Metastasis and routes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compose the full response.
Metastasis and Routes of Spread
Metastasis is the spread of a tumor to sites physically discontinuous with the primary tumor. It is what unequivocally marks a tumor as malignant, and it is one of the principal causes of cancer mortality. About 30% of solid tumors (excluding non-melanoma skin cancers) already present with clinically evident metastases at diagnosis, and an additional 20% have occult spread at that time.
Key point: invasiveness and metastasis are separable properties. Basal cell carcinoma and most CNS gliomas invade locally but rarely metastasize. Conversely, some small well-differentiated tumors metastasize widely.
Routes of Spread
Malignant neoplasms disseminate by three main pathways:
1. Seeding of Body Cavities and Surfaces
Occurs when a tumor invades a natural "open field" lacking physical barriers.
- Most common site: the peritoneal cavity
- Other cavities involved: pleura, pericardium, meninges, joint spaces
- Classic example: Ovarian carcinoma - spreads widely over peritoneal surfaces without necessarily invading the underlying tissue
- Mucus-secreting appendiceal or ovarian carcinomas can fill the peritoneal cavity with gelatinous tumor mass - pseudomyxoma peritonei
- CNS tumors (medulloblastoma, ependymoma) may penetrate cerebral ventricles and seed meningeal surfaces via CSF
2. Lymphatic Spread
The most common initial route for carcinomas. Sarcomas may also use this route.
- Tumors themselves lack functional lymphatics, but vessels at the tumor's margin are sufficient for spread
- Spread follows natural routes of lymphatic drainage
Examples by primary site:
| Primary Tumor | First Nodal Station |
|---|---|
| Breast (upper outer quadrant) | Axillary nodes → infraclavicular/supraclavicular |
| Breast (medial) | Internal mammary chain nodes |
| Lung (major airways) | Perihilar tracheobronchial → mediastinal nodes |
| Colorectal | Mesenteric nodes |
| Testis | Para-aortic nodes |
Skip metastasis: tumor cells can bypass immediately adjacent nodes and appear in distal nodes - possibly because microscopic disease is missed in proximal nodes or because of anatomical variation in lymphatic channels.
Sentinel lymph node (SLN): The first regional lymph node receiving lymph from the primary tumor. Identified by injecting dyes or radiolabeled tracers near the tumor. SLN biopsy is used clinically to determine extent of spread (e.g., in breast cancer, melanoma) and guide treatment. Important: enlarged nodes near a tumor do not always signal metastasis - reactive hyperplasia (lymphadenitis) from tumor antigens can enlarge nodes too; biopsy is necessary.
3. Hematogenous Spread
Favored by sarcomas, but carcinomas also use this route - especially late in disease. Venous invasion is far more common than arterial because veins have thinner walls.
Why veins and not arteries? Thin-walled veins are more easily penetrated. Once in the bloodstream, tumor cells arrest in the first capillary bed they encounter.
Vascular anatomy determines the most common metastatic sites:
| Venous Drainage | Organs Affected |
|---|---|
| Portal venous system (GI tract, pancreas) | Liver - most common site of hematogenous mets |
| Systemic veins (caval system) | Lungs |
| Paravertebral venous plexus (thyroid, prostate) | Vertebral column/spine |
Special patterns of hematogenous spread (organ tropism):
