USE OF ULTRASOUND IN AIRWAY ASSESSMENT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"airway ultrasound" AND assessment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a thorough, well-illustrated answer. Let me compile it.
Use of Ultrasound in Airway Assessment
Ultrasound has evolved into a valuable point-of-care tool for pre-intubation assessment, procedural guidance, and post-intubation confirmation. Its real-time, non-ionizing, and bedside nature makes it particularly useful in emergency, critical care, and anesthetic settings. The applications can be organized into five major domains.
1. Sonographic Anatomy of the Airway
A high-frequency linear probe (7-15 MHz) is used for most anterior neck assessments. Key structures visible on ultrasound include:
- Tracheal rings - C-shaped hypoechoic cartilages with characteristic posterior acoustic shadowing due to air attenuation
- Thyroid gland - hyperechoic, flanking the trachea laterally
- Cricothyroid membrane (CTM) - the soft tissue gap between the thyroid and cricoid cartilages
- Esophagus - visualized posterior and slightly lateral to the trachea in transverse views
The transverse (axial) view gives a cross-section of the trachea and is the most useful for ETT confirmation, while the midline sagittal view is preferred for CTM identification.
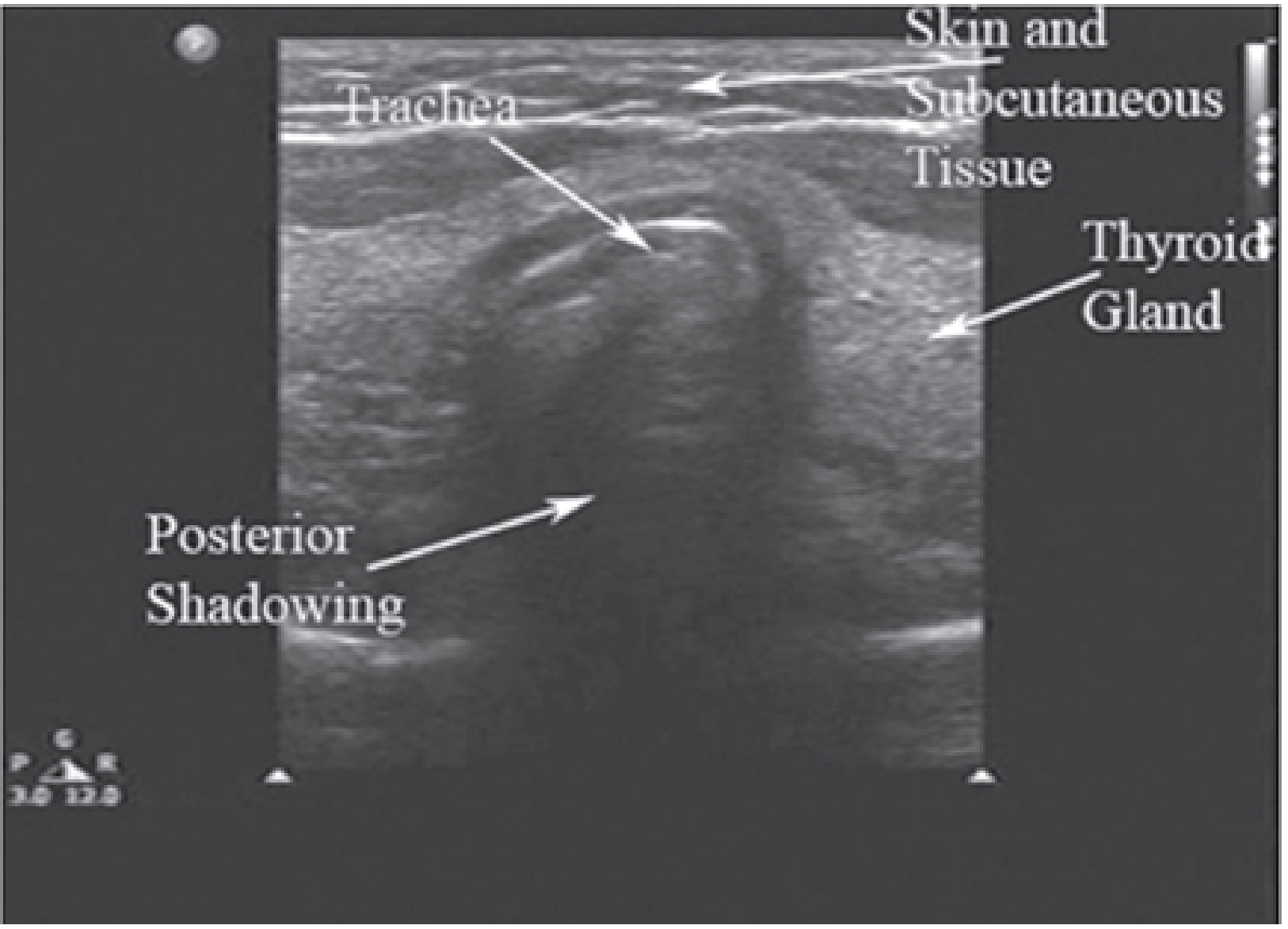
Fig. 1 - Transverse view of the trachea. The anechoic area posterior to the tracheal rings represents acoustic shadowing from dense cartilage. The thyroid gland is visible bilaterally. (Morgan & Mikhail's Clinical Anesthesiology, 7e)
