Distraction osteogenesis what's this principle uses and application of it and everything related to it for 10 marks question with appropriate illustrative images and diagrams
Reading File
Finding Sources
Searching the Web
distraction osteogenesis principle mechanism applications clinical uses
Searching Images
distraction osteogenesis principle mechanism diagram
Reading File
Reading File
Searching Images
distraction osteogenesis phases latency distraction consolidation bone regenerate histology
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching Images
Ilizarov external fixator limb lengthening bone transport tibia
Loading Image
Loading Image
I now have all the information needed for a comprehensive 10-mark answer. Let me compile it.
Distraction Osteogenesis — Comprehensive 10-Mark Answer
Definition
Distraction osteogenesis (DO) is the mechanical induction of new bone formed between bony surfaces that are gradually separated by controlled mechanical forces following a controlled fracture (osteotomy/corticotomy). Ilizarov described the underlying law as the "Tension-Stress Effect": living tissues under slow, steady tension stress become metabolically activated, generating new cellular mass and tissue matrix.
"Distraction osteogenesis is the mechanical induction of new bone that occurs between bony surfaces that are gradually pulled apart." — Rockwood and Green's Fractures in Adults, 10th ed.
Historical Background
- Codivilla (1905): First described leg lengthening using traction
- Ilizarov (1950s–1960s): Russian orthopaedic surgeon who systematically developed and popularized the technique using circular ring fixators (the Ilizarov apparatus). His work with limb lengthening in Soviet soldiers with war injuries laid the scientific foundation.
- Distraction osteogenesis was first applied to the craniofacial skeleton over 80 years ago, coming into widespread clinical use only in the past 25 years.
Biological Principle (Tension-Stress Effect)
Mechanism at the Cellular Level
When bone is gradually distracted:
- Fibroblast-like cells in the regenerate zone develop an elongated shape, oriented parallel to the tension vector
- Collagen fibers align parallel to the distraction direction
- Fibroblastic cells transform into osteoblasts, depositing osteoid on these collagen fibers
- Osteoblasts further differentiate into osteocytes within the bone matrix
- New bone grows both proximally and distally from a central growth region — the interzone (fibrous zone)
- The process occurs by direct intramembranous ossification (not endochondral) when there is stable fixation, omitting the cartilaginous phase
Neovascularization
- Fibroblast precursors cluster around sinusoidal capillaries
- Tension stress drives rapid new capillary growth, producing a dense longitudinally-oriented vascular network
