In detail medical answer about deep vein thrombosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"deep vein thrombosis"[MeSH Terms] AND diagnosis AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Deep Vein Thrombosis (DVT) - Comprehensive Medical Overview
Definition and Epidemiology
Deep vein thrombosis (DVT) is the formation of a thrombus within the deep venous system, most commonly in the deep veins of the lower extremities. It is part of the broader spectrum of venous thromboembolism (VTE), which includes pulmonary embolism (PE). DVT accounts for more than 90% of cases of thrombophlebitis and phlebothrombosis - these two terms are largely interchangeable designations for venous thrombosis accompanied by inflammation. [Robbins & Kumar Basic Pathology, p. 3359]
DVT is largely an asymptomatic disease - only about one-fourth of cases present with identifiable complaints, making clinical vigilance essential. [S Das Manual on Clinical Surgery, p. 5100]
Anatomy of the Lower Limb Venous System
Understanding DVT requires familiarity with the deep venous anatomy. The deep veins most commonly affected include, from distal to proximal:
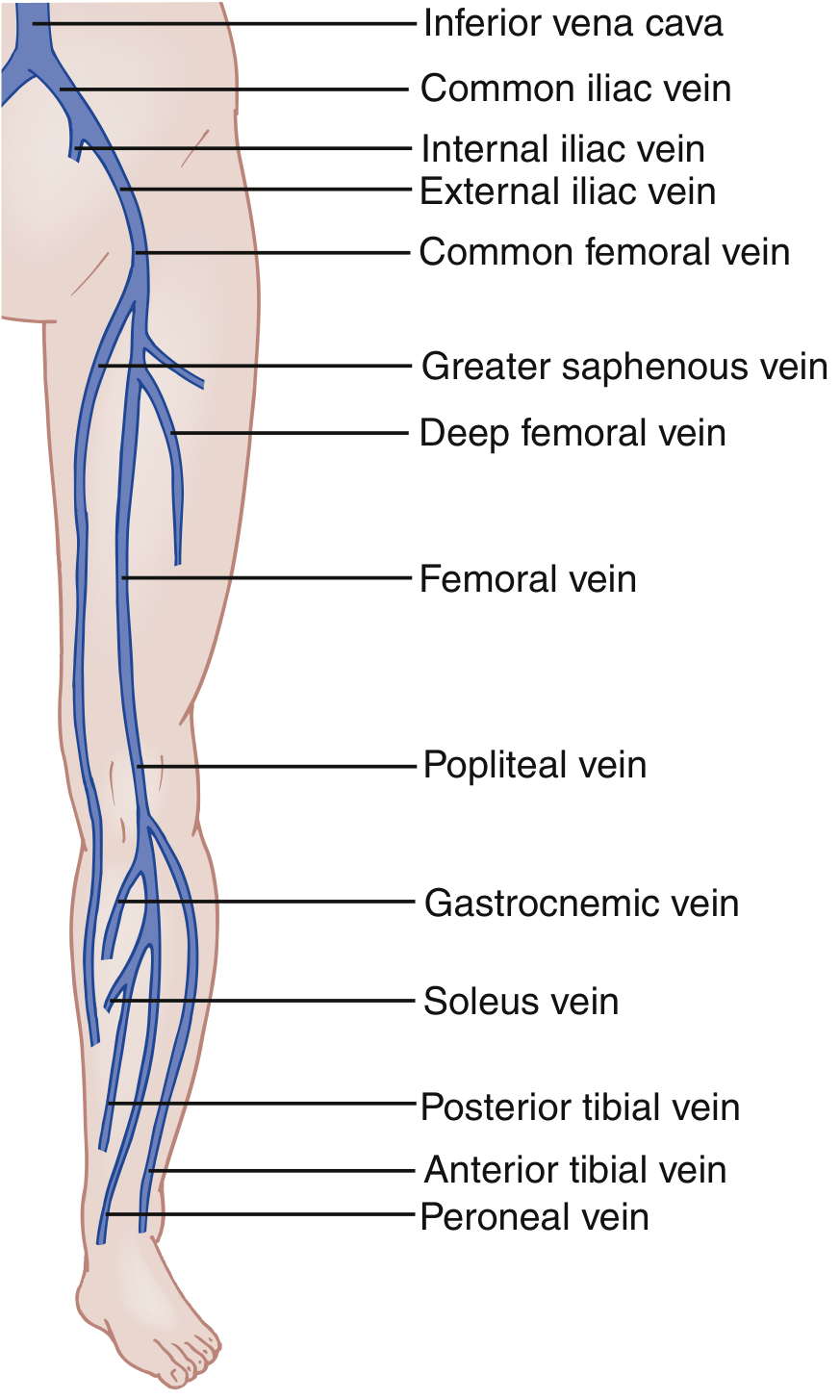
Diagram of lower limb venous anatomy showing the deep vein system - from the tibial and peroneal veins distally to the common femoral vein and iliac vessels proximally. (Source: Rosen's Emergency Medicine)
- Distal (calf) veins: Posterior tibial, anterior tibial, peroneal, gastrocnemius, and soleus veins
- Proximal veins: Popliteal, femoral (previously "superficial femoral"), common femoral, and iliac veins
A three-point ultrasound covers common femoral, femoral, and popliteal veins; a whole-leg ultrasound additionally covers the tibial, peroneal, gastrocnemius, and saphenous veins. [Rosen's Emergency Medicine, p. 1196]
Pathophysiology: Virchow's Triad
The three fundamental factors predisposing to venous thrombosis form Virchow's Triad, first described in the mid-19th century:
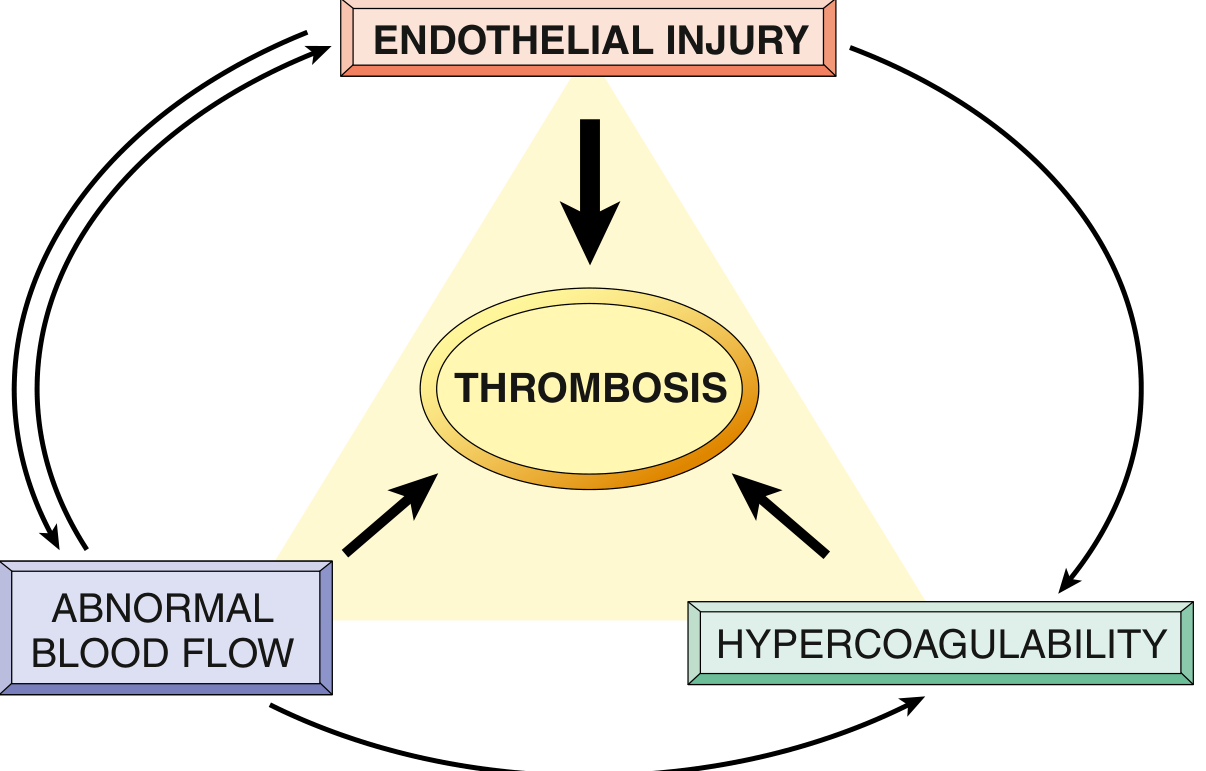
Virchow's Triad - Endothelial integrity is the most important factor. Abnormal blood flow and hypercoagulability interact and contribute to thrombosis. (Source: Robbins & Kumar Basic Pathology)
1. Endothelial Injury
Endothelial injury activates a "prothrombotic" gene expression shift in the endothelium. Key mechanisms include:
- Downregulation of coagulation inhibitors (thrombomodulin, endothelial protein C receptor, tissue factor pathway inhibitor)
- Upregulation of tissue factor expression
- Increased secretion of plasminogen activator inhibitors (PAI), which limit fibrinolysis by antagonizing t-PA and urokinase
Causes include physical injury, infection, cytokines, inflammatory mediators, hypercholesterolemia, homocystinemia, and cigarette smoke toxins. [Robbins & Kumar Basic Pathology, p. 2502-2506]
2. Stasis / Abnormal Blood Flow
Stasis is the dominant factor in venous thrombosis. Under laminar flow, platelets are segregated to the vessel center away from the endothelium. Stasis disrupts this by:
- Allowing platelets and leukocytes to contact the endothelium
- Slowing washout of activated clotting factors
- Impeding inflow of clotting factor inhibitors
- Promoting endothelial gene expression changes that favor procoagulant activity
Clinical causes: prolonged immobility, post-surgical bedrest, pregnancy (gravid uterus compresses iliac veins), calf muscle pump failure, plaster immobilization. [Robbins & Kumar Basic Pathology, p. 2518-2526]
3. Hypercoagulability
Hypercoagulability refers to an abnormally high tendency to clot, caused by alterations in coagulation factors. It is divided into:
Primary (Inherited) Causes:
- Factor V Leiden mutation - an amino acid substitution renders Factor V resistant to proteolysis by Protein C. Heterozygotes have a 3-4x increased risk; homozygotes have a 25-50x increased risk. Found in ~60% of patients with recurrent DVT. Present in 2-15% of those of European ancestry.