2. Pre-Intubation Assessment / Difficult Airway Prediction
Ultrasound can supplement traditional bedside assessment (Mallampati, thyromental distance, mouth opening) for predicting difficult intubation:
| Parameter | Ultrasound Finding | Clinical Relevance |
|---|---|---|
| Pretracheal soft tissue thickness | Measured in sagittal/transverse plane at thyroid cartilage level | Increased in obese patients; predicts difficult mask ventilation and intubation |
| Tongue base thickness | Measured submentally | Larger tongue correlates with higher Mallampati score |
| Hyoid-to-skin distance | Distance from skin surface to hyoid bone | Increased distance associated with difficult laryngoscopy |
| Epiglottis visibility | May be seen in midline sagittal plane | Helps assess anatomy prior to intubation |
According to Barash's Clinical Anesthesia (9e): "Ultrasound can be used in trauma care to predict difficult airways, to identify the cricothyroid membrane, to facilitate rapid front-of-neck access in expected difficult airways, and to confirm endotracheal (vs. esophageal) tube position, especially in low cardiac output state where capnography can be less reliable."
Morbidly obese patients (BMI ≥30) deserve particular attention - ultrasound can quantify redundant pharyngeal tissue and neck circumference that may predict both difficult intubation and difficult bag-mask ventilation.
3. Cricothyroid Membrane (CTM) Identification
This is one of the highest-yield applications of airway ultrasound, especially in the "can't intubate, can't oxygenate" (CICO) scenario.
Why it matters