- Prostate → bone (osteoblastic)
- Bronchogenic carcinoma → adrenal glands, brain
- Breast → bone, lung, liver, brain
- Neuroblastoma → liver, bones
- Uveal melanoma → liver
- Renal cell carcinoma / Hepatocellular carcinoma → can grow as a snakelike cord inside the IVC or renal vein (intravenous growth without widespread dissemination)
- Skeletal muscle, despite being richly vascularized, is rarely a site of metastasis
The Metastatic Cascade (Molecular Steps)
The entire metastatic process can be subdivided into two phases:
- Invasion of the ECM
- Vascular dissemination, homing, and colonization
The metastatic cascade (hematogenous spread):
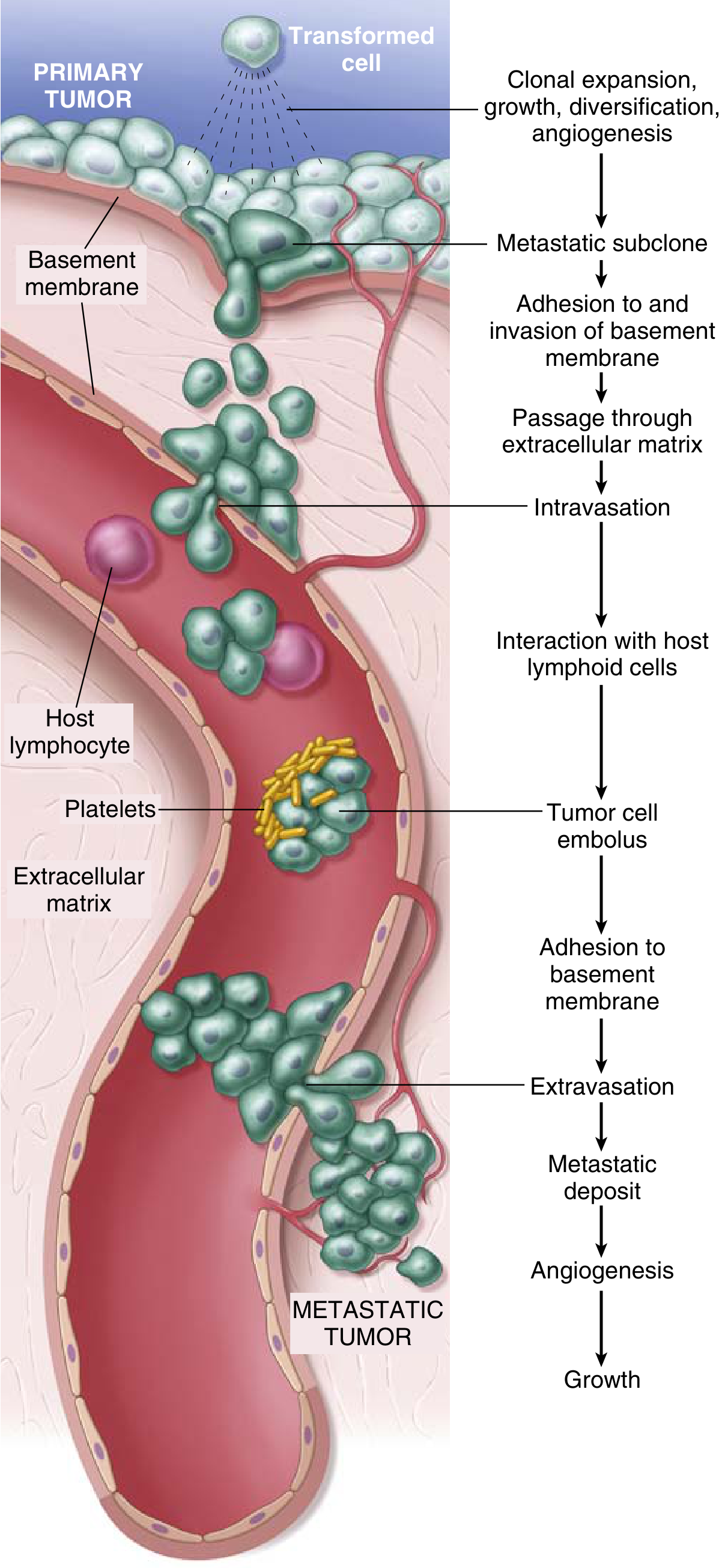
Phase 1: Invasion of ECM
Step 1 - Loosening of intercellular connections:
- E-cadherin acts as intercellular "glue." Its cytoplasmic portion binds β-catenin; E-cadherin also transmits antigrowth signals
- In many epithelial cancers, E-cadherin function is lost via: mutational inactivation, β-catenin activation, or upregulation of SNAIL and TWIST transcription factors (which suppress E-cadherin expression)
- This is part of Epithelial-Mesenchymal Transition (EMT)
Step 2 - Local ECM degradation:
- Tumor cells secrete or induce stromal cells (fibroblasts, macrophages) to produce proteolytic enzymes
- Key enzymes: matrix metalloproteinases (MMPs) - degrade collagen, glycoproteins, and proteoglycans
- MMP activity: cleaves ECM, releases growth factors stored within it, generates fragments with pro-migratory or pro-angiogenic activity
Step 3 - Migration of tumor cells:
- Tumor cells move through degraded ECM
- Migration is guided by: chemokines, fragments of degraded ECM (laminin), and growth factors from stromal cells and ECM stores
Phase 2: Vascular Dissemination and Colonization
| Step | Description |
|---|---|
| Intravasation | Tumor cells penetrate blood/lymph vessel walls |
| Survival in circulation | Most cells die - from shear stress, immune attack (NK cells, T cells); some survive by aggregating with platelets (platelet cloak protects them) |
| Arrest | Tumor cell emboli lodge in capillary beds |
| Extravasation | Cells adhere to vascular endothelium and exit vessels using mechanisms similar to those at invasion |
| Colonization | Formation of micrometastases → requires angiogenesis → growth into macroscopic tumor |
Note: metastasis is remarkably inefficient. Millions of cells may enter the bloodstream daily from a primary tumor, yet only a tiny fraction ever establish secondary growths. This reflects the many barriers at each step.
Gross Pathology: Liver with Metastatic Cancer

The image above shows a liver studded with multiple pale metastatic nodules - the classic appearance of hematogenous metastasis from a GI primary via the portal venous system.
Summary Table
| Route | Typical Tumor Type | Classic Example |
|---|---|---|
| Seeding of body cavities | Ovarian, GI carcinomas | Ovarian ca → peritoneal seeding; pseudomyxoma peritonei |
| Lymphatic | Carcinomas (most common initial route) | Breast → axillary nodes; Lung → hilar nodes |
| Hematogenous | Sarcomas (primarily); carcinomas (also) | GI → liver; lung/breast → lungs; prostate → bone |
| CSF/meningeal | CNS tumors | Medulloblastoma → spinal cord seeding |
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), p. 221-222; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 259-261
This is a shared conversation. Sign in to Orris to start your own chat.