Charnelys friction arthroplasty in orthopaedics 10 marks pg answer with flow chart and images
Charnley low friction arthroplasty principles components technique indications
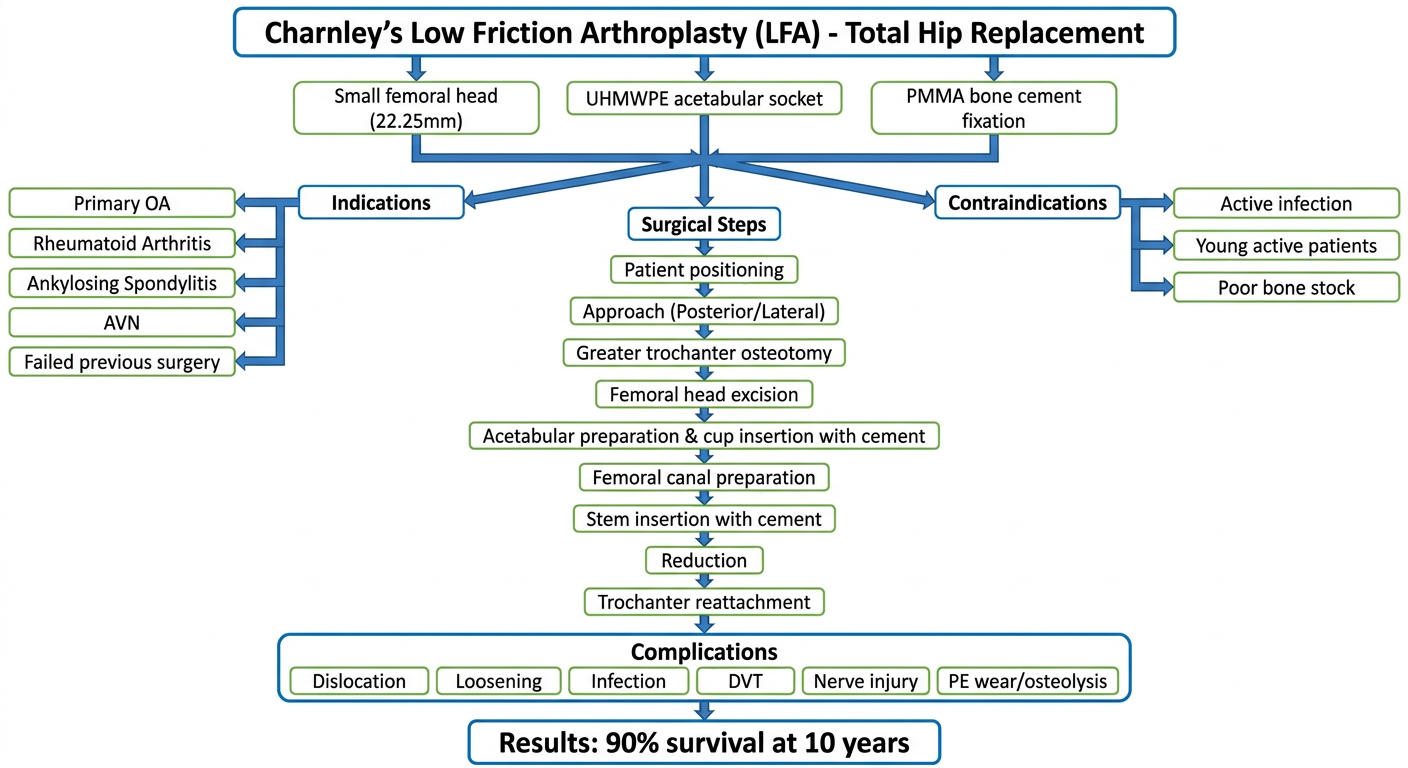
A detailed medical flowchart for Charnley's Low Friction Arthroplasty (LFA) of the hip. The flowchart should show: 1) Definition box at top: "Charnley's Low Friction Arthroplasty (LFA) - Total Hip Replacement". 2) Three main principle boxes: Small femoral head (22.25mm), UHMWPE acetabular socket, PMMA bone cement fixation. 3) Indications branch: Primary OA, Rheumatoid Arthritis, Ankylosing Spondylitis, AVN, Failed previous surgery. 4) Contraindications branch: Active infection, Young active patients, Poor bone stock. 5) Surgical steps flowchart: Patient positioning → Approach (Posterior/Lateral) → Greater trochanter osteotomy → Femoral head excision → Acetabular preparation & cup insertion with cement → Femoral canal preparation → Stem insertion with cement → Reduction → Trochanter reattachment. 6) Complications box: Dislocation, Loosening, Infection, DVT, Nerve injury, PE wear/osteolysis. 7) Results box at bottom: 90% survival at 10 years. Clean white background, medical blue and green color scheme, clear arrows connecting each step.
