Breathlessness how to differentiate weather it is cardiac or respiratory
Reading File
Finding Sources
Finding Sources
Searching PubMed
dyspnea cardiac respiratory differentiation diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized response.
Differentiating Cardiac vs. Respiratory Breathlessness
Both cardiac and respiratory diseases produce breathlessness, and overlap is common - especially in elderly, smoking, or multi-morbid patients. A systematic approach using history, physical examination, and targeted investigations resolves most cases.
1. Underlying Mechanisms
Cardiac dyspnea arises from increased pulmonary venous and capillary pressure due to left ventricular failure, mitral stenosis, or other conditions causing pulmonary congestion. The engorged pulmonary bed + interstitial/alveolar edema stiffens the lungs, stimulating ventilation via "J" (juxtacapillary) receptors. This increases the work of breathing and generates the sensation of breathlessness. - Fishman's Pulmonary Diseases, p. 3720
Respiratory dyspnea arises from airflow obstruction (asthma, COPD), intrinsic lung disease (pneumonia, ILD, fibrosis), reduced lung compliance, ventilation-perfusion mismatch, or neuromuscular weakness of the respiratory muscles.
2. History: Key Differentiating Features
| Feature | Points Toward Cardiac | Points Toward Respiratory |
|---|---|---|
| Quality of sensation | "Hunger for air," urge to breathe, air hunger | "Tightness," "cannot take a deep breath," increased effort/work of breathing |
| Chest tightness | Pulmonary edema (also) | Bronchoconstriction (asthma, COPD) - more typical |
| Orthopnea | Classic - 2-3 pillow orthopnea, LV failure, MS | Can occur in COPD/asthma (diaphragm mechanics), but less typical |
| Paroxysmal nocturnal dyspnea (PND) | Strongly suggests LV failure - patient wakes 1-2 hours after lying down, sits up for relief | Can occur in COPD (secretion pooling, nocturnal bronchoconstriction) but less specific |
| Wheezing | "Cardiac asthma" - late sign of pulmonary edema | Hallmark of obstructive airway disease |
| Cough | Productive pink frothy sputum; nocturnal cough in LVF | Productive purulent sputum (infection), chronic dry cough (ILD, ACE inhibitors), wheeze + cough (asthma) |
| Triggers | Exertion, lying flat, sodium/fluid load | Allergens, smoke, dust, cold air, exercise (in asthma); infections (COPD exacerbation) |
| Relief | Sitting upright (orthopnea), diuretics, nitrates | Bronchodilators (beta-agonists), sitting forward (tripod position in severe COPD) |
| Pace of onset | Acute decompensation - hours; chronic - gradual over weeks | Acute exacerbation - hours; chronic obstructive disease - insidious over years |
| Associated symptoms | Pedal edema, weight gain, palpitations, angina, fatigue | Wheeze, purulent sputum, fever (infection), haemoptysis |
| Smoking history | Less specific | Strong - COPD, lung cancer, ILD |
| Occupational exposure | Less specific | Pneumoconiosis, occupational asthma |
Important: Wheezing, dyspnea on exertion, orthopnea, PND, and leg edema alone are not sufficient to discriminate cardiac from pulmonary causes - they can occur in both. No single feature is definitive. - Tintinalli's Emergency Medicine, p. 3531
