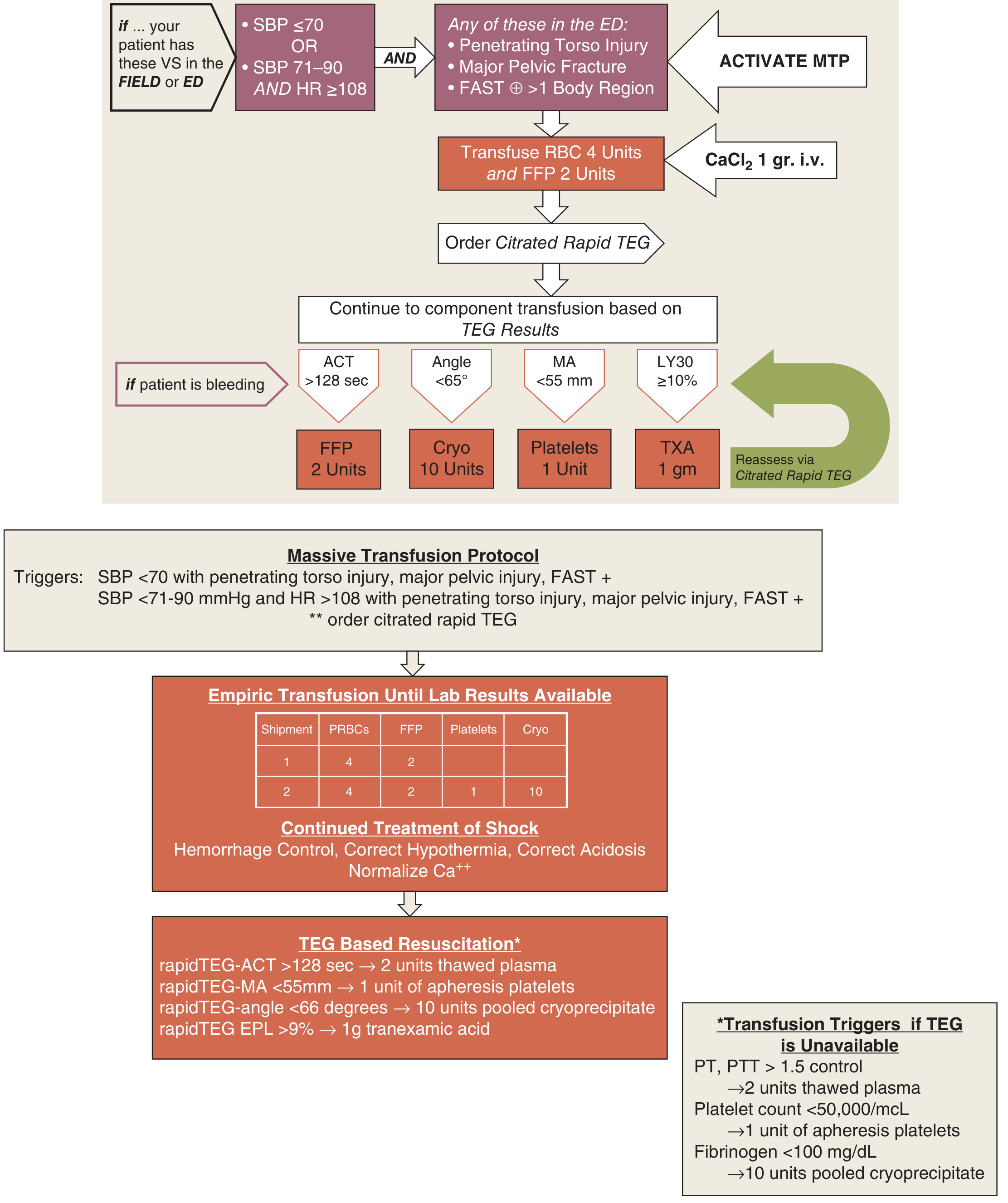
Figure 7-33 from Schwartz's Principles of Surgery 11th Ed - Denver Health Medical Center MTP
Phase 1 - Trigger & Activate
- SBP ≤70 OR (SBP 71-90 AND HR ≥108) PLUS any of: penetrating torso injury / major pelvic fracture / FAST+ in >1 region
- ACTIVATE MTP - call blood bank, notify OR, anaesthesia, lab
- Give CaCl₂ 1g IV immediately (combat citrate-induced hypocalcaemia)
Phase 2 - Empiric (Pre-Lab) Transfusion
| Shipment | PRBCs | FFP | Platelets | Cryo |
|---|---|---|---|---|
| Pack 1 | 4 units | 2 units | - | - |
| Pack 2 | 4 units | 2 units | 1 unit | 10 units |
Simultaneously: correct hypothermia, correct acidosis, normalize Ca²⁺, haemorrhage control
Phase 3 - Goal-Directed (TEG/ROTEM-Guided)
Once a Citrated Rapid TEG result is available, replace components based on specific deficits:
| TEG Parameter | Threshold | Give |
|---|---|---|
| ACT (clotting time) | > 128 sec | FFP 2 units |
| Angle (fibrin kinetics) | < 65° | Cryoprecipitate 10 units |
| MA (platelet function) | < 55 mm | Platelets 1 unit (apheresis) |
| LY30 (fibrinolysis) | ≥ 10% | TXA 1g |
If TEG is unavailable, use conventional coagulation triggers:
- PT/PTT > 1.5x control → FFP 2 units
- Platelets < 50,000/µL → 1 unit apheresis platelets
- Fibrinogen < 100 mg/dL → 10 units pooled cryoprecipitate
The "Lethal Triad" MTP Targets
COAGULOPATHY
△
/|\
/ | \
/ | \
ACIDOSIS──────HYPOTHERMIA
MTP directly counteracts all three limbs by:
- Clotting factors/FFP → treat coagulopathy
- Warming all blood products → prevent/treat hypothermia
- Restoring perfusion (not crystalloid overload) → treat acidosis
Blood Products in MTP - At a Glance
| Product | Role | Key Points |
|---|---|---|
| PRBCs | Oxygen-carrying capacity | Start with Group O uncrossmatched if urgent; Rh-negative preferred for females of childbearing age |
| FFP (Fresh Frozen Plasma) | Replaces all clotting factors | Given when PT/APTT >1.5x normal |
| Platelets | Haemostatic plug | Give if count <50,000; use apheresis units |
| Cryoprecipitate | Fibrinogen + Factor VIII + vWF + XIII | Give if fibrinogen <100 mg/dL |
| Whole Blood (Low-Titer Type O) | All components in one unit | Re-emerging as preferred option especially in pre-hospital/military settings |