Traditional palpation-based CTM identification fails in up to 30-60% of obese or anatomically challenging patients. Ultrasound localizes the CTM accurately even in difficult necks.
Technique
- Place a linear probe midline sagittal on the anterior neck
- The thyroid cartilage appears as a hyperechoic structure superiorly
- Below it, the CTM appears as the echogenic soft tissue gap between thyroid and cricoid cartilages
- The air-mucosal interface appears as a bright hyperechoic line with posterior reverberation artifacts
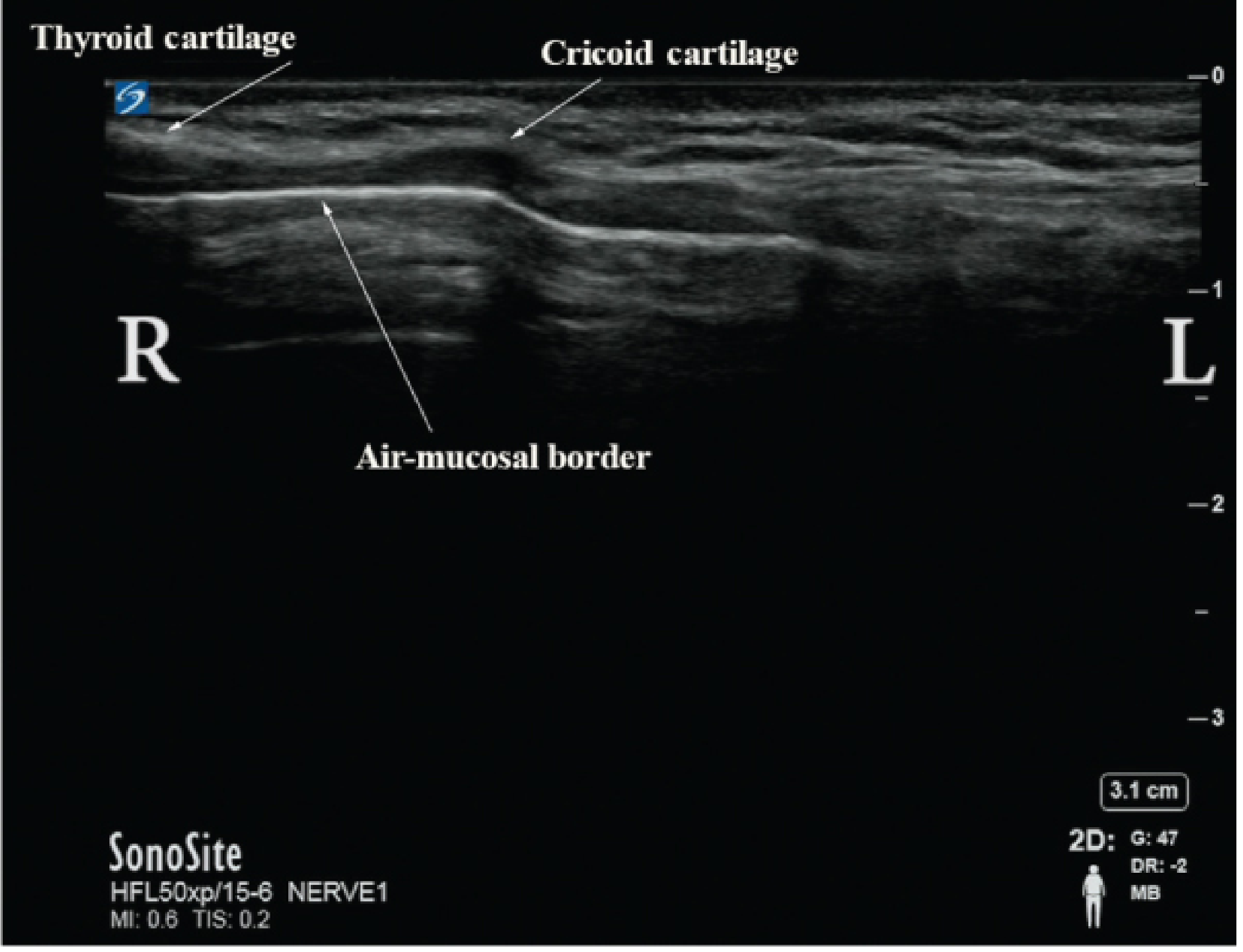
Fig. 2 - Midline sagittal ultrasound view of the CTM. Thyroid cartilage (left), cricoid cartilage (right), and the air-mucosal border are clearly labeled. This view guides emergency cricothyrotomy needle/scalpel placement. (Barash Clinical Anesthesia, 9e)
Clinical application
Roberts & Hedges' Clinical Procedures in Emergency Medicine describes the use of ultrasound to localize the CTM before simulated failed intubation, with studies showing ultrasound-guided marking significantly increases accuracy compared to digital palpation alone. The 4-step cricothyrotomy technique can be modified to use ultrasound pre-marking of the CTM to reduce laryngeal/tracheal injury.
POCUS improves success rates for:
- Emergency cricothyrotomy
- Percutaneous tracheostomy (identification of tracheal rings and avoidance of blood vessels)
4. Endotracheal Tube (ETT) Placement Confirmation
Confirming tracheal vs. esophageal intubation is a critical application, particularly when capnography is unreliable (low cardiac output states, cardiac arrest, CPR).