- Prothrombin gene mutation (G20210A) - found in 1-2% of the general population, causes increased prothrombin gene expression
- Protein C or S deficiency - loss of natural anticoagulant control
- Antithrombin III deficiency
- Hyperhomocysteinemia
Secondary (Acquired) Causes:
- Active malignancy (especially pancreatic cancer - "Trousseau's syndrome")
- Prolonged immobility or surgery
- Oral contraceptive pills / hormone replacement therapy
- Pregnancy and puerperium
- Antiphospholipid antibody syndrome
- Heparin-induced thrombocytopenia (HIT)
- Polycythemia vera, thrombocytosis
- Nephrotic syndrome
- Inflammatory bowel disease
[Robbins & Kumar Basic Pathology, p. 2531-2540; Gray's Anatomy for Students, p. 6488-6490]
Risk Factors
DVT occurs when one or more elements of Virchow's triad are present. Major clinical risk factors include:
| Risk Category | Examples |
|---|---|
| Surgical | Pelvic surgery, total hip/knee replacement, abdominal surgery, orthopaedic trauma |
| Immobilization | Bedrest ≥3 days, plaster cast, long-haul travel |
| Medical illness | Active cancer, heart failure, inflammatory bowel disease, sepsis |
| Pregnancy | Compression of iliac veins by gravid uterus, hypercoagulable state |
| Medications | Combined oral contraceptive pill, hormone therapy |
| Thrombophilia | Factor V Leiden, prothrombin mutation, protein C/S deficiency |
| Prior VTE | Previous DVT or PE significantly increases recurrence risk |
| Vascular access | Central venous catheters, pacemaker wires (upper extremity DVT) |
Surgical risk stratification (Bailey & Love): High-risk procedures include pelvic elective and trauma surgery, total knee and hip replacement. Medium-risk includes abdominal, gynaecological, and urological surgery. [Bailey & Love's Surgery, p. 345]
Clinical Features
Symptoms:
- Unilateral limb pain and swelling (hallmark signs)
- Mild cramping or a sense of fullness in the calf
- Heaviness or aching of the affected limb
- Most cases are asymptomatic - only ~25% present with symptoms
Signs:
- Pitting edema of the affected extremity
- Erythema and warmth
- Tenderness to palpation along the deep venous distribution
- Dilation of superficial collateral veins
- Rarely: a palpable venous cord
- Homans' sign (calf pain on dorsiflexion of the foot) - historically used but neither sensitive nor specific
Special patterns:
- Left leg predominance: The left iliac vein is vulnerable to compression by the left iliac artery (May-Thurner syndrome), explaining a slightly higher frequency of left-sided DVT
- Bilateral DVT: Found in fewer than 10% of ED patients
- Phlegmasia cerulea dolens: Massive iliofemoral thrombosis causing severe limb swelling, cyanosis, and threatened limb viability
- Upper extremity DVT: >90% occur with an indwelling catheter; in young athletes, the dominant arm can develop effort-induced thrombosis from thoracic outlet compression (Paget-Schroetter syndrome)
[Rosen's Emergency Medicine, p. 1196; Bailey & Love's Surgery, p. 5668-5672]
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Cellulitis | Fever more prominent; DVT co-exists in only ~3% of cases |
| Ruptured Baker cyst | History of knee pathology; popliteal fullness |
| Venous insufficiency | Chronic bilateral changes; varicose veins |
| Muscle/tendon injury | Trauma history; localized to muscle belly |
| Hematoma | Trauma history; no flow abnormality on Doppler |
| Asymmetric edema | Heart failure, liver disease - usually bilateral |
| Lymphedema | Non-pitting, progressive; lymphatic history |
[Rosen's Emergency Medicine, p. 1196]
Diagnosis
Step 1: Pre-Test Probability - Wells DVT Score
The two-level Wells DVT Score is the most widely validated clinical decision tool:
| Clinical Feature | Points |
|---|---|
| Active cancer (treatment ongoing, within 6 months, or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of lower extremities | +1 |
| Recently bedridden ≥3 days, or major surgery within 12 weeks (general/regional anaesthesia) | +1 |
| Localized tenderness along distribution of the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling at least 3 cm larger than the asymptomatic side | +1 |
| Pitting edema confined to the symptomatic leg | +1 |
| Collateral (non-varicose) superficial veins | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely as DVT | -2 |
Interpretation:
- Score ≤1: Low probability (~2% pre-test probability)
- Score ≥2: High probability (~28% pre-test probability)
The Wells score can be combined with D-dimer to triage patients safely. [Rosen's Emergency Medicine, p. 1197; Bailey & Love's Surgery, p. 5673]
Note: The Wells score is not validated in pregnancy. The LEFt score is used instead:
- L = Left leg suspicion (+1)
- E = Edema (+1)
- Ft = First trimester (+1) A LEFt score of 0 or 1 indicates low probability.
Step 2: D-Dimer
- Measures enzymatic breakdown of cross-linked fibrin from any intravascular thrombus
- Standard cutoff: >500 ng/mL = positive
- A negative D-dimer in a low-probability patient excludes proximal DVT with ~92% sensitivity
- Age-adjusted threshold: Age × 10 ng/mL - safely reduces need for ultrasound in elderly patients while maintaining ~95% sensitivity
- D-dimer specificity is low in pregnancy, cancer, infection, recent surgery, and inflammatory states
- A negative D-dimer in a high-probability patient does not exclude DVT - imaging is still required
Step 3: Venous Compression Ultrasound (VCU/Doppler)
The gold standard for DVT diagnosis. Diagnostic criteria include:
- Non-compressibility of the vein under probe pressure (most reliable sign)
- Absent or abnormal flow on Doppler
- Absence of flow augmentation with calf compression
- Absent respiratory phasicity
- Direct visualization of intraluminal thrombus
A normal vein collapses completely under probe pressure; a thrombosed vein does not compress.
Three-point ultrasound: Evaluates common femoral, femoral, and popliteal veins.
Whole-leg ultrasound: Adds tibial, peroneal, and gastrocnemius veins - detects isolated distal DVT.