3. Physical Examination
| Sign | Cardiac | Respiratory |
|---|---|---|
| Auscultation - lungs | Bilateral basal fine (wet) crackles; wheeze in pulmonary edema | Wheeze (diffuse, expiratory > inspiratory in COPD/asthma); coarse crackles (infection); diminished breath sounds (COPD hyperinflation, effusion) |
| Heart sounds | S3 gallop - strongly suggests heart failure; loud P2 (pulmonary HTN); murmurs (valvular disease) | Usually normal heart sounds |
| Jugular venous distention (JVD) | Present in right or biventricular failure | Absent (unless cor pulmonale from chronic lung disease) |
| Peripheral edema | Bilateral pitting pedal edema (RV failure or biventricular) | Absent unless cor pulmonale |
| Chest shape | Normal or enlarged cardiac dullness | Barrel chest, hyperresonance to percussion (COPD); tracheal deviation (pneumothorax) |
| Accessory muscle use | Less prominent | Prominent - sternocleidomastoid, scalenes; tripod positioning |
| Pursed lip breathing | Absent | Characteristic of COPD |
| Cyanosis | Peripheral cyanosis (low output) | Central cyanosis (hypoxemia) |
An S3 gallop on physical exam or pulmonary venous congestion/interstitial edema with cardiomegaly on CXR strongly suggests heart failure. The overall clinical gestalt + JVD + alveolar edema together also suggest cardiac cause. - Tintinalli's Emergency Medicine, p. 3531
4. Investigations
Chest X-Ray (CXR)
| Finding | Cardiac | Respiratory |
|---|---|---|
| Cardiomegaly | Yes | No |
| Pulmonary venous congestion (upper lobe diversion) | Yes | No |
| Kerley B lines, bat-wing perihilar edema | Yes (pulmonary edema) | No |
| Bilateral pleural effusions | Yes (heart failure) | Usually unilateral or absent |
| Hyperinflation, flat diaphragms | No | Yes (COPD/emphysema) |
| Focal consolidation | No | Pneumonia |
| Interstitial pattern | (pulmonary edema can mimic) | ILD, fibrosis |
ECG
| Finding | Cardiac | Respiratory |
|---|---|---|
| LV hypertrophy / ST-T changes | Yes | No |
| Atrial fibrillation | Yes (common in HF, MS) | Possible in COPD exacerbation |
| Right heart strain (P pulmonale, right axis deviation, RBBB, S1Q3T3) | Pulmonary embolism / cor pulmonale | COPD / pulmonary hypertension |
Biomarkers
BNP / NT-proBNP is the most important biomarker for differentiating cardiac from non-cardiac dyspnea:
- BNP < 100 pg/mL (or NT-proBNP < 300 pg/mL): effectively excludes heart failure as the cause - 95-99% sensitivity. - Tintinalli's Emergency Medicine, p. 3553
- BNP > 500 pg/mL (or NT-proBNP > 900 pg/mL): moderately supports heart failure diagnosis
- BNP 100-500 pg/mL: indeterminate - not useful to include or exclude HF
- BNP sensitivity ~95-99%, specificity ~50-60% for heart failure - Goldman-Cecil Medicine, p. 2524
- Note: BNP is also elevated in pulmonary embolism, COPD exacerbation, sepsis, and renal failure - so a raised level alone is not diagnostic of cardiac cause
D-dimer: if normal, excludes pulmonary embolism in low-to-moderate pretest probability patients.
Troponin: elevated in ACS-related dyspnea, and also elevated (due to myocyte stress) in acute heart failure.