Tracheal intubation
The probe is placed transversely on the anterior neck at the level of the suprasternal notch or just above. During intubation:
- The ETT passing through the trachea appears as a hyperechoic structure with a "double-wall" sign within the tracheal air shadow
- Tube motion can be visualized in real time as the ETT passes beneath the probe
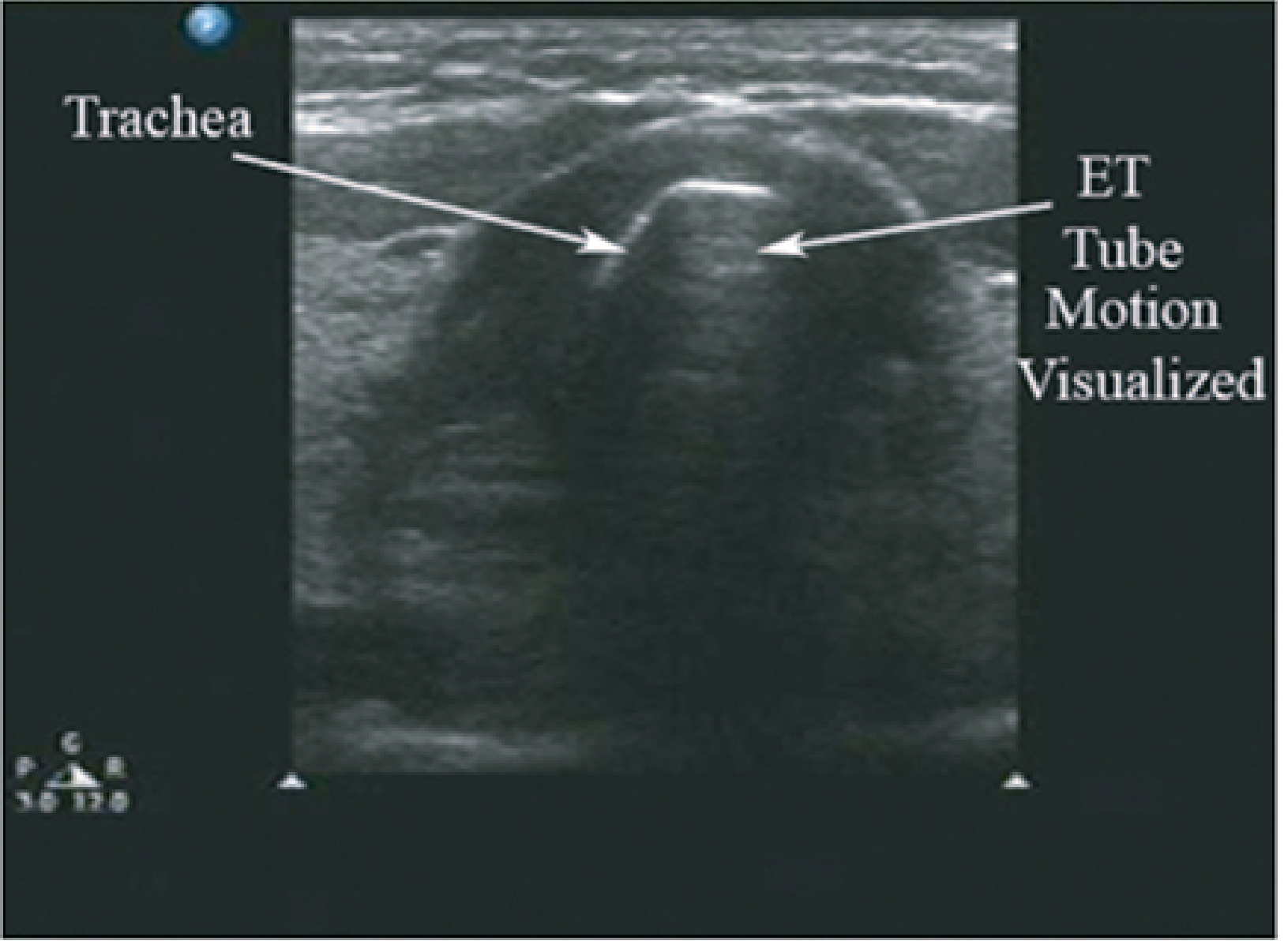
Fig. 3 - Transverse view during tracheal intubation. The arrow points to increased echogenicity and visible motion of the ETT passing just distal to the tracheal cartilage. (Morgan & Mikhail's, 7e)
Esophageal intubation
Immediately recognizable: a second tubular structure appears posterior and lateral to the trachea - the esophagus - with two parallel echogenic lines representing the inner and outer walls of the ETT passing through it.
