Gait
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have enough comprehensive data to write an authoritative answer. Let me compile it.
Orthopedic/Musculoskeletal Gait
The Gait Cycle
The gait cycle is the interval from initial contact (heel strike) of one foot to the next ipsilateral initial contact - i.e., one complete stride. It is divided into two primary phases:
| Phase | Duration | Description |
|---|---|---|
| Stance | ~60% of cycle | Foot is in contact with the ground (weight-bearing) |
| Swing | ~40% of cycle | Foot is off the ground (non-weight-bearing) |
During normal walking, there are two periods of double-limb support (both feet on the ground simultaneously), totalling 20-30% of the cycle - a key distinction from running, which eliminates double-limb support entirely and introduces a float phase (neither foot on the ground). Running also shortens the cycle time but greatly increases ground reaction forces.
Key spatial/temporal terms:
- Step - distance between successive initial contacts by the two lower limbs
- Stride - distance between successive initial contacts by the same limb (= two steps)
- Cadence - steps per unit time
- Velocity - distance/time
Stance Phase (60%) - Subdivisions
The stance phase is subdivided into five components (Perry's classification):
-
Heel Strike / Initial Contact (IC) - heel contacts the ground; foot is dorsiflexed; tibialis anterior contracts eccentrically to guide the forefoot to the ground. The subtalar joint is everted, unlocking the transverse tarsal joint to allow shock absorption in the transverse plane.
-
Loading Response (LR) - begins with IC and ends with initial swing of the contralateral foot. Early knee flexion of ~15° dampens the impact. Quadriceps act eccentrically to control this flexion.
-
Midstance (MSt) - begins with initial swing of the advancing (contralateral) foot; ends when the body's center of gravity is directly over the supporting forefoot. Single-limb support phase. Gluteus medius contracts eccentrically to control pelvic tilt.
-
Terminal Stance (TSt) - begins with heel rise; ends with IC of the contralateral foot. Ankle plantarflexors and toe flexors contract to raise the heel. The subtalar joint inverts, locking the transverse tarsal joint - converting the midfoot from flexible to rigid to allow propulsion.
-
Pre-swing (PSw) - begins with IC of the contralateral limb; ends when the stance foot lifts off. Maximum subtalar inversion and maximal rigidity at toe-off.
Swing Phase (40%) - Subdivisions
-
Initial Swing (ISw) - begins immediately after toe-off. Hip flexors contract concentrically to propel the limb forward. Ends at maximal knee flexion.
-
Mid-swing - dorsiflexors contract to clear the foot from the ground (foot clearance is critical - failure causes foot drop/steppage gait).
-
Terminal Swing (TSw) - hamstrings contract eccentrically to decelerate the advancing limb and prepare for heel strike. Ends at foot contact.
Gait Dynamics and Determinants
The body's center of mass (2 cm anterior to S2) follows a sinusoidal path with:
- Vertical displacement amplitude: ~5 cm
- Lateral displacement amplitude: ~6 cm
Six determinants minimize displacement of the center of mass, reducing energy expenditure:
| Determinant | Mechanism |
|---|---|
| Pelvic rotation | Pelvis externally rotates at IC, internally at preswing - minimizes vertical displacement needed for limb advancement |
| Pelvic list (tilt) | Non-weight-bearing side drops ~5°, reducing superior deviation |
| Knee flexion at loading | 15° flexion dampens impact at initial loading |
| Foot and ankle motion | Subtalar joint damping at loading response |
| Knee motion | Reduces abrupt changes in center of mass |
| Lateral pelvic displacement | Shifts center of mass over stance limb |
Muscle Action During Gait
| Muscle | Contraction Type | Function |
|---|---|---|
| Gluteus medius | Eccentric | Controls pelvic tilt (midstance) |
| Gluteus maximus | Concentric | Powers hip extension |
| Iliopsoas | Concentric | Powers hip flexion (swing) |
| Hip adductors | Eccentric | Control lateral sway (late stance) |
| Quadriceps | Eccentric | Stabilizes knee at IC and preswing |
| Hamstrings | Eccentric | Controls rate of knee extension in swing; decelerates limb at terminal swing |
| Tibialis anterior | Eccentric (primary) | Slows plantarflexion rate at IC; dorsiflexes ankle in swing for foot clearance |
| Gastrocnemius-soleus | Eccentric | Slows dorsiflexion rate during stance; propulsion at terminal stance |
Pathological Gait Patterns
Clinical Assessment
Ask the patient to stand (inspect from front, side, and back), then walk using any aids. Observe head position, cadence, symmetry, and foot progression angle.