ABG (Arterial Blood Gas):
| Pattern | Suggests |
|---|---|
| Hypoxia + hypocapnia (type 1 RF) | Pulmonary cause (pneumonia, PE, pulmonary edema early) |
| Hypoxia + hypercapnia (type 2 RF) | Severe obstructive/restrictive respiratory disease (COPD, neuromuscular) |
| Normal PaO2, low PaCO2 | Hyperventilation / anxiety / metabolic acidosis |
| Metabolic acidosis + hyperventilation | Non-cardiac, non-respiratory (DKA, sepsis) |
Spirometry / Peak Flow
- FEV1/FVC < 70%: obstructive pattern - COPD or asthma
- FVC < 80% predicted with normal FEV1/FVC: restrictive pattern - ILD, pleural disease, NMD
- Normal spirometry in a breathless patient shifts suspicion toward cardiac or non-pulmonary cause
- Textbook of Family Medicine, p. 239
Echocardiography
The definitive test to confirm or exclude cardiac cause:
- Measures ejection fraction (systolic dysfunction in HFrEF)
- Identifies diastolic dysfunction (HFpEF)
- Detects valvular disease (MS, AR, MR)
- Identifies regional wall motion abnormalities (ischemia)
- Pericardial effusion / tamponade
Bedside/Point-of-Care Ultrasound (POCUS)
Extremely useful in emergency settings - can differentiate acute decompensated heart failure from non-cardiac causes of dyspnea rapidly:
- B-lines on lung US: bilateral multiple B-lines = pulmonary edema (cardiac)
- A-lines: normal or pneumothorax pattern (non-cardiac)
- Also identifies pleural effusion, cardiac function, IVC status. - Tintinalli's Emergency Medicine, p. 3551
5. Special Patterns Worth Knowing
| Pattern | Meaning |
|---|---|
| Orthopnea (lying flat worsens) | Classic for LV failure; also occurs in COPD (diaphragm mechanics) and bilateral diaphragmatic paralysis (instant orthopnea) |
| PND (wakes from sleep after 1-2 hrs, worse lying) | Strongly suggests LV failure; can occur in nocturnal asthma or COPD with secretions |
| Platypnea (worse when upright) | AV malformation at lung bases, hepatopulmonary syndrome |
| Trepopnea (worse on one side) | Asymmetric lung disease (V/Q mismatch) |
| Cardiac asthma | Wheeze from pulmonary edema - can mimic true asthma |
| Dyspnea + squatting (children) | Tetralogy of Fallot - squatting increases SVR and reduces R-L shunting |
6. Cardiopulmonary Exercise Testing (CPET)
When the cause of dyspnea remains unclear after the above, CPET is the gold standard for differentiating cardiac from pulmonary limitation:
- Cardiac limitation: VO2 max reduced, anaerobic threshold reached early, flat O2 pulse (stroke volume proxy), heart rate reserve exhausted
- Respiratory limitation: reduced breathing reserve, O2 desaturation on exercise, abnormal ventilatory equivalents
- Miller's Anesthesia, p. 1459; Fishman's Pulmonary Diseases
7. Quick Summary Algorithm
Breathless patient
|
Clinical assessment: History + Exam
|
+---> Fever + purulent sputum + focal signs → Respiratory infection (pneumonia)
+---> Wheeze + smoking + obstructive spirometry → COPD/Asthma
+---> S3 + JVD + basal crackles + bilateral edema → Heart Failure
+---> Pleuritic pain + risk factors → PE (D-dimer / CTPA)
|
v
CXR + ECG + SpO2
|
v
BNP / NT-proBNP
< 100 → HF unlikely → Pursue respiratory cause
> 500 → HF likely → Echo
|
v
Echo: confirms LV/valvular dysfunction
|
Still unclear → ABG + Spirometry + CPET
Sources: Goldman-Cecil Medicine (p. 2514-2520); Tintinalli's Emergency Medicine (p. 3529-3553); Fishman's Pulmonary Diseases (p. 3714-3740); Textbook of Family Medicine (p. 234-239); Frameworks for Internal Medicine (p. 3449-3468)
Treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
heart failure treatment dyspnea management guidelines
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Excellent - I have rich content from multiple authoritative sources. Let me now compile the comprehensive treatment answer.
Treatment of Breathlessness: Cardiac vs. Respiratory
The principle is simple: treat the underlying cause. General supportive measures apply to both; specific therapies differ sharply.