Patients with high pre-test probability + positive D-dimer + negative proximal ultrasound should have a repeat ultrasound at 1 week to detect propagation of distal thrombus. [Rosen's Emergency Medicine, p. 1197-1201]
Other Imaging
- CT venography: Used in suspected pelvic or IVC thrombosis
- MRI venography: Excellent for pelvic veins, pregnancy, or when ultrasound is inconclusive
- Conventional contrast venography: Historical gold standard, now rarely used due to invasiveness
Treatment
Anticoagulation - First-Line Therapy
The goal is to prevent thrombus propagation, PE, and recurrence while allowing natural fibrinolysis. Anticoagulation should be started immediately upon diagnosis (or even upon high clinical suspicion while awaiting imaging). [Rosen's Emergency Medicine, p. 1199; Bailey & Love's Surgery, p. 5654]
Direct-Acting Oral Anticoagulants (DOACs) - First Choice:
- Rivaroxaban (Factor Xa inhibitor) and Apixaban (Factor Xa inhibitor) - do NOT require bridging with LMWH; first-choice anticoagulants for most DVT patients
- Dabigatran (direct thrombin inhibitor) - requires initial LMWH bridge for 5-10 days
- DOACs are equally effective as warfarin in preventing recurrent VTE but are associated with fewer bleeding complications, especially fewer intracranial bleeds
- Do not require regular INR monitoring; well-tolerated by patients
Low-Molecular-Weight Heparin (LMWH):
- Subcutaneous injection; treatment dose initiated immediately
- Preferred initial therapy for cancer-associated DVT (DOACs increasingly used here too)
- Preferred in pregnancy (does not cross the placenta)
- Adjust or avoid in significant renal impairment (use unfractionated heparin instead)
Unfractionated Heparin (UFH):
- IV infusion; used in severe renal impairment or when rapid reversal may be needed
- Requires aPTT monitoring
Alternatives in heparin-induced thrombocytopenia (HIT):
- Fondaparinux (indirect Factor Xa inhibitor)
- Bivalirudin (direct thrombin inhibitor)
- Argatroban
Duration of anticoagulation:
- Provoked DVT (transient risk factor, e.g., surgery): minimum 3 months
- Unprovoked DVT: At least 3 months; often extended based on recurrence risk vs. bleeding risk
- Cancer-associated DVT: Indefinite (as long as cancer is active)
- Recurrent DVT or major thrombophilia: Often indefinite
Anticoagulant Reversal Agents
| Anticoagulant | Reversal Agent |
|---|---|
| Heparin (UFH) | Protamine sulfate |
| Warfarin | FFP, 4-Factor PCC, Vitamin K |
| Dabigatran | Idarucizumab |
| Rivaroxaban, Apixaban | Andexanet alfa |
[Rosen's Emergency Medicine, p. 1199]
IVC Filter
Patients who cannot be safely anticoagulated (due to active bleeding, high bleeding risk, or severe bleeding diathesis) should be considered for a temporary inferior vena cava (IVC) filter to prevent PE. Retrievable filters are preferred - they should be removed once anticoagulation is safely initiated. [Bailey & Love's Surgery, p. 5659-5163]
Endovascular Interventions (Catheter-Directed Thrombolysis / CDT)
- Increasingly used in acute iliofemoral DVT with symptoms ≤14 days duration
- Goals: restore venous patency, relieve acute symptoms, reduce risk of post-thrombotic syndrome
- Techniques include: catheter-directed thrombolysis (CDT), pharmacomechanical thrombectomy, venoplasty, and stenting
- Systemic thrombolysis for DVT (without concurrent limb ischemia) has not been shown to improve mortality or reduce post-thrombotic syndrome and increases bleeding risk - not routinely recommended
- Selected patients with massive iliofemoral thrombosis or threatened limb viability may benefit [Rosen's Emergency Medicine, p. 1201; Bailey & Love's Surgery, p. 5666; Fuster & Hurst's The Heart, p. 3307]
Compression and Ambulation
- Compression stockings: No longer routinely recommended to prevent post-thrombotic syndrome (recent evidence does not consistently support this benefit). However, some patients report quality-of-life improvement, and timing of initiation may matter.
- Early ambulation after starting anticoagulation is encouraged - it reduces the incidence of post-thrombotic syndrome. [Rosen's Emergency Medicine, p. 1201]
DVT Prophylaxis
All surgical and hospitalized patients should be risk-stratified for VTE prophylaxis within 24 hours of admission. Risk should be reassessed if clinical status changes. [Bailey & Love's Surgery, p. 5653]
Methods:
- Mechanical: Graded compression stockings (TED stockings), intermittent pneumatic compression (IPC) devices / calf pumps
- Pharmacological: Subcutaneous LMWH (e.g., enoxaparin), UFH, fondaparinux
- Compression stockings are contraindicated in peripheral arterial disease, peripheral neuropathy, severe oedema, or skin breakdown
Note: Compression stockings are not offered to patients with suspected/confirmed peripheral arterial disease or neuropathy.
Complications
1. Pulmonary Embolism (PE)
The most feared and potentially fatal complication. The thrombus dislodges (typically from the iliofemoral system) and travels through the right heart into the pulmonary vasculature. Small emboli cause pleuritic chest pain; massive PE causes right heart failure and cardiovascular collapse. Most PEs can be treated with anticoagulation and monitoring; severe right heart strain indicates need for thrombolysis or catheter embolectomy. [Bailey & Love's Surgery, p. 5669; Gray's Anatomy for Students, p. 6494-6496]
2. Post-Thrombotic Syndrome (PTS)
Occurs in 20-50% of DVT patients. Results from damage to venous valves, leading to venous insufficiency and chronic venous hypertension. Features include:
- Chronic leg pain, heaviness, and fatigue
- Persistent edema
- Paresthesia, induration
- Skin discoloration (lipodermatosclerosis)
- Varicose veins
- In severe cases: venous stasis ulcers Early endovascular intervention for iliofemoral DVT may reduce the risk of PTS. [Rosen's Emergency Medicine, p. 1201; Bailey & Love's Surgery, p. 5166]
3. Venous Gangrene / Phlegmasia
Massive occlusion of venous outflow causing arterial compromise and limb ischemia - a surgical emergency.