- The regenerate gap is highly vascular — each longitudinal collagen column is surrounded by large vascular channels
- This intense neovascularization extends to surrounding soft tissues as well
The "Physis-Like" Structure
New bone forms in parallel columns extending in both directions from the central interzone — structurally mimicking a growth plate (physis). This is why the regenerate resembles physeal growth cartilage histologically.
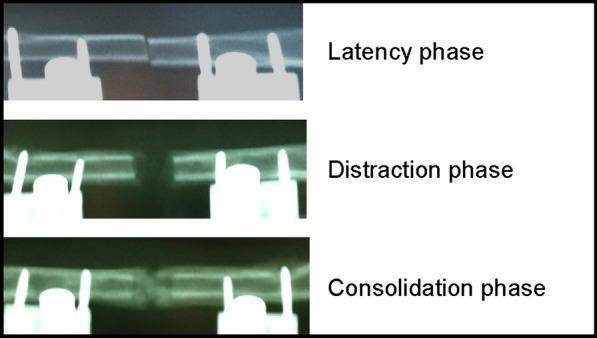
Phases of Distraction Osteogenesis
Phase 1: Latency (Lag) Period
- Duration: 5–7 days in adults; as short as 24 hours in neonates/infants
- Osteotomy/corticotomy is performed; distractor is placed but not activated
- Wound healing begins; callus forms at the osteotomy site
- Periosteal and endosteal regenerative cells proliferate
- Purpose: allow initial granulation tissue and callus bridge before active distraction
Phase 2: Distraction (Active) Phase
- Distractors are gradually activated at 1 mm/day (Ilizarov's recommended rate)
- Achieved in ≥4 increments/day (rhythm) — continuous distraction over 24 h is ideal
- Too slow (≤0.5 mm/day) → premature consolidation, locking distractors
- Too fast (≥2 mm/day) → disruption of vascular channels, cyst formation, fibrous non-union
- New immature woven bone is laid down between the separated bony edges
- Soft tissues (skin, muscle, nerves, vessels) adapt to the lengthening
Phase 3: Consolidation Phase
- Active distraction stops; desired length is achieved
- Distractor remains in place (hardware not removed)
- Woven bone mineralizes → remodels to lamellar bone
- Rule of thumb: consolidation period = at least twice the duration of the distraction phase
- Soft tissues continue remodelling and reorienting
- After several months, the regenerated bone is similar in volume to native bone, though with somewhat reduced mineral content initially
Surgical Technique
Corticotomy vs. Osteotomy
- Corticotomy (preferred by Ilizarov): low-energy technique — cortices are osteotomized with a small drill/osteotome, preserving the periosteum and medullary canal (intramedullary blood supply and marrow intact)
- Anterior, anterolateral, and anteromedial cortices are cut, then the posterior cortex is closed osteoclasis — this maximises periosteal preservation
- Osteotomy: complete bone cut (used when corticotomy impossible)
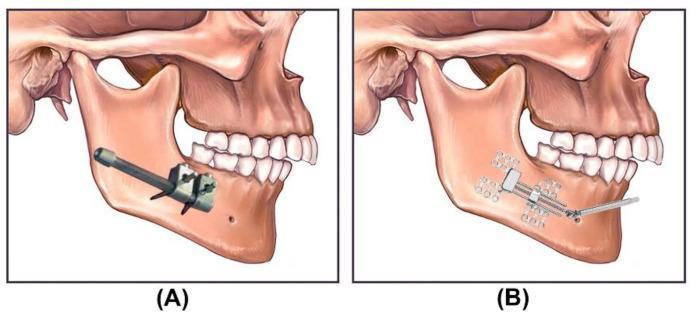
Device Placement
- Fixation screws/pins are inserted on both sides of the osteotomy
- Internal devices: anchored with plates and screws; no external bulk; less vector control
- External devices: percutaneous pins; allow 3D vector control; more bulky
Types of Distractors
| Feature | Internal | External |
|---|---|---|
| Bulk | Minimal | Significant |
| Scar | Intraoral/hidden | Pin migration scars |
| Vector control | Limited | 3D control possible |