PART 1 - GENERAL (Initial) Approach to Any Breathless Patient
Regardless of cause, the first priority is:
- Sit the patient upright (reduces venous return, eases diaphragm work)
- Supplemental oxygen - target SpO2 ≥ 94% (but avoid high-flow O2 in known COPD - risk of hypercapnic drive suppression; target 88-92% in COPD)
- IV access + monitoring (SpO2, ECG, BP)
- Rapid assessment - ABG, CXR, ECG, BNP - to direct specific treatment
PART 2 - CARDIAC BREATHLESSNESS
A. Acute Heart Failure (AHF) - Immediate Management
AHF management is guided by the hemodynamic profile - first classify the patient:
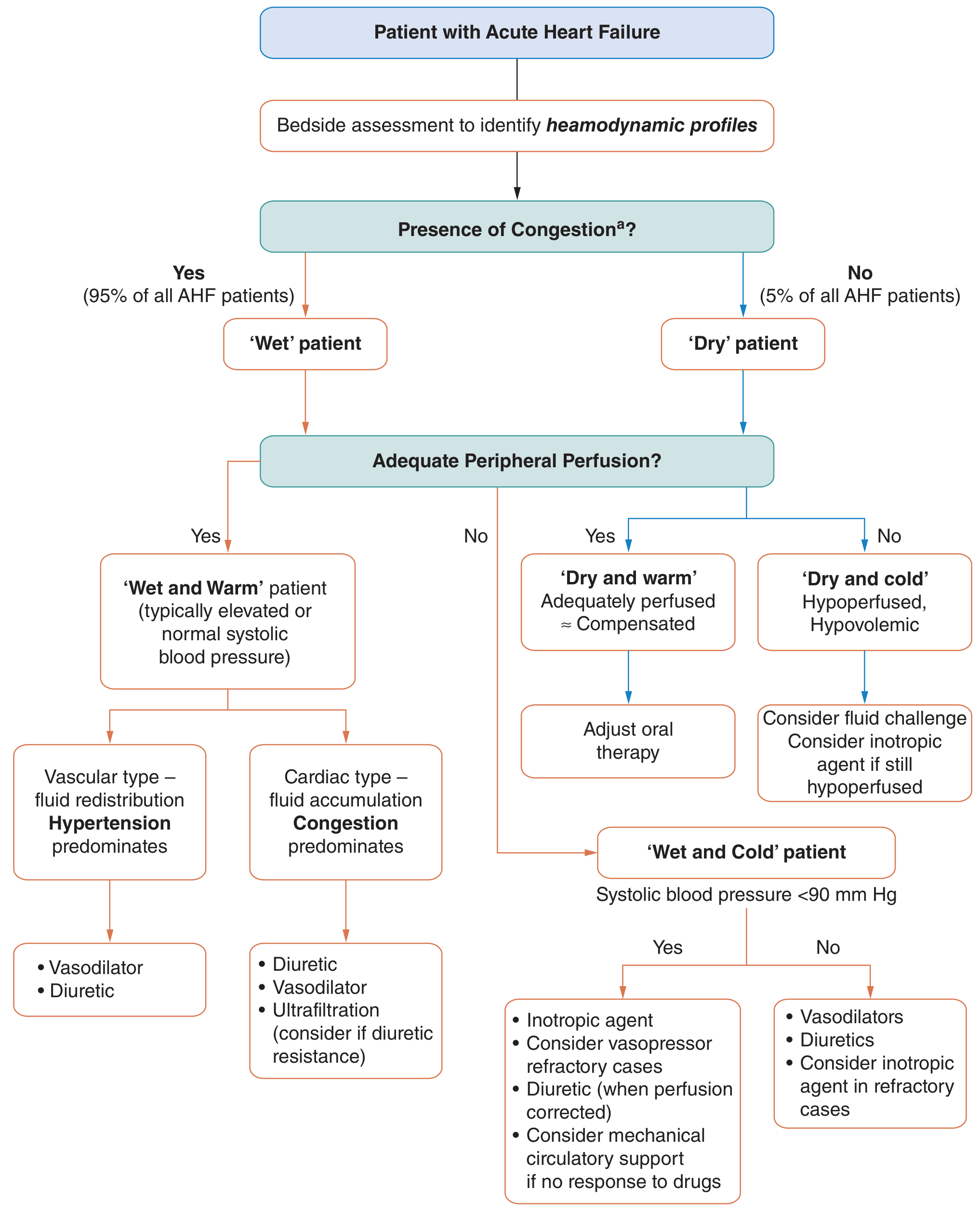
Figure: Management of acute heart failure based on clinical profile - Fuster & Hurst's The Heart, 15th Ed.