| Gait Type | Cause | Mechanism | Clinical Features |
|---|---|---|---|
| Antalgic | Hip/knee/foot arthritis, any painful limb | Shortened stance phase on painful side to minimize loading time | Head dips on painful side; cadence asymmetric (dot/dash pattern); rapid swing of unaffected limb |
| Trendelenburg (abductor lurch) | Weakness of hip abductors (gluteus medius/minimus) - OA hip, DDH, post-THR | Abductors cannot hold pelvis level during single-limb stance; pelvis drops to contralateral side | Trunk lurches toward the affected side to bring center of gravity over the femoral head and reduce abductor demand |
| Trendelenburg sign | Same as above | Standing on one limb - pelvis drops on the contralateral (lifted) side | Positive sign = pelvis drops on unsupported side |
| High-stepping / Steppage | Foot drop - common peroneal nerve palsy, L4/L5 radiculopathy | Loss of dorsiflexion prevents foot clearance in swing; hip/knee over-flex to lift foot | High steppage; foot slap at heel strike |
| Varus thrust | Lateral compartment OA / ligamentous laxity | Knee collapses into increased varus during loading response | Visible lateral thrust of knee; associated with lateral compartment OA |
| Crouch gait | Hamstring contracture, spastic diplegia, quadriceps weakness, plantar flexor weakness | Excessive knee and hip flexion throughout stance | Excessively flexed knees and hips during stance; increased energy expenditure |
| Equinus gait | Achilles contracture, spastic equinus, tibialis anterior weakness | Fixed plantarflexion prevents heel strike | Toe-first or forefoot initial contact |
| Stiff gait | Hip arthrodesis, severe hip/knee stiffness | Compensatory trunk and lumbar motion | Head rocks forward and back to compensate for restricted hip motion |
| Scissor gait | Spastic diplegia (cerebral palsy) | Hip adductor spasticity causes limbs to cross midline | Knees cross during swing; narrow base, internal rotation |