4. Recurrent VTE
Unprovoked DVT carries a significant recurrence risk (~30% at 5 years without ongoing anticoagulation), which drives decisions about long-term anticoagulation.
Special Populations
Pregnancy
- DVT is more common in pregnancy due to IVC compression by the gravid uterus (especially left-sided), hormonal hypercoagulability, and venous stasis
- LMWH is the preferred anticoagulant - does not cross the placenta
- Warfarin and DOACs are contraindicated in pregnancy
- Use the LEFt score for clinical probability assessment
- Anticoagulate until at least 6 weeks postpartum (total duration minimum 3 months)
Cancer Patients
- Cancer is both a risk factor and a trigger for DVT investigation (unprovoked DVT should prompt malignancy screening)
- LMWH was historically preferred; DOACs (especially apixaban and rivaroxaban) are increasingly first-choice for cancer-associated VTE based on recent trial data
- Duration: indefinite while cancer is active
Upper Extremity DVT
-
90% associated with indwelling central venous catheters, pacemaker wires, or infusion devices
- Paget-Schroetter syndrome: effort-induced subclavian vein thrombosis in young athletes (dominant arm)
- Treat with anticoagulation; consider catheter removal if possible
Summary Algorithm
Suspected DVT
↓
Calculate Wells Score
↓
Low probability (≤1) High probability (≥2)
↓ ↓
D-Dimer Venous Ultrasound
↓ ↓
Negative → DVT excluded Positive → Diagnose DVT
Positive → Ultrasound Negative → D-Dimer
↓
If D-Dimer negative → DVT excluded
If D-Dimer positive → Repeat US in 1 week
↓
Initiate anticoagulation
(DOAC preferred, or LMWH)
Duration ≥3 months
Key Teaching Points
- DVT is often clinically silent - most cases are asymptomatic; a high index of suspicion based on risk factors is required
- Virchow's Triad (stasis, endothelial injury, hypercoagulability) underlies all DVT pathogenesis
- Wells score + D-dimer is the validated diagnostic pathway; venous ultrasound non-compressibility is the gold standard imaging sign
- DOACs (rivaroxaban, apixaban) are now first-line treatment for most patients with DVT - no bridging required, fewer bleeds than warfarin
- The most life-threatening complication is PE; the most common chronic complication is post-thrombotic syndrome (20-50% of patients)
- LMWH is preferred in pregnancy and renal failure patients (use UFH in severe renal impairment)
- IVC filter is a bridge for patients who cannot be anticoagulated
- Early ambulation after anticoagulation reduces post-thrombotic syndrome
Sources: Rosen's Emergency Medicine (Concepts and Clinical Practice) | Bailey & Love's Short Practice of Surgery, 28th Ed | Robbins & Kumar Basic Pathology | Gray's Anatomy for Students | Fuster & Hurst's The Heart, 15th Ed | S Das Manual on Clinical Surgery, 13th Ed
in detail about gbs
Finding Sources
Finding Sources
Searching PubMed
"Guillain-Barre syndrome"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the comprehensive content needed. Let me compile the full detailed answer on GBS.
Guillain-Barré Syndrome (GBS) - Comprehensive Medical Overview
Definition
Guillain-Barré syndrome (GBS) refers to a group of acquired, inflammatory polyradiculoneuropathies that share three defining features:
- Acute onset
- Cytoalbuminologic dissociation in cerebrospinal fluid (elevated protein with low cell count)
- Monophasic course (one episode that progressively worsens then typically recovers)
It is one of the most common life-threatening diseases of the peripheral nervous system and a leading cause of non-traumatic paralysis worldwide. [Goldman-Cecil Medicine, p. 4080]
Historical Background
In 1916, Guillain, Barré, and Strohl described the key clinical features: motor weakness, areflexia, paresthesias with minor sensory loss, and elevated CSF protein without pleocytosis. Multifocal inflammatory demyelination of spinal roots and peripheral nerves was later characterized histologically. Before the introduction of positive-pressure ventilation, mortality was approximately 33%; with modern critical care, mortality is now approximately 1-5%. [Bradley & Daroff's Neurology, p. 2663]
Epidemiology
- Annual incidence: 0.81 to 1.89 cases per 100,000 persons per year worldwide
- Sex: Men more commonly affected than women (ratio ~1.4:1)
- Age: Incidence increases with age, though it affects all age groups
- Most common form: Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) accounts for ~97% of cases in North America and Europe
- Preceding infection: Identified in ~60-70% of patients, typically 1-4 weeks before neurological symptoms
- ICU admission: Required in 20-30% of patients due to respiratory failure; mortality rises to ~14.3% in mechanically ventilated patients
- GBS and COVID-19: Not substantially associated with SARS-CoV-2 infection or most vaccines; a slight increase of 0.6 cases/100,000 doses was noted with ChADOx1nCoV-19 (AstraZeneca). GBS incidence actually declined during the pandemic due to reduced exposure to common triggering infections.
