Effects of exercise on cardiac output. Refer, uh, Sembulingham book.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the material needed. Now let me compose a thorough answer structured along Sembulingam-style physiology topics.
Note: The library does not contain K. Sembulingam's Essentials of Medical Physiology directly. The answer below is drawn from Guyton & Hall (13th ed.) - the closest authoritative equivalent in the library - and is aligned with the content Sembulingam covers on this topic (the two books agree closely on exercise physiology of cardiac output).
Effects of Exercise on Cardiac Output
Overview
Exercise places the greatest demands on circulatory function. The primary cardiovascular response is a large, graded increase in cardiac output - roughly proportional to the intensity of exercise. This is just as important as muscle strength in determining exercise capacity: marathon runners who can raise their cardiac output the most typically set the best times.
Magnitude of Increase
| Condition | Cardiac Output (L/min) |
|---|---|
| Young man at rest | 5.5 |
| Maximal - untrained young man | ~23 |
| Maximal - average male marathoner | ~30 |
| Maximal - elite marathoners | 35-40 |
- An untrained person can increase cardiac output ~4-fold above resting.
- A well-trained athlete can increase it ~6-fold (up to 7-8x in elite marathoners).
Mechanisms Responsible for the Increase
1. Increased Heart Rate (Chronotropy)
- Sympathetic stimulation raises heart rate to 170-190 beats/min (up from ~75 at rest).
- This is by far the dominant factor - heart rate increases ~270% while stroke volume increases only ~50%.
- Heart rate continues to rise even after stroke volume plateaus.
2. Increased Stroke Volume (Inotropy)
- Sympathetic stimulation increases cardiac contractility, raising stroke volume from ~75 mL to ~110 mL (untrained) or up to 162 mL (marathoner).
- Enhanced venous return increases preload (Frank-Starling mechanism).
- Stroke volume reaches its maximum by the time cardiac output has increased only halfway to its maximum - beyond that, further increases depend entirely on heart rate.
3. Increased Venous Return
Two mechanisms raise venous return during exercise:
a) Increased mean systemic filling pressure
- Sympathetic venoconstriction squeezes blood out of the venous capacitance vessels.
- Contraction of abdominal and skeletal muscles compresses internal vessels.
- Mean systemic filling pressure rises from the normal 7 mm Hg up to ~30 mm Hg during maximal exercise.
b) Decreased venous resistance
- Vasodilation in active skeletal muscles (from local metabolites: CO₂, lactic acid, K⁺, adenosine) reduces peripheral resistance.
- This rotates the venous return curve upward - more blood flows back to the heart per unit of right atrial pressure.
Together, these two effects shift the venous return curve upward and to the right.
Graphic Analysis (Guyton Diagram)
The equilibrium shifts from Point A (rest: ~5 L/min) to Point B (heavy exercise: ~21+ L/min). Despite the huge increase in output, right atrial pressure rises only minimally (~1.5 mm Hg) because the venous return curve shifts up simultaneously with the cardiac output curve.
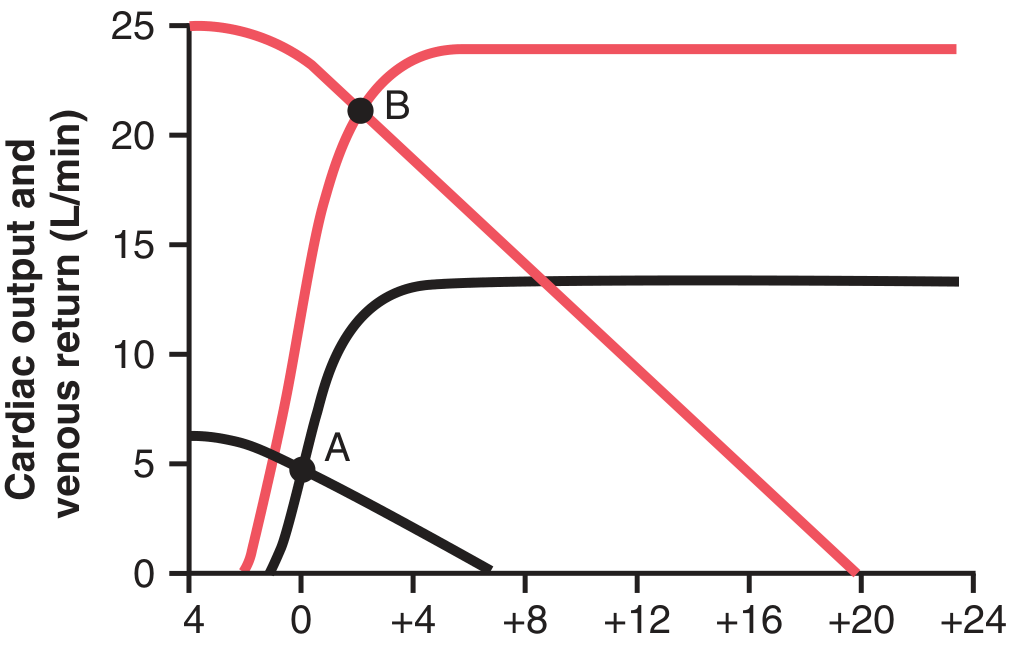
Without sympathetic augmentation of the cardiac output curve, maximum CO could only rise ~2.5-fold. Without changes in the venous return curve (upper plateau ~6 L/min normally), CO could hardly rise at all.