| Removal | Requires second surgery | Removed non-operatively |
| Application | Craniofacial, mandible | Limbs, craniofacial |
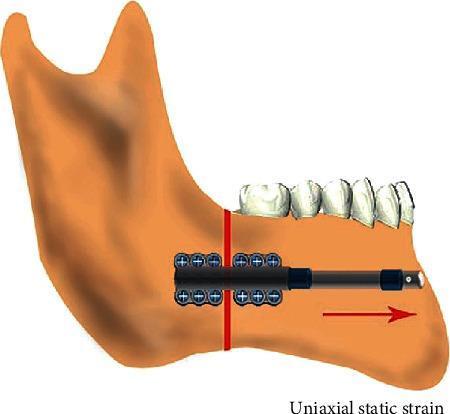
Special Designs
- Monolateral fixators: uniaxial distraction; simpler; used for straightforward lengthening
- Ilizarov ring fixators: circular rings + transfixion wires; allow multiplanar correction and weight bearing
- Hexapod fixators (Taylor Spatial Frame): 6-strut design enabling simultaneous correction in all 6 axes; computer-software driven
- Motorized intramedullary lengthening nails (PRECICE, STRYDE): eliminate external fixator entirely; patient-controlled via external remote
Applications
1. Orthopaedic Surgery
Limb Lengthening
- Limb length discrepancy (LLD): primary indication; discrepancies >2 cm are candidates
- Skeletal dysplasias (achondroplasia, hypochondroplasia): femoral and tibial lengthening
- Post-traumatic shortening: after physeal injury, fracture malunion, or growth arrest
- Lengthening is typically performed in the femur or tibia

Bone Transport (Intercalary Reconstruction)
- For large segmental bone defects (post-infection, post-tumour resection, osteomyelitis, trauma)
- A corticotomy is made away from the defect; the transported segment is slowly moved across to fill the gap ("docking")
- Can be performed with monolateral or Ilizarov ring fixators, or newer internal transport nails

Deformity Correction
- Angular and rotational deformities (e.g., tibial varus, genu varum/valgum)
- Hexapod fixators allow multiplanar simultaneous correction
Non-Union Treatment
- Hypertrophic non-unions can be compressed across the fixator; atrophic non-unions benefit from bone transport
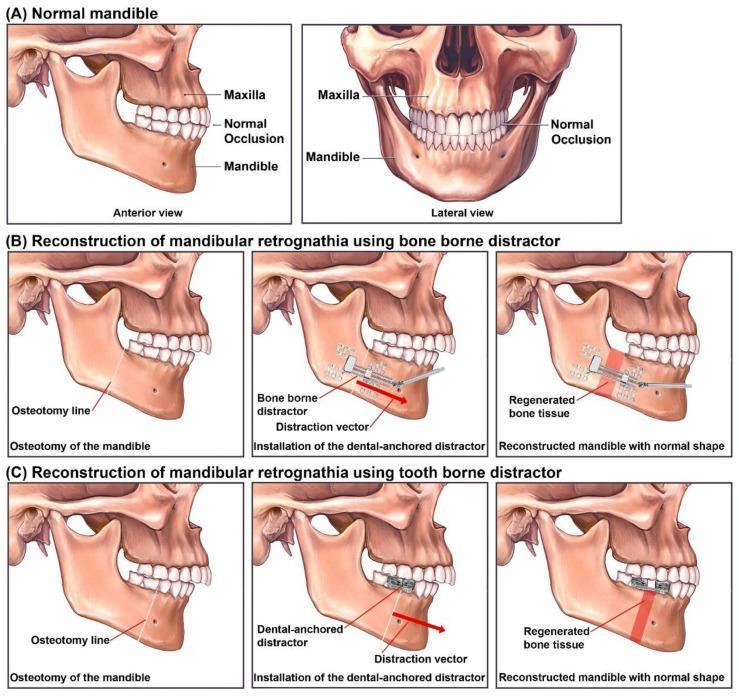
2. Craniofacial / Oral & Maxillofacial Surgery
Mandibular Distraction
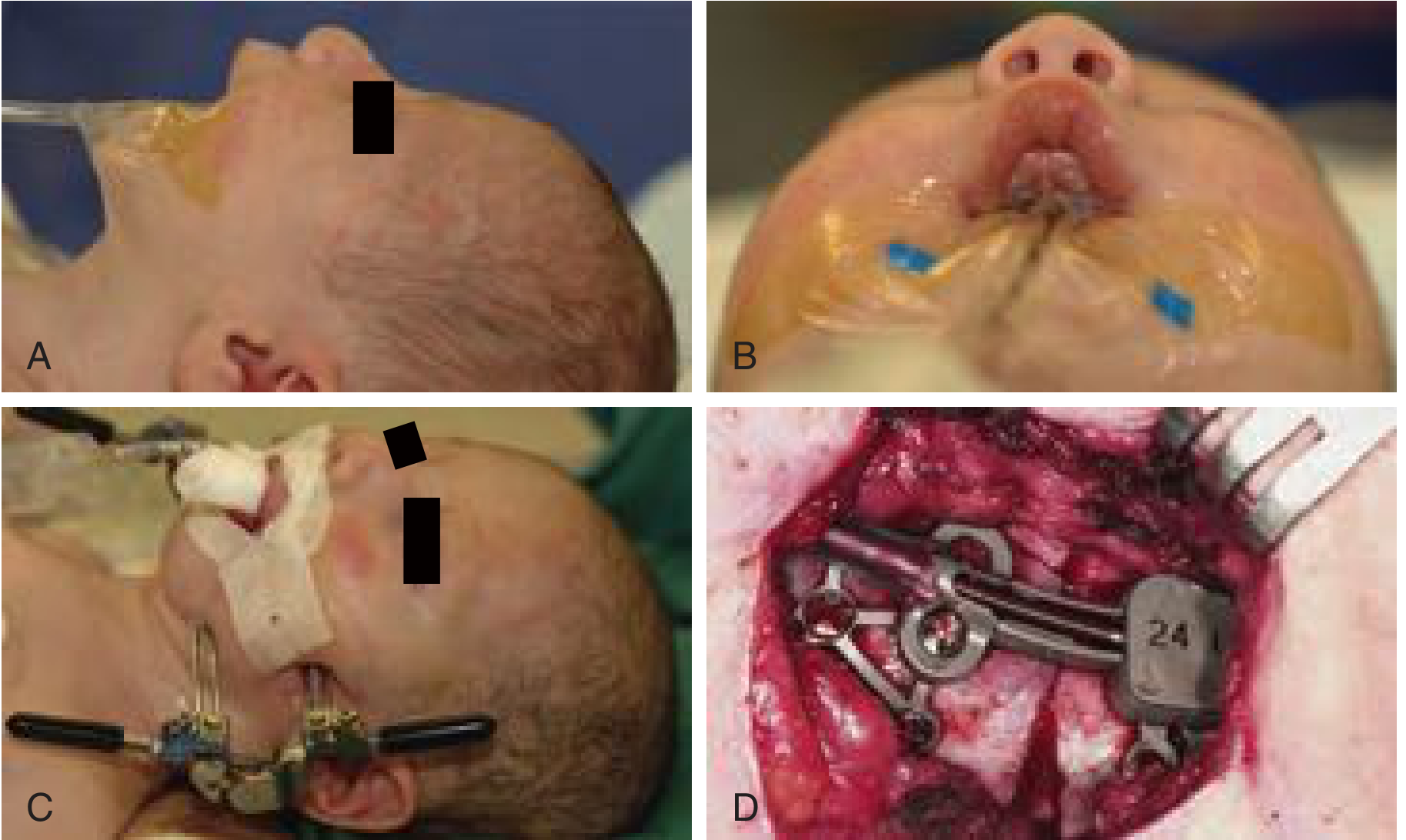
- Pierre Robin sequence: neonates with severe micrognathia causing airway obstruction and glossoptosis — mandibular DO can eliminate the need for tracheostomy
- Hemifacial microsomia: unilateral mandibular hypoplasia
- Mandibular retrognathia: bilateral mandibular advancement
Midfacial / Craniofacial Advancement
- Syndromic craniosynostosis (Crouzon, Apert): posterior cranial vault distraction (PCVD) achieves 20–40 mm of advancement vs. only 10–15 mm with conventional fronto-orbital advancement (FOA)
- Le Fort III / Monobloc advancement with internal distractors for midface hypoplasia
- Alveolar bone reconstruction: for dental implant site preparation
3. Other Applications
- Metacarpal/phalangeal lengthening: digital stump lengthening after amputation, for prosthesis fitting
- Vertical alveolar ridge augmentation (dental implantology)
- Calvarial vault reconstruction
- Transport DO for osteomyelitis: removes infected bone while simultaneously reconstructing
Advantages of Distraction Osteogenesis