The two key questions are:
- Wet or Dry? (Is there congestion? - 95% of AHF patients are "wet")
- Warm or Cold? (Is peripheral perfusion adequate?)
| Profile | Clinical Picture | Primary Treatment |
|---|---|---|
| Wet + Warm (most common) | Congested, well-perfused, normal/elevated BP | Diuretics + Vasodilators |
| Wet + Cold (cardiogenic shock) | Congested, hypoperfused, SBP < 90 | Inotropes ± vasopressors + diuretics after perfusion restored; consider MCS |
| Dry + Warm | Compensated, euvolemic | Adjust oral GDMT |
| Dry + Cold | Hypovolemic, hypoperfused | Fluid challenge; inotropes if still hypoperfused |
1. Diuretics (Cornerstone of AHF Treatment)
Loop diuretics are the primary agents to relieve congestion and pulmonary edema:
- Furosemide IV - most widely used; IV dose should equal or exceed the patient's home oral dose
- Bumetanide, Torsemide - alternatives
- High-dose strategy (2.5x daily oral dose) shows trend toward better dyspnea relief and lower BNP vs. low-dose, with no significant difference in renal function (DOSE trial)
- For diuretic resistance: switch loop diuretic, add thiazide (metolazone), or consider ultrafiltration
- New evidence: Acetazolamide added to high-dose furosemide has shown important additive diuretic benefit
SGLT2 inhibitors (dapagliflozin, empagliflozin) also act as diuretics via glucosuresis and reduce cardiac preload and afterload, and are now part of the evidence base for both acute and chronic HF. - Katzung's Basic & Clinical Pharmacology, p. 884
2. Vasodilators
Reduce preload and afterload, relieve pulmonary congestion:
- Nitroglycerin (GTN) IV - first-line vasodilator; reduces preload and afterload; particularly useful when hypertension is present ("wet + warm - vascular type")
- Nitroprusside IV - more potent; reduces afterload significantly; useful in severe hypertension-driven flash pulmonary edema; requires close monitoring (risk of cyanide toxicity)
- Nesiritide - recombinant BNP; vasodilatory and mild diuretic effect
Recent meta-analysis (PMID 40506079, 2025): High-dose IV nitroglycerin shows superior efficacy vs. low-dose in sympathetic crashing acute pulmonary oedema.
3. Oxygen and Ventilatory Support
- High-flow oxygen for hypoxemia
- Non-Invasive Ventilation (NIV) - CPAP or BiPAP: first-line for respiratory failure in pulmonary edema; reduces work of breathing, improves oxygenation, reduces need for intubation
- Endotracheal intubation / mechanical ventilation: for severe respiratory failure, altered consciousness, inability to maintain airway
4. Inotropes (for "Cold" profile - reduced cardiac output)
For patients with hypoperfusion (cardiogenic shock):
- Dobutamine - beta-1 agonist; increases cardiac contractility and heart rate; first-line inotrope
- Dopamine - low dose (renal dose): dopaminergic effect; medium dose: beta-1 inotropic; high dose: vasopressor (alpha effect)
- Levosimendan - calcium sensitizer + K-ATP channel opener; positive inotropy without increasing O2 demand; approved in Europe; non-inferior to dobutamine; may have additional anti-stunning effect
- Milrinone - PDE3 inhibitor; inotrope + vasodilator (inodilator)
5. Vasopressors (for Cardiogenic Shock with Hypotension)
- Noradrenaline (Norepinephrine) - preferred vasopressor in cardiogenic shock
- Vasopressin - second line