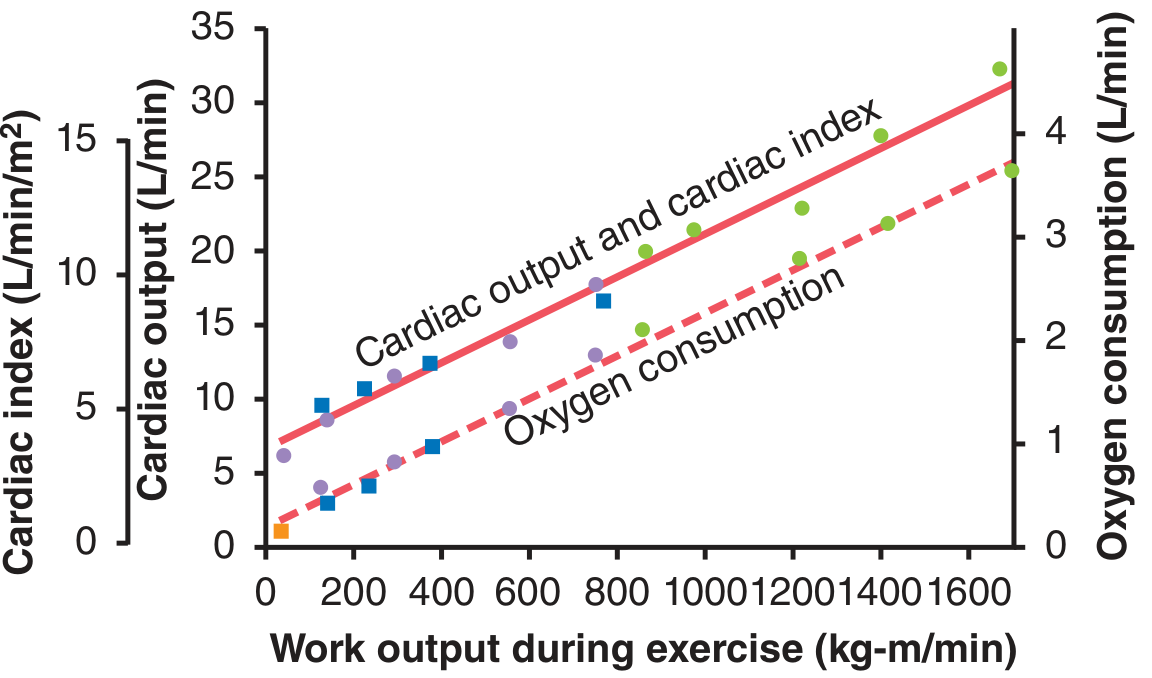
Cardiac Output vs. Work Output and O₂ Consumption
All three - work output, oxygen consumption, and cardiac output - are linearly related during exercise. Greater muscle work → more O₂ demand → metabolic vasodilation in muscle → increased venous return → increased cardiac output.