- Zika virus: Significantly increased risk of all GBS variants
[Goldman-Cecil Medicine, p. 4080; Miller's Anesthesia, p. 12033]
Subtypes and Classification
GBS is a heterogeneous syndrome with several distinct variants:
Common Subtypes
| Subtype | Key Features | Common Trigger |
|---|---|---|
| AIDP (Acute Inflammatory Demyelinating Polyradiculoneuropathy) | Most common (97% in North America/Europe); demyelinating; sensorimotor | Various infections |
| AMAN (Acute Motor Axonal Neuropathy) | Pure motor; axonal injury; common in China (summer epidemics in children/young adults) | C. jejuni (GM1 antibodies) |
| AMSAN (Acute Motor-Sensory Axonal Neuropathy) | Both motor and sensory axons; most severe; poorest recovery | C. jejuni |
Rare Variants
| Variant | Classic Triad | Antibody |
|---|---|---|
| Miller-Fisher Syndrome (MFS) | Ophthalmoplegia + Ataxia + Areflexia | Anti-GQ1b (>85% of cases) |
| Pharyngeal-cervical-brachial | Weakness of oropharyngeal, neck, and arm muscles | Anti-GT1a |
| Paraparetic GBS | Weakness limited to legs | - |
| Bickerstaff brainstem encephalitis | Overlap with MFS; altered consciousness | Anti-GQ1b |
MFS accounts for 6% of GBS cases in Western countries but up to 18% in Taiwan, reflecting geographic variation in antigenic triggers. [Bradley & Daroff's Neurology, p. 2663; Miller's Anesthesia, p. 12034]
Pathophysiology
Molecular Mimicry - The Core Mechanism
All forms of GBS probably result from postinfectious molecular mimicry: the immune system mounts a response against a pathogen antigen that structurally resembles ganglioside or glycolipid antigens on peripheral nerve components. When antibodies and T-cells cross-react with peripheral nerve antigens, autoimmune injury follows.
Key mechanism:
- A preceding infection (most commonly Campylobacter jejuni) presents antigens structurally similar to ganglioside components of peripheral nerve myelin or axolemma
- T cell-mediated responses and antibody-mediated responses both contribute, though T cells are believed to play the dominant role
- The injury is most extensive at nerve roots and proximal nerve segments
- Mononuclear cell infiltrates rich in macrophages mediate myelin stripping in AIDP
Specific Antibody-Target Associations
| Antibody | Target Ganglioside | GBS Subtype |
|---|---|---|
| Anti-GM1 | GM1 ganglioside (axolemma) | AMAN - worse prognosis |
| Anti-GalNAc-GD1a | Ganglioside on nodes of Ranvier | AMAN |
| Anti-GD1b | Ganglioside | AMSAN |
| Anti-GQ1b | Paranodal region, neuromuscular junction | Miller-Fisher syndrome |
| Anti-GT1a | Oropharyngeal cranial nerve antigens | Pharyngeal-cervical-brachial variant |
In AIDP, mechanisms are less clear - molecular mimicry may not be the sole driver, as it involves a more complex T cell and antibody-mediated attack on myelin.
Infectious Triggers
| Pathogen | Notes |
|---|---|
| Campylobacter jejuni | Most common bacterial trigger (especially AMAN) |
| Cytomegalovirus (CMV) | Common viral trigger |
| Epstein-Barr virus (EBV) | Well-established trigger |
| HIV | May also cause direct nerve injury |
| Zika virus | Significantly elevated risk of all subtypes |
| Hepatitis E virus | Important in Belgium and Netherlands (5-10% of cases) |
| SARS-CoV-2 | Slight association; risk declined overall during pandemic |
| Chikungunya | Regional association |
[Robbins & Kumar Basic Pathology, p. 472; Goldman-Cecil Medicine, p. 4080; Miller's Anesthesia, p. 12034]
Clinical Features
Typical Presentation (AIDP)
The onset follows a biphasic pattern:
- Prodrome (1-4 weeks prior): Respiratory tract infection, gastroenteritis, or other illness
- Neurological phase: Rapidly progressive weakness, usually ascending
Progressive weakness is the most common initial symptom. It typically begins in the legs and ascends to the arms, trunk, and cranial nerves. The pattern can range from mild (difficulty walking) to severe (total quadriplegia and respiratory failure).
Key Clinical Features
Motor:
- Ascending, symmetrical flaccid weakness - the hallmark
- Areflexia or hyporeflexia - almost universal and required for diagnosis
- Proximal weakness is common (not just "ascending from distal")
- 5% have isolated cranial nerve involvement that then descends
- Respiratory failure in 20-30% due to diaphragm and intercostal muscle weakness
Sensory:
- Mild sensory loss or paresthesias in most patients
- Sensory symptoms typically less prominent than motor weakness
- Neuropathic/deafferentation pain is common - truncal in distribution, severe, responds better to anticonvulsants than opiates
Cranial Nerve Involvement:
- Bilateral facial nerve (CN VII) palsy in ~50% of patients
- Bulbar weakness: dysarthria, dysphagia (risk of aspiration)
- Ophthalmoplegia (especially in Miller-Fisher variant)
- Ptosis
Autonomic Nervous System (65% of AIDP patients):
- Cardiac arrhythmias (most dangerous - can cause sudden death)
- Blood pressure lability (hypertension and hypotension)
- Uncontrolled sweating
- Temperature dysregulation
- Ileus and bladder dysfunction
- Orthostatic hypotension
- Dysautonomia is a major source of ICU morbidity and can cause sudden cardiac arrest
Miller-Fisher Syndrome (MFS) Triad:
- Ophthalmoplegia (bilateral external ophthalmoplegia)
- Ataxia (cerebellar-type)
- Areflexia
- Facial weakness, ptosis, and pupillary abnormalities may also be present
- Nerve conduction velocities are normal (unlike AIDP)
[Goldman-Cecil Medicine, p. 4080-4082; Miller's Anesthesia, p. 12033]
Time Course
Day 0-14: Infection/trigger
Week 1-2: Symptom onset - weakness, sensory symptoms
Weeks 2-4: Progressive worsening - NADIR of disease
50% reach maximum disability within 2 weeks
75% within 3 weeks
>90% within 4 weeks
[5% progress to maximal loss within 72 hours!]