- Simultaneous soft tissue expansion: skin, muscle, nerves, and vessels adapt concurrently — no need for large flaps or separate tissue expanders
- No donor site morbidity: no bone graft harvesting
- Larger advancements possible: up to 40 mm vs. 10–15 mm with acute osteotomy
- Neovascularization: the regenerate is highly vascular
- Reduced operative time and blood loss vs. traditional techniques
- Safe in infants and children: attractive for craniofacial anomalies
- 3D correction: vectors can be manipulated to correct angulation, translation, and rotation simultaneously
- Gradual soft tissue adaptation: reduces risk of airway compromise or vascular injury
Complications
Local Complications
| Complication | Cause/Feature |
|---|---|
| Pin-site infection | Most common; superficial (50%) or deep/osteomyelitis; prevented by good technique |
| Premature consolidation | Rate too slow or incomplete osteotomy; treat by re-corticotomy |
| Delayed consolidation / non-union | Rate too fast; poor vascular supply; smoking |
| Axial deviation | Eccentric pin placement; muscle imbalance |
| Joint contracture | Soft tissue tethering during lengthening (e.g., hip flexion in femoral lengthening) |
| Nerve palsy | Stretch injury (peroneal nerve in tibial lengthening) |
| Refracture | Premature removal of fixator before consolidation complete |
| Vessel injury | Rare; from wire/pin placement |
Systemic Complications
- Psychological morbidity from prolonged fixator wear
- Device malfunction / broken pins or wires
Key Parameters (Ilizarov's Rules)
| Parameter | Optimal Value |
|---|---|
| Rate of distraction | 1 mm/day |
| Rhythm (frequency) | ≥4 increments/day (0.25 mm each) |
| Latency period | 5–7 days (adults); 24 h (neonates) |
| Consolidation period | ≥2× distraction period |
| Corticotomy type | Low-energy, periosteum-preserving |
Summary Table
| Aspect | Detail |
|---|---|
| Principle | Tension-stress effect (Ilizarov) — tension drives intramembranous new bone formation |
| Bone formation mode | Intramembranous ossification (not endochondral) when stable fixation maintained |
| Regenerate structure | Parallel bone columns growing from central fibrous interzone (physis-like) |
| Phases | Latency → Distraction → Consolidation |
| Key advantage | Simultaneous bone + soft tissue generation, no graft needed |
| Main orthopaedic use | Limb lengthening, bone transport, deformity correction |
| Main craniofacial use | Mandibular DO (Pierre Robin, hemifacial microsomia), midfacial advancement |
| Main complication | Pin-site infection (most common) |
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. (2025) — Biology of Distraction Osteogenesis, Bone Transport
- Cummings Otolaryngology Head and Neck Surgery — Craniofacial Distraction Osteogenesis
This is a shared conversation. Sign in to Orris to start your own chat.