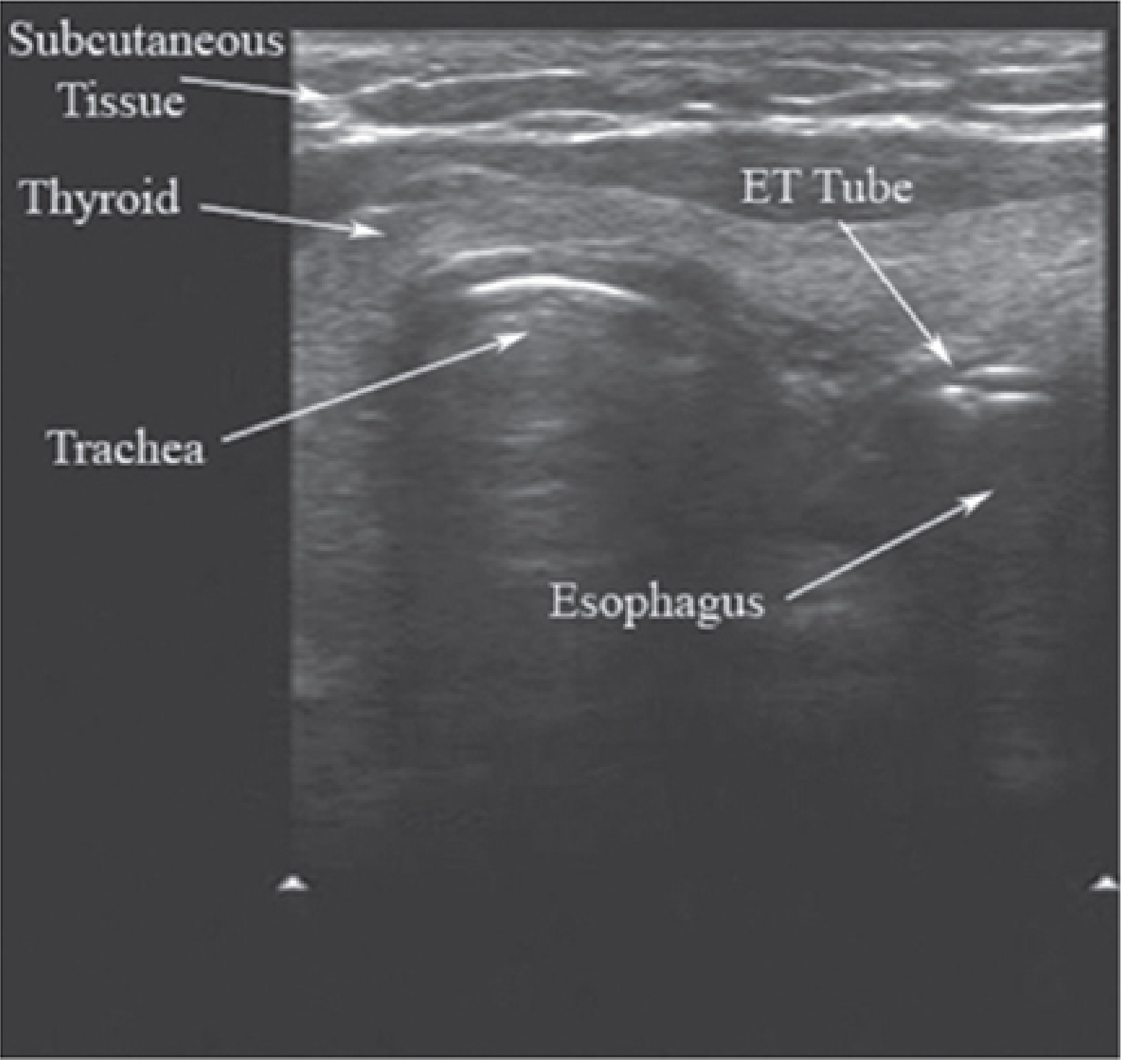
Fig. 4 - Transverse view during esophageal intubation. The trachea and esophagus are visible. The ET tube is seen posterior-lateral to the trachea within the esophagus lumen (two parallel echogenic lines). (Morgan & Mikhail's, 7e)
Intratracheal vs. esophageal confirmation (Tintinalli view)
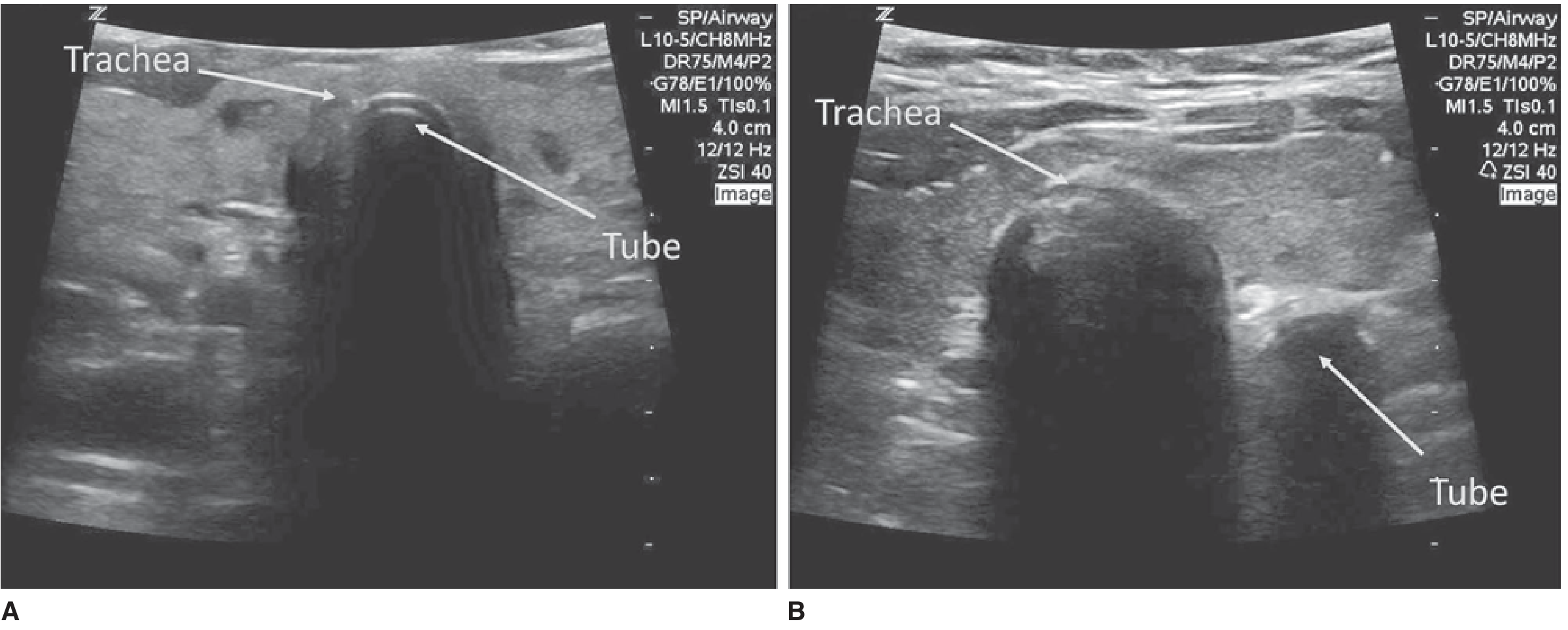
Fig. 5 - Intratracheal (A) vs. esophageal (B) ETT placement. In tracheal placement, the tube is seen within the single midline trachea. In esophageal placement, the tube creates a second circular structure lateral to the trachea. (Tintinalli's Emergency Medicine)
Additional ETT confirmation methods
- Lung sliding - bilateral lung sliding on pleural ultrasound after intubation confirms bilateral ventilation and excludes right mainstem bronchus placement
- Diaphragmatic movement - bilateral symmetric diaphragm excursion
- Absence of lung sliding on one side - suggests mainstem intubation
5. Tracheal Sizing and ETT Selection
Miller's Anesthesia (10e) notes: "POCUS can help determine size of trachea and endotracheal tube, accurately locate cricothyroid membrane, and improves success of procedures like cricothyrotomy, tracheal rings for percutaneous tracheostomy."
Ultrasound measurement of the subglottic transverse diameter allows appropriate ETT size selection, particularly important in:
- Pediatric patients - where cuffed vs. uncuffed tube selection and tube size is critical
- Post-intubation cuff pressure assessment - the cuff can be visualized as a fluid-filled structure distending within the tracheal lumen
6. Gastric Content Assessment (Aspiration Risk)
Though not airway anatomy per se, gastric ultrasound is an important pre-intubation tool to stratify aspiration risk - especially relevant in emergency cases where fasting history is unclear.
The gastric antrum is scanned in the right lateral decubitus position using a curvilinear probe. The antrum appears as a target-like structure adjacent to the liver:
- Empty antrum (flat, collapsed walls) - low aspiration risk
- Clear fluid (anechoic contents) - moderate risk; volume can be estimated
- Solid contents (heterogeneous, hyperechoic) - high aspiration risk; RSI and precautions indicated
Barash's Clinical Anesthesia notes that point-of-care gastric ultrasound has been used to evaluate gastric emptying times, with recent pediatric studies showing clear fluid emptying in under 1 hour, informing institutional fasting guideline modifications.
7. Supplementary Uses - Lung/Thoracic Ultrasound
In the post-intubation period and for airway decision-making:
| Finding | Significance |
|---|---|
| Lung sliding present, bilateral | Tracheal intubation, bilateral ventilation confirmed |
| Absent lung sliding, unilateral | Mainstem intubation or pneumothorax |
| B-lines (comet-tail artifacts) | Pulmonary edema, may influence airway/ventilation strategy |
| "Barcode sign" (M-mode) | Pneumothorax - guides need for decompression before or after intubation |
| Absent lung sliding + lung point | Pneumothorax - locates the transition zone |
These findings from E-FAST (Extended Focused Assessment with Sonography in Trauma) are now part of standard critical care airway evaluation.
Summary Table - Ultrasound Applications in Airway Management
| Application | Probe | View | Key Finding |
|---|---|---|---|
| Anatomical landmarks | Linear (7-15 MHz) | Transverse/sagittal | Trachea, thyroid, esophagus |
| CTM identification | Linear | Sagittal midline | Gap between thyroid/cricoid |
| Difficult airway prediction | Linear | Sagittal at thyroid | Pretracheal fat thickness |
| ETT confirmation (tracheal) | Linear | Transverse suprasternal | Tube motion in trachea |
| Esophageal intubation exclusion | Linear | Transverse | Double tube sign lateral to trachea |
| Right mainstem exclusion | Linear | Bilateral anterior chest | Bilateral lung sliding |
| Pneumothorax | Linear | Anterior chest | Absent sliding, lung point |
| Gastric content/aspiration risk | Curvilinear | Right lateral decubitus | Antrum contents |
| ETT/trachea sizing | Linear | Transverse subglottic | Transverse diameter measurement |
| Percutaneous tracheostomy | Linear | Sagittal/transverse | Tracheal ring identification |
Key Clinical Points
- Ultrasound is best used as an adjunct to - not a replacement for - clinical assessment and capnography
- Real-time ultrasound during laryngoscopy allows the operator to watch the ETT pass into the trachea via a transverse neck view, providing near-instantaneous confirmation
- In cardiac arrest, capnography is unreliable due to low pulmonary blood flow; ultrasound is especially valuable here
- CTM identification by ultrasound should be performed pre-emptively in anticipated difficult airways (obese, female, short neck) before the airway is instrumented
- The entire airway ultrasound examination can be performed in under 2 minutes with practice, making it suitable for emergency scenarios
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Barash, Cullen & Stoelting's Clinical Anesthesia, 9e | Miller's Anesthesia, 10e | Tintinalli's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Rosen's Emergency Medicine | Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.