Week 4+: Plateau phase
Weeks 4-8: Beginning of recovery (spontaneous remyelination)
Months-Years: Full recovery (variable, may be prolonged)
Diagnostic Criteria
Required Features (Brighton Collaboration Criteria / Asbury & Cornblath)
- Progressive weakness of both legs and arms (bilateral)
- Areflexia or significant hyporeflexia
Supportive Clinical Features
- Progression over days to 4 weeks
- Relative symmetry of symptoms and signs
- Mild sensory symptoms or signs
- Bifacial palsies
- Autonomic dysfunction
- Absence of fever at onset (fever suggests alternative diagnosis)
- Recovery beginning 2-4 weeks after progression ceases
Laboratory Features Supportive of Diagnosis
1. CSF Analysis (Lumbar Puncture):
- Cytoalbuminologic (albuminocytologic) dissociation: elevated protein (often >45 mg/dL) with <10 WBCs/μL - this is the classical CSF finding
- CSF protein may be normal in the first 7-10 days of illness (up to 10% remain normal throughout)
- CSF WBC >50/μL should prompt evaluation for HIV seroconversion, Lyme disease, or meningitis - these suggest an alternative diagnosis
2. Electrodiagnostic Studies (Nerve Conduction Studies + EMG):
The most important tool for subtype classification and prognosis:
| Subtype | NCS Findings |
|---|---|
| AIDP | Slowed conduction velocities, prolonged distal latencies, F-wave delays, conduction block - demyelinating pattern |
| AMAN | Reduced compound muscle action potential (CMAP) amplitude with preserved conduction velocities; anti-GM1 antibodies |
| AMSAN | Reduced CMAP and sensory nerve action potential (SNAP) amplitudes - axonal degeneration |
| Miller-Fisher | Normal nerve conduction velocities |
Prognostic value: Axonal degeneration (reduced CMAP amplitudes in upper extremities) and GM1 antibodies predict poorer recovery.
3. Serum Antibody Testing:
- Anti-GQ1b: >85% sensitivity for Miller-Fisher syndrome
- Anti-GM1, anti-GD1a: AMAN subtype
- Helpful for classification but not required for treatment initiation
[Bradley & Daroff's Neurology, p. 2663; Goldman-Cecil Medicine, p. 4081]
Differential Diagnosis
Conditions that can mimic GBS and require exclusion:
| Warning Sign | Differential Diagnosis |
|---|---|
| Sensory predominant | Sensory neuronopathy |
| Prominent bowel and bladder dysfunction | Myelopathy (GBS spares sphincters early) |
| Spinal sensory level | Myelopathy, transverse myelitis |
| Persistently asymmetric weakness | Viral encephalomyelitis, mononeuritis multiplex (vasculitis), diabetic amyotrophy |
| Distal predominant pattern | Toxic neuropathy (arsenic, thallium) |
| Slow progression (>4 weeks) | CIDP (Chronic Inflammatory Demyelinating Polyneuropathy) |
| CSF WBC >50/μL | HIV seroconversion, Lyme disease, meningitis |
| Ophthalmoplegia, unreactive pupils, dry mouth | Botulism |
| Variable weakness; ptosis, diplopia | Myasthenia gravis |
| Tick bite | Tick paralysis |
Key distinguishing features of GBS vs. myelopathy: GBS has flaccid weakness + areflexia + sensory involvement WITHOUT a spinal level, bowel/bladder involvement is late, and CSF shows cytoalbuminologic dissociation (not pleocytosis).
[Goldman-Cecil Medicine, p. 4081]
Management
Hospitalization and Monitoring
All patients with confirmed or suspected GBS should be hospitalized due to the risk of rapid respiratory deterioration. The trajectory of respiratory function must be closely monitored.
Respiratory monitoring - the "20-30-40 rule" / key thresholds:
| Parameter | Action Threshold |
|---|---|
| Forced Vital Capacity (FVC) <20 mL/kg | Observe closely in ICU |
| FVC <15 mL/kg | Probable intubation needed |
| Maximum Inspiratory Pressure (MIP) < -30 cmH₂O | Consider intubation |
| Vital capacity <1 L | ICU ventilator support needed |
| Negative inspiratory force < -70 cmH₂O | Ventilator support likely needed |
Key point: Hypercarbia (raised PaCO₂) is a late and unreliable sign of respiratory failure in GBS - do not wait for it. Monitor serial FVC and clinical signs of fatigue.
Erasmus GBS Respiratory Insufficiency Score (EGRIS): A validated tool to predict which patients need early ICU admission, based on:
- Severity of limb weakness
- Timing of symptoms at presentation
- Bulbar symptoms
Early tracheostomy is appropriate in patients with identifiably prolonged respiratory failure.
Autonomic monitoring: ECG monitoring and blood pressure monitoring are essential given the risk of cardiac arrhythmia and BP lability from dysautonomia.
[Goldman-Cecil Medicine, p. 4081; Miller's Anesthesia, p. 12035]
Specific Immunotherapy
Treatment should be initiated within 2 weeks of symptom onset.
1. Intravenous Immunoglobulin (IVIG) - Preferred
- Dose: 2 g/kg total, divided over 2 days (or longer if cardiac function or fluid status requires it)
- Mechanism: Suppresses immune responses through multiple mechanisms including Fc receptor blockade, complement inhibition, modulation of T and B cell function
- Preferred over plasmapheresis because patients are significantly more likely to complete a full course
- A second dose of IVIG does not improve outcomes and increases complication risk - do not repeat
2. Therapeutic Plasma Exchange (Plasmapheresis) - Equally Effective
- 5 plasma volumes exchanged over 10 days
- Removes circulating autoantibodies and inflammatory mediators
- Equally effective to IVIG (no randomized trial has shown superiority of either)
- Many physicians try them sequentially if the first treatment fails
- Less preferred because it requires vascular access and more patient compliance
3. Corticosteroids - NOT Recommended
- Methylprednisolone 500 mg/day for 5 days plus IVIG shows a slight initial advantage but no long-term benefit over IVIG alone
- Steroids alone do not improve outcomes
- Given the risks, corticosteroids are generally not recommended for GBS
4. Newer Agents
- Interferon has not been shown to improve outcomes
- Newer immune modulation drugs (e.g., eculizumab, IgG-Fc receptor blockers) are currently in clinical trials
Miller-Fisher Syndrome: Prognosis is generally excellent. There is controversy about whether IVIG or plasma exchange is necessary - the condition often resolves spontaneously.