| Incoordinated gait | Cerebellar ataxia, cerebral palsy | Disrupted motor coordination | No regular cadence; wide base; head movement lacks coordination |
Intoeing and Pediatric Gait
Intoeing = negative foot progression angle. It results from one or more torsional anomalies:
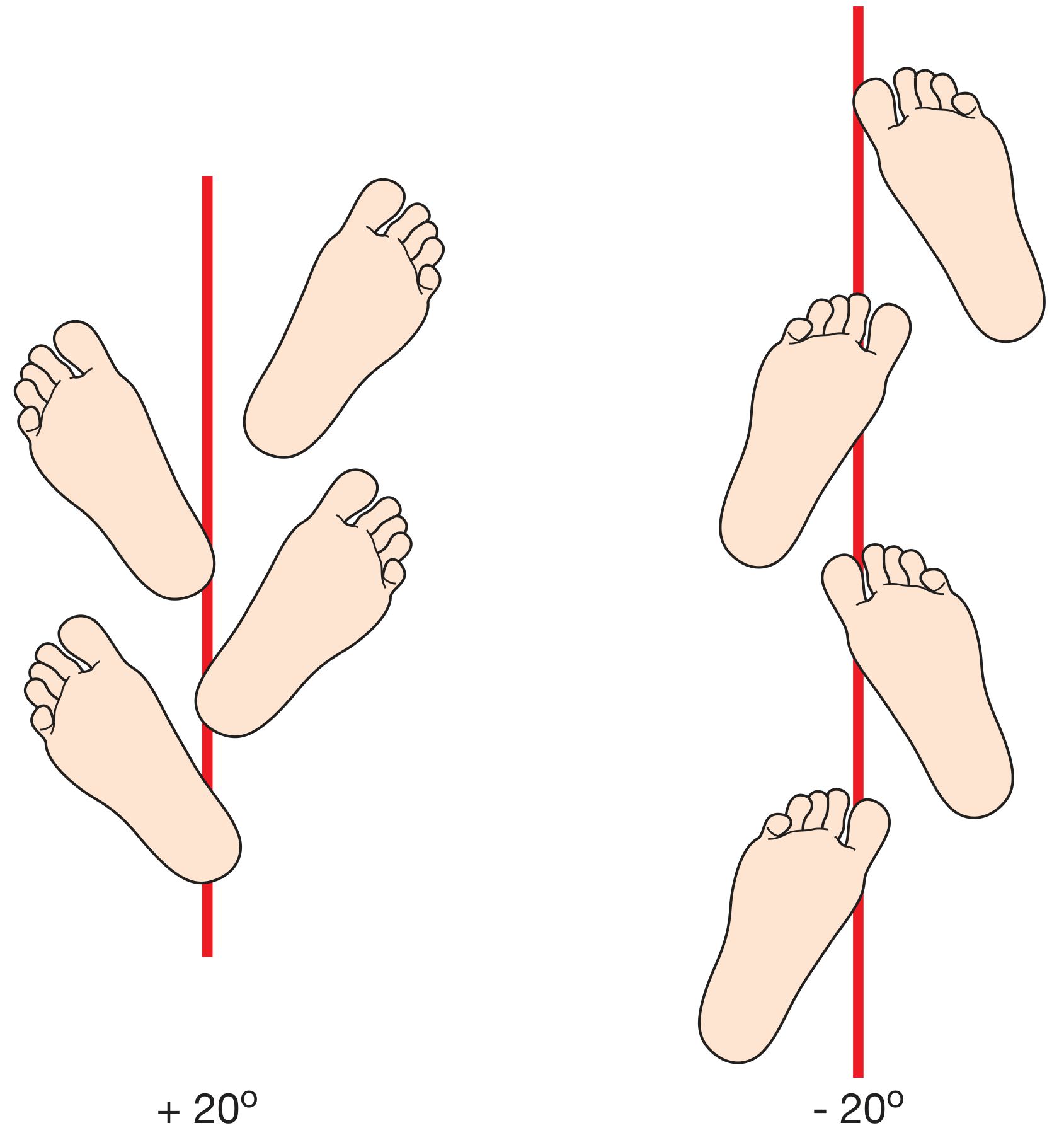
Foot progression angle: toes-out (+20°) on left vs. toes-in (-20°) on right
| Level | Cause | Assessment | Natural History |
|---|---|---|---|
| Femur/Hip | Persistent femoral neck anteversion | Excessive IR at hip (prone); Craig's test | Most resolve; osteotomy if severe after age 10-12 with functional difficulty |
| Tibia | Internal tibial torsion | Thigh-foot angle (prone) | Resolves by age 4 with normal tibial rotation |
| Foot | Metatarsus adductus | Flexible vs. rigid forefoot adduction | Usually corrects by age 2-4; casting for rigid cases |
Compensatory external tibial torsion may develop alongside femoral anteversion, normalizing the foot progression angle but producing "miserable malalignment syndrome" - knee pain and instability.
Ground Reaction Force (GRF) and Clinical Relevance
The GRF is the mean load-bearing vector that changes in both magnitude and direction throughout the gait cycle. It determines the moment (torque) across each joint, which drives muscle demand. This is directly relevant to:
- Knee OA - a high external knee adduction moment (KAM) = increased medial compartment loading; varus alignment exacerbates this
- Hip OA / after THR - a shortened lever arm from valgus coxa or leg shortening increases the abductor force required to prevent pelvic drop
- Foot orthotics - modify subtalar and forefoot GRF distribution
Sources:
- Miller's Review of Orthopaedics, 9th Ed., Ch. 10 (Gait, pp. 864-867)
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 35 & 41 (Gait examination, Biomechanics)
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3, Ch. 23 (Gait cycle, pp. 3162-3169)
- Campbell's Operative Orthopaedics, 15th Ed. 2026 (Inspection of gait)
This is a shared conversation. Sign in to Orris to start your own chat.