6. Mechanical Circulatory Support (MCS)
For refractory cardiogenic shock unresponsive to drugs:
- Intra-aortic balloon pump (IABP) - reduces afterload, augments diastolic coronary perfusion
- Impella - percutaneous LV assist device
- ECMO (Extracorporeal membrane oxygenation) - for severe cardiorespiratory failure
- Fuster & Hurst's The Heart, p. 1869
7. Treat Precipitating Cause
Always identify and treat the trigger:
- ACS → emergency revascularization (PCI or thrombolysis)
- Atrial fibrillation with fast ventricular rate → rate control (beta-blocker, digoxin) or cardioversion
- Hypertensive emergency → rapid BP reduction with IV nitrates/nitroprusside
- Infection → antibiotics
- Non-compliance → resume medications, reinforce adherence
B. Chronic Heart Failure - Guideline-Directed Medical Therapy (GDMT)
The "Fantastic Four" of chronic HFrEF (EF ≤ 40%) - all reduce mortality:
| Drug Class | Examples | Mechanism / Benefit |
|---|---|---|
| ACE inhibitor / ARB | Enalapril, Ramipril / Losartan | Block RAAS; reduce remodeling, preload, afterload |
| Sacubitril/Valsartan (ARNI) | Entresto | Superior to ACE inhibitor alone (PARADIGM-HF); reduces HF hospitalization and mortality |
| Beta-blocker | Carvedilol, Bisoprolol, Metoprolol succinate | Block sympathetic activation; reduce HR, reverse remodeling |
| MRA (Mineralocorticoid receptor antagonist) | Spironolactone, Eplerenone | Block aldosterone; reduce fibrosis and edema |
| SGLT2 inhibitor | Dapagliflozin, Empagliflozin | Diuretic + cardioprotective; reduce HF hospitalizations in HFrEF and HFpEF |
Loop diuretic (furosemide) for symptom relief (edema, dyspnea) - does not reduce mortality but relieves congestion.
Ivabradine - reduces heart rate in sinus rhythm when HR remains ≥ 70 bpm despite beta-blocker.
Device therapy:
- ICD (Implantable cardioverter defibrillator) - for EF ≤ 35%, to prevent sudden cardiac death
- CRT (Cardiac resynchronization therapy) - for LBBB + EF ≤ 35%; improves cardiac output and symptoms
PART 3 - RESPIRATORY BREATHLESSNESS
A. Acute Exacerbation of COPD (AECOPD)
| Treatment | Details |
|---|---|
| Controlled O2 therapy | Target SpO2 88-92%; avoid hyperoxia (suppresses hypoxic drive, worsens hypercapnia) |
| Short-acting bronchodilators | Salbutamol (albuterol) nebulized + Ipratropium (anticholinergic) nebulized - first-line; every 4-6 hours |
| Systemic corticosteroids | Prednisolone 30-40 mg orally for 5 days; reduces inflammation, shortens recovery |
| Antibiotics | If purulent sputum or signs of infection - amoxicillin, doxycycline, or clarithromycin; 5-7 days |
| NIV (BiPAP) | For type 2 respiratory failure (hypercapnia + respiratory acidosis, pH < 7.35); reduces intubation rate and mortality |
| Intubation / invasive ventilation | If NIV fails or contraindicated; if obtunded |
| Theophylline | Second-line bronchodilator; narrow therapeutic window; rarely used now |
| Diuretics | Only if cor pulmonale / RV failure with edema |
B. Acute Asthma Attack
| Severity | Treatment |
|---|---|
| Mild-Moderate | Salbutamol (albuterol) pMDI via spacer (4-8 puffs) or nebulized; ipratropium add-on; oral prednisolone 40-50 mg |
| Severe | Nebulized salbutamol + ipratropium continuously; IV/oral steroids; magnesium sulphate IV 1.2-2 g over 20 min (bronchodilation + anti-inflammatory) |