[Goldman-Cecil Medicine, p. 4081; Miller's Anesthesia, p. 12035-12036]
ICU and Supportive Care
Comprehensive supportive care is critical for outcomes and includes:
| Domain | Management |
|---|---|
| Respiratory | Serial FVC monitoring; early intubation when thresholds met; early tracheostomy for prolonged failure |
| Cardiovascular | Continuous cardiac monitoring; cautious treatment of BP lability (avoid large swings); temporary pacing for bradyarrhythmias |
| DVT prophylaxis | LMWH + compression devices in immobile patients |
| Nutrition | Enteral feeding (NGT or PEG if prolonged); maintain euglycemia |
| Bladder | Urinary catheter for bladder dysfunction |
| Bowel | Bowel care; prokinetics for ileus |
| Pain | Deafferentation pain is severe, truncal - treat with anticonvulsants (gabapentin, carbamazepine) rather than opioids |
| Rehabilitation | Early physiotherapy and mobilization |
| Psychological | Treatment for depression (very common in cognitively intact, paralyzed patients); psychosocial support |
| Succinylcholine | AVOID - risk of lethal hyperkalemia from upregulated extrajunctional acetylcholine receptors; use non-depolarizing NMBAs with caution |
Pain in GBS: Deafferentation pain is severe, truncal in distribution, and often magnified by immobility, boredom, and depression. Anticonvulsants are more effective than opioids.
Anesthetic considerations: Succinylcholine is absolutely contraindicated in GBS (even in recovered patients, the upregulation of extrajunctional ACh receptors persists and can cause fatal hyperkalemia). Non-depolarizing neuromuscular blockers should be used with caution due to altered sensitivity.
[Miller's Anesthesia, p. 12035-12036]
Prognosis
| Timeline | Clinical Milestone |
|---|---|
| 2 weeks | 50% of patients reach maximum disability |
| 3 weeks | 75% reach maximum disability |
| 4 weeks | >90% reach maximum disability (nadir) |
| 4-8 weeks | Plateau, then gradual recovery begins |
| 6 months | Mortality ~3% (mainly elderly/severely affected) |
| Long-term | 80% recover completely or with minor sequelae; 20% have persistent disability |
Poor prognostic indicators:
- Older age
- Preceding diarrheal illness (C. jejuni infection)
- Axonal variant (AMAN/AMSAN)
- Need for mechanical ventilation (mortality increases to ~14.3%)
- Reduced CMAP amplitudes in the upper extremities (significant axonal loss)
- Presence of anti-GM1 antibodies
- Severity of weakness at nadir
Good prognostic indicators:
- Young age
- Respiratory and upper limb infection as trigger (vs. diarrheal illness)
- Demyelinating pattern (AIDP - remyelination is more complete)
- Milder weakness at presentation
- Anti-GQ1b antibodies (MFS has excellent prognosis)
[Goldman-Cecil Medicine, p. 4082]
Comparison: GBS vs. CIDP
| Feature | GBS (Acute) | CIDP (Chronic) |
|---|---|---|
| Onset | Acute, monophasic | Chronic, progressive or relapsing-remitting |
| Progression | Peaks at ≤4 weeks | Progresses >2 months |
| Recovery | Usually complete/near-complete | Incomplete; relapses common |
| CSF | Cytoalbuminologic dissociation | Similar (elevated protein, low cells) |
| Treatment | IVIG or plasmapheresis (acute course) | IVIG, plasmapheresis, corticosteroids (effective, unlike GBS) |
| Association | HIV, paraproteinemia less common | HIV, lymphoid neoplasms, paraproteinemias more common |
Unlike GBS, corticosteroids are effective in CIDP and are a mainstay of long-term treatment.
[Robbins & Kumar Basic Pathology, p. 475]
Summary: Key Teaching Points
- GBS is the most common cause of acute flaccid paralysis worldwide in the post-polio era
- The classic CSF finding is cytoalbuminologic dissociation (high protein, <10 WBCs) - but may be normal in the first 7-10 days
- Areflexia is virtually universal and required for diagnosis
- Respiratory failure occurs in 20-30% - monitor FVC closely; don't wait for hypercarbia
- IVIG (2 g/kg) is the preferred treatment - equally effective to plasmapheresis but better tolerated; start within 2 weeks of onset
- Corticosteroids do not help in GBS (contrast with CIDP where they work)
- Autonomic dysfunction (in 65%) is life-threatening - continuous cardiac monitoring is mandatory
- Succinylcholine is absolutely contraindicated - risk of fatal hyperkalemia
- Anti-GQ1b antibodies are highly specific for Miller-Fisher syndrome
- Pain (deafferentation) is common, severe, and responds to anticonvulsants better than opioids
- Most patients recover, but 20% are left with significant disability; axonal subtypes have worse outcomes
Sources: Goldman-Cecil Medicine International Edition | Bradley & Daroff's Neurology in Clinical Practice | Miller's Anesthesia, 10th Ed | Robbins & Kumar Basic Pathology | Adams & Victor's Principles of Neurology, 12th Ed
This is a shared conversation. Sign in to Orris to start your own chat.