| Tranexamic Acid (TXA) | Antifibrinolytic | 1g IV within 3 hours of injury/bleeding onset; do NOT give after 3 hours |
| Calcium | Reverses citrate toxicity | Give CaCl₂ or calcium gluconate with every pack |
Whole Blood - The Emerging Trend
Low-Titer Group O Whole Blood (LTOWB) is regaining favour, especially in trauma and military settings:
- Provides all components in physiological ratios in a single unit
- Reduces logistical burden in pre-hospital care
- Reduces donor exposures
- ACS TQIP now includes guidance on LTOWB in MTP frameworks
When to Stop (MTP Termination Criteria)
- Bleeding is controlled surgically
- Haemodynamics are stable
- Labs normalize (Hb, PT/INR, fibrinogen, platelets in acceptable range)
- Clinical decision by senior physician
Complications of Massive Transfusion
| Complication | Mechanism | Management |
|---|---|---|
| Hypothermia | Cold blood products | Fluid warmers, warm blankets, Bair Hugger |
| Hypocalcaemia | Citrate chelates calcium | CaCl₂ 1g IV per pack |
| Hyperkalaemia | Stored blood releases K⁺ | Monitor, ECG |
| Metabolic acidosis | Hypoperfusion + citrate | Optimize O₂ delivery; NOT bicarbonate |
| TRALI | Immune reaction to donor plasma | Supportive; use male donor or pathogen-reduced plasma |
| Dilutional coagulopathy | Volume replacing coagulation factors | Guided by TEG/ROTEM |
| Hypothermic coagulopathy | Cold reduces clotting factor activity | Warming |
Key Evidence Base
- The PROPPR trial (Holcomb et al.): 1:1:1 reduces exsanguination deaths at 24h vs 2:1:1
- Williams et al., Cochrane 2025 - transfusion of blood products for PPH management (PMID: 39911088)
- ACS TQIP MTP Guidelines - standardization across trauma systems, 2025
- TEG/ROTEM-guided resuscitation associated with lower mortality vs conventional coag parameters in trauma (Rosen's EM, p. 2430)
Bottom line: MTP is not just "give lots of blood" - it is a structured, ratio-driven, goal-directed protocol that reconstructs whole blood from components, fights the lethal triad, and is triggered early using validated criteria (ABC score ≥2). The 1:1:1 ratio of PRBCs:FFP:platelets is the current standard, with TEG/ROTEM enabling personalised correction once labs are available.
This is a shared conversation. Sign in to Orris to start your own chat.