| Life-threatening (near fatal) | ICU; IV salbutamol infusion; heliox; consider intubation (dangerous - risk of air trapping); anaesthetic agents (ketamine, halothane) as bronchodilators |
| Oxygen | High-flow O2 to maintain SpO2 ≥ 94% (unlike COPD) |
C. Pneumonia
- Antibiotics - guided by severity (CURB-65 score):
- Community-acquired: amoxicillin ± clarithromycin (covers atypicals)
- Severe/hospital: piperacillin-tazobactam + macrolide; consider co-amoxiclav in milder cases
- Supportive: O2, fluids, antipyretics
- Ventilatory support if severe hypoxia (high-flow nasal cannula, CPAP, intubation)
D. Pulmonary Embolism
- Anticoagulation - immediate: LMWH/UFH or DOAC (rivaroxaban, apixaban); long-term: DOAC x 3-6 months minimum
- Thrombolysis - for massive PE with haemodynamic instability (alteplase 100 mg IV)
- Embolectomy - surgical or catheter-directed for failed thrombolysis
E. Pneumothorax
- Small/spontaneous (primary): observation or simple aspiration
- Large/tension: immediate needle decompression (2nd intercostal space, mid-clavicular line), then chest drain
F. Interstitial Lung Disease (ILD / Fibrosis)
- Anti-fibrotics: Pirfenidone or Nintedanib for IPF - slow progression
- Systemic corticosteroids for inflammatory ILDs (hypersensitivity pneumonitis, NSIP)
- Lung transplant for advanced disease
- Pulmonary rehabilitation - improves exercise tolerance and dyspnea
PART 4 - Palliative / Symptomatic Treatment of Refractory Breathlessness
When the underlying cause cannot be fully reversed (advanced cancer, terminal COPD, end-stage HF):
- Opioids (morphine): most evidence-based treatment for refractory dyspnea; titrate carefully - no evidence of respiratory depression at correct doses; oral or SC morphine is effective
- Benzodiazepines (lorazepam, midazolam): for anxiety-related breathlessness; adjunct to opioids
- Cool moving air (fan, open window): stimulates trigeminal receptors; reduces perception of breathlessness
- Oxygen: only if hypoxic; not better than air for non-hypoxic dyspnea
- Corticosteroids: for lymphangitis carcinomatosa, superior vena cava obstruction, or malignant airway obstruction
- Textbook of Family Medicine, p. 3775
Summary Table
| Cause | Acute Treatment | Chronic Treatment |
|---|---|---|
| Acute HF / Pulmonary edema | IV furosemide, GTN, NIV, O2 | ACEi/ARB/ARNI, beta-blocker, MRA, SGLT2i, diuretic |
| Cardiogenic shock | Inotropes, vasopressors, MCS | Optimize GDMT, CRT, ICD, transplant |
| ACS-related dyspnea | O2, nitrates, PCI/thrombolysis | Dual antiplatelet, statin, ACEi, beta-blocker |
| AECOPD | SABDs nebulized, steroids, antibiotics, NIV | LABA+LAMA, ICS, pulmonary rehab |
| Acute asthma | Salbutamol, steroids, Mg sulphate | ICS + LABA, leukotriene antagonists |
| Pneumonia | Antibiotics, O2, supportive | Pneumococcal/flu vaccination |
| PE | Anticoagulation, thrombolysis | DOAC 3-6 months |
| Tension pneumothorax | Needle decompression, chest drain | - |
| Refractory/terminal | Opioids, benzodiazepines, fan | Palliative care MDT |
Sources: Fuster & Hurst's The Heart, 15th Ed. (pp. 1869-1927); Katzung's Basic & Clinical Pharmacology, 16th Ed. (pp. 880-887); Goldman-Cecil Medicine (pp. 2518-2540); Tintinalli's Emergency Medicine (pp. 3558-3560); Textbook of Family Medicine (p. 3775)
This is a shared conversation. Sign in to Orris to start your own chat.