Role of Stroke Volume vs. Heart Rate
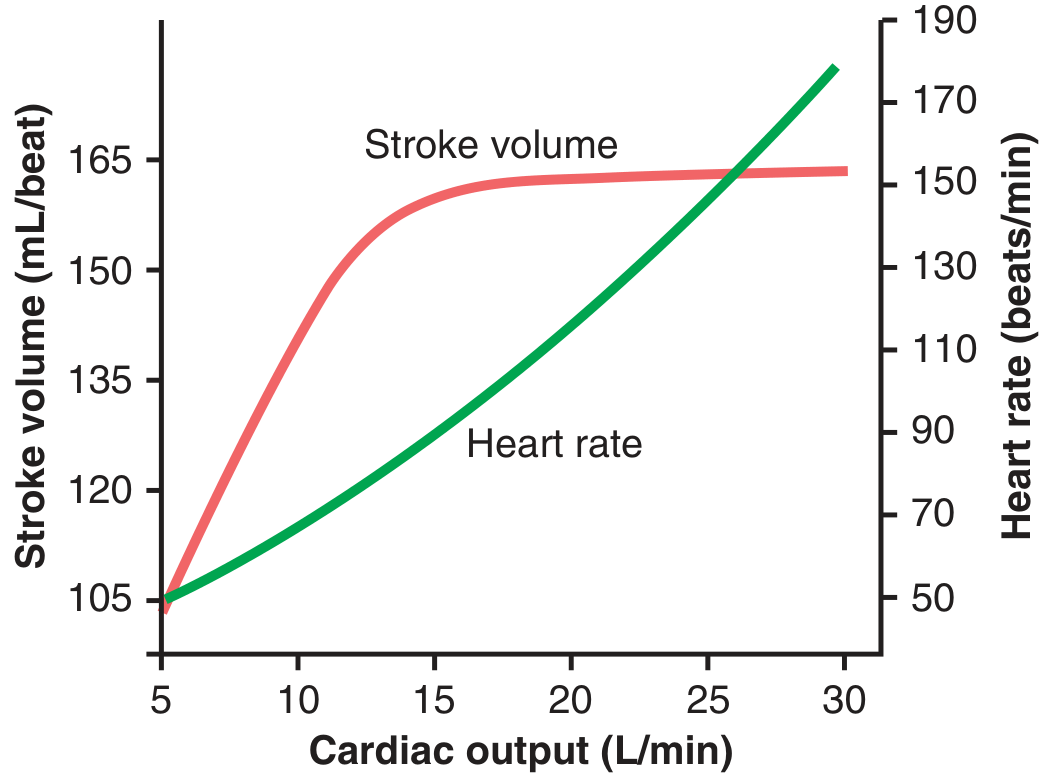
- Stroke volume: increases from 105 → 162 mL (~50% increase), then plateaus.
- Heart rate: increases from 50 → 185 beats/min (~270% increase) - the dominant driver.
- At maximal exercise, both HR and SV are at ~95% of their respective maximums, so cardiac output is ~90% of its maximum.
Cardiovascular System as the Limiting Factor
The cardiovascular system (not the respiratory system) limits VO₂max. At maximal exercise, cardiac output is at ~90% of maximum vs. pulmonary ventilation at only ~65% of maximum. The heart's ability to pump is therefore the most critical bottleneck in oxygen delivery to exercising muscles.
Effect of Athletic Training
| Stroke Volume (mL) | Heart Rate (beats/min) | |
|---|---|---|
| Resting - nonathlete | 75 | 75 |
| Resting - marathoner | 105 | 50 |
| Maximum - nonathlete | 110 | 195 |
| Maximum - marathoner | 162 | 185 |
- Endurance training causes cardiac hypertrophy: chamber volume and heart mass increase ~40%.
- Resting cardiac output is the same in trained vs. untrained persons, but in athletes it is achieved at a lower heart rate with higher stroke volume (athlete's bradycardia).
- The 40% greater maximal cardiac output in marathoners is the principal reason for their superior athletic performance.
- This hypertrophy occurs mainly with endurance training, not sprint training.
Source: Guyton and Hall Textbook of Medical Physiology (13th ed.), Chapters 21 & 85 - the Sembulingam text covers the same physiology with largely identical values and mechanisms.
This is a shared conversation. Sign in to Orris to start your own chat.