Charnley's Low Friction Arthroplasty (LFA) of the Hip
Introduction
Principle of Low Friction
| Component | Charnley's Choice | Rationale |
|---|---|---|
| Femoral head | Small (22.225 mm diameter) | Reduces lever arm, minimizes torque |
| Acetabular socket | Ultra-High Molecular Weight Polyethylene (UHMWPE) | Very low friction coefficient (~0.02) vs. cartilage (0.002) |
| Fixation | PMMA bone cement (acrylic) | Secure interface load transfer |
Components
- Forged stainless steel (later cobalt-chrome alloys)
- Small polished spherical head: 22.225 mm (originally tried 41 mm then reduced)
- Straight stem cemented into femoral canal with PMMA
- Later designs: smooth polished slip-taper stems (designed to slightly subside in cement, compressing it into bone)
- All-polyethylene cup (UHMWPE)
- Cemented into reamed acetabulum
- Flanged designs improve cement pressurization
- Cup positioned at 45° abduction (Lewinnek safe zone: 40-50° abduction, 5-25° anteversion)
- Polymethylmethacrylate
- Acts as a grout - fills trabecular spaces for microinterlock
- Does NOT chemically bond to bone or metal - purely mechanical
- Strongest in compression, weakest in tension (hence cemented cups fail more than stems)

Indications
-
Primary indications:
- Osteoarthritis (most common) - Kellgren-Lawrence Grade 3 and 4
- Rheumatoid arthritis
- Ankylosing spondylitis
- Avascular necrosis of femoral head
- Failed previous hip surgery / hemiarthroplasty
- Post-traumatic arthritis
- Neglected congenital dislocation of hip
- Protrusio acetabuli
-
General criteria:
- Debilitating pain affecting activities of daily living
- Pain not controlled by conservative measures
- Patient medically fit for surgery
- No active infection anywhere in body
Contraindications
- Active infection (local or systemic)
- Young, very active patients (cement fatigue risk)
- Neuropathic joint (Charcot arthropathy)
- Insufficient bone stock
- Neurological disorders with spasticity
- Patient unable to comply with postoperative restrictions
Surgical Technique
| Approach | Interval | Risk | Pros |
|---|---|---|---|
| Posterior (Southern) | Gluteus maximus split + external rotator tenotomies | Sciatic nerve | Extensible, quick |
| Lateral (Hardinge) | Gluteus medius split | Superior gluteal nerve/artery | Good stability |
| Anterolateral (Watson-Jones) | TFL and gluteus medius | SGA branch | Stable |
| Anterior (Smith-Petersen) | Sartorius/TFL + rectus/gluteus medius | LFCN, ascending LCFA | No dislocation |
- Greater trochanter detachment (osteotomy) for wide exposure
- Hip dislocation and femoral head excision at neck
- Acetabular reaming to hemispherical shape
- Cement pressurization into acetabular cancellous bone
- UHMWPE cup insertion at 40-45° abduction, 10-15° anteversion
- Femoral canal preparation (broaching)
- Cement gun insertion of PMMA into femoral canal
- Stem introduction - press-fit, then cement hardens
- 22.225 mm head reduction into cup
- Greater trochanter reattachment with wires/cables
- Wound closure in layers
Flowchart
Cemented Femoral Stem Design
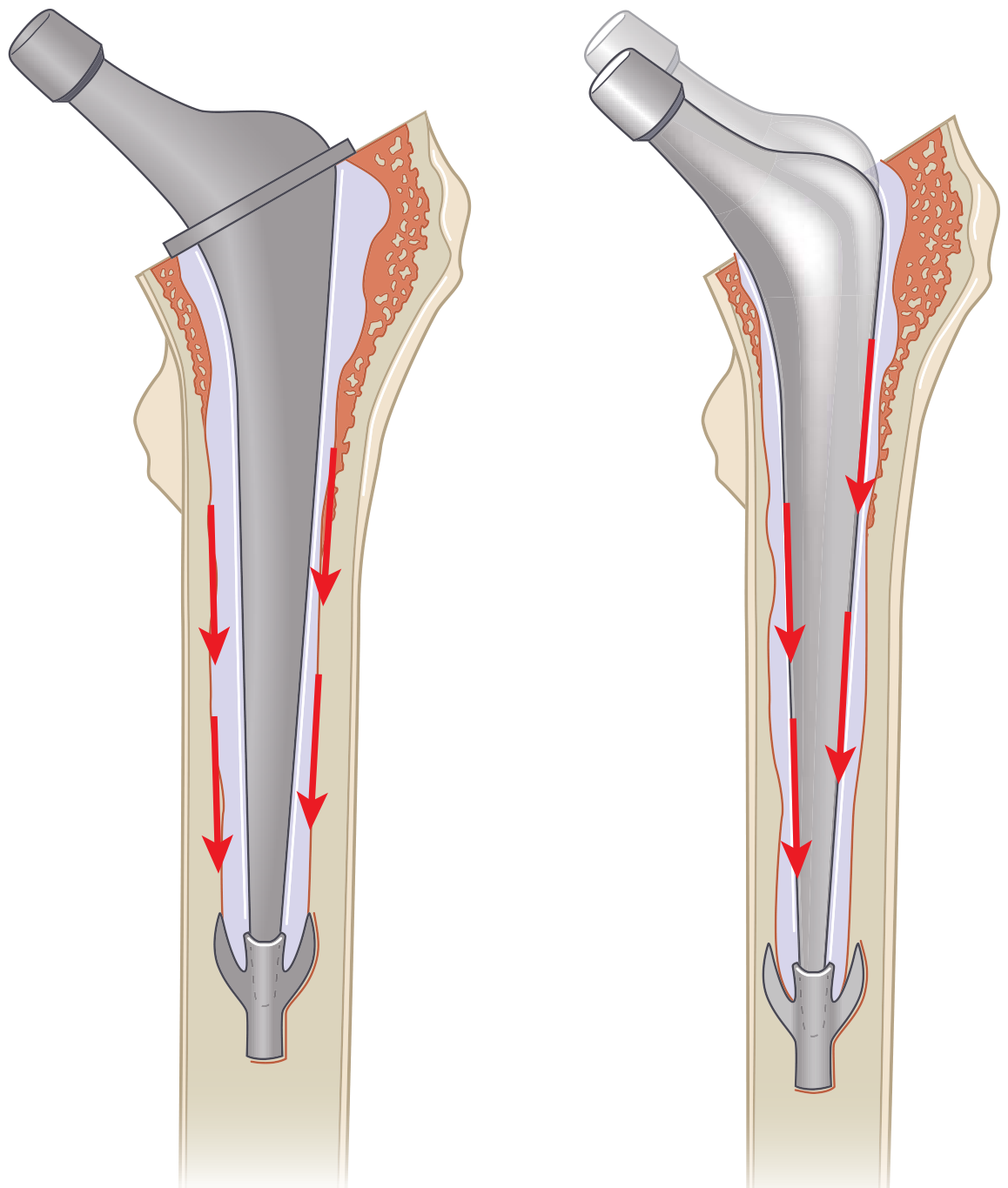
- Microinterlock with endosteal bone trabecular spaces
- Cement fatigues with cyclic loading starting at stress points
- A mantle defect (where prosthesis touches bone) = area of high stress concentration
- Cemented stems fail at a lower rate than cups because stems experience primarily compressive forces, while cups experience shear/tension
Biomechanical Basis - Joint Reaction Force Reduction
- Reduce the joint reaction force (JRF)
- Minimize wear and mechanical loosening
- Protect the bone-cement interface
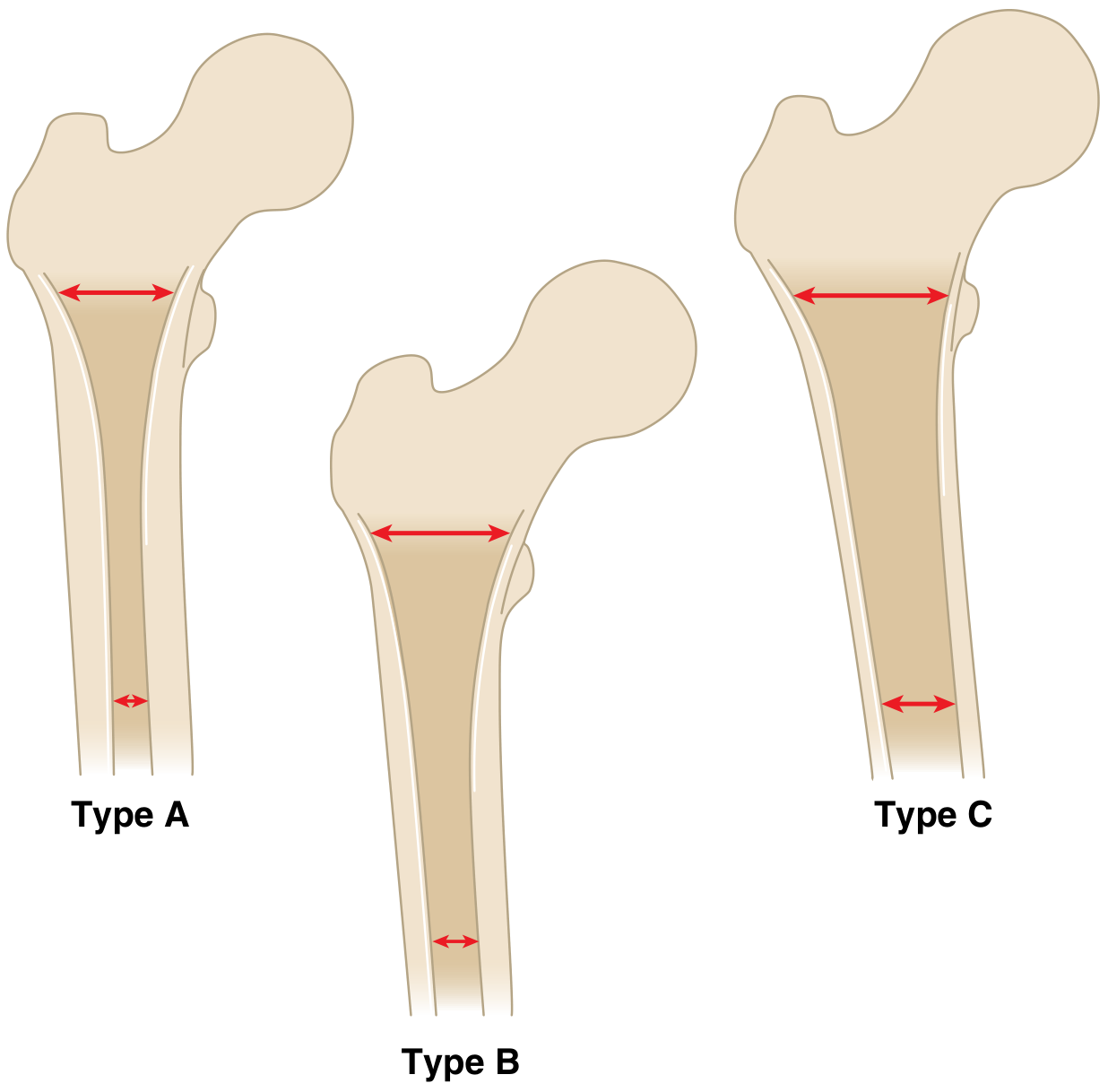
Dorr Classification (Guides Stem Selection)
Complications
- Dislocation (most common - especially posterior approach, ~2-3%)
- Wound infection / deep periprosthetic infection
- DVT / Pulmonary embolism
- Nerve injury (sciatic > femoral)
- Vascular injury
- Periprosthetic fracture
- Aseptic loosening - most common late complication
- Cement-bone interface failure
- Osteolysis from polyethylene wear particles
- PE wear and osteolysis: Submicron PE particles phagocytized by macrophages → RANKL-mediated osteoclast activation → bone resorption. Volumetric wear = π × r² × w
- Heterotopic ossification (Brooker classification)
- Trochanteric non-union (specific to original technique)
- Periprosthetic fracture (Vancouver classification)
- Leg length discrepancy
Results
- Charnley's original series: 90%+ survivorship at 10 years, 80%+ at 20 years
- Long-term results published by Wroblewski (Wrightington series): Charnley LFA 25-year survivorship approaching 75-80%
- The low-friction principle remains the foundation of all modern THA designs
- Modern improvements: highly cross-linked PE (HCLPE), cementless fixation, modular heads, ceramic bearings - all build on Charnley's framework
Summary Points for Exam
| Feature | Detail |
|---|---|
| Introduced | Sir John Charnley, 1960s, Wrightington |
| Femoral head size | 22.225 mm stainless steel |
| Socket material | UHMWPE (ultra-high MW polyethylene) |
| Fixation | PMMA bone cement |
| Friction coefficient | ~0.02 |
| Approach | Lateral with GT osteotomy (original) |
| Key principle | Low frictional torque = protect cement-bone interface |
| 10-year survival | ~90% |
Sources: Miller's Review of Orthopaedics 9th Edition, Section 5 THA, pp. 380-414; Campbell's Operative Orthopaedics 15th Ed 2026; Wroblewski (2009) - principle